Within the last two decades, transcatheter aortic valve replacement (TAVR) has transformed the treatment strategy for symptomatic severe aortic stenosis (AS), representing a less invasive alternative to traditional open-chest surgery. With time, advances in device features, imaging planning, and implantation techniques have contributed to an improvement in safety as well as a reduction in procedural complications. This has led to the expansion of TAVR to lower-risk patients, where TAVR has shown favorable outcomes compared to surgical aortic valve replacement (SAVR). As TAVR expands to younger and lower-risk patients with longer life expectancies, the need for reintervention for failing transcatheter heart valves is expected to increase. Redo-TAVR has gained increasing relevance in the lifetime management of AS as one of the treatment strategies available for structural valve dysfunction (SVD).
1. Introduction
Originally described by Cribier in 2002 [
1], transcatheter aortic valve replacement (TAVR) has since proven to be a safe, effective solution for replacing the aortic valve throughout the full spectrum of surgical risk patients with severe aortic stenosis [
2,
3,
4]. Current data show that since its approval by the Food and Drug Administration (FDA) as an alternative to SAVR for high (2012), moderate (2016), and low (2019) surgical risk patients, TAVR has been established as a therapy with high adherence by physicians and patients, outpacing the volume of all forms of SAVR [
5].
As TAVR expands to younger and lower risk patients with longer life expectancies, the need for reintervention for failing transcatheter heart valves (THV) is expected to increase. Over time, several efforts have been made to mitigate procedural risks, with the aim of maximizing its durability. Currently, Redo-TAVR provides acceptable results in terms of safety and efficacy, but it does come with some unavoidable procedural risks that cannot be neglected [
6].
2. Bioprosthetic Valve Dysfunction and Structural Valve Deterioration Definitions
The Valve Academic Research Consortium (VARC) published its most recent updates in response to the exponential growth in the number of transcatheter and surgical aortic valve interventions in order to standardize clinical endpoints for both procedures [
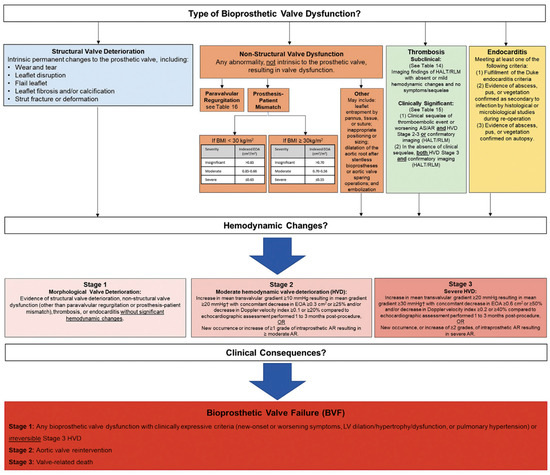
7]. Bioprosthetic Valve Dysfunction (BVD) and Structural Valve Deterioration (SVD) were included as novel endpoints in the VARC-3 document (
Figure 1). BVD was subcategorized into four groups: structural valve deterioration (the dysfunction is related to an intrinsic permanent change in the prosthetic valve, such as wear and tear, leaflet disruption, flail leaflet, leaflet fibrosis and/or calcification and strut fracture), non-structural valve dysfunction (such as paravalvular regurgitation, prosthesis-patient mismatch, leaflet entrapment by pannus, tissue or suture, inappropriate positioning, or sizing), thrombosis, and endocarditis. Three stages of BVD were proposed according to hemodynamic changes: Stage 1: morphological valve deterioration, where no hemodynamic change is present; Stage 2: moderate hemodynamic deterioration; and Stage 3: severe hemodynamic valve deterioration.
Figure 1. Bioprosthetic Valve Dysfunction and Bioprosthetic Valve Failure definitions according to VARC-3 criteria.
From Valve Academic Research Consortium 3: Updated Endpoint Definitions for Aortic Valve Clinical Research. J. Am. Coll. Cardiol. 2020, 76, 2492–2516 [
7]. Permission to reprint obtained.
The definition of bioprosthetic valve failure (BVF) included in this document states that this is a patient-oriented clinical endpoint that considers relevant and clinically meaningful consequences of BVD, including stage 3 hemodynamic valve degeneration and irreversible changes in hemodynamics as a result of SVD, as well as clinical symptoms and sequelae, including valve-related death and re-intervention (either surgical or transcatheter).
3. TAVR Explantation
Prosthesis failure mechanism, patient’s anatomical characteristics, age, comorbidities, and life expectancy are among the factors that should be considered when deciding what is the best alternative for a failed transcatheter bioprosthetic valve.
TAVR explantation consists of surgically removing a transcatheter aortic valve device from the patient’s body. It requires a skilled surgical team and is associated with an increased risk of complications. Nevertheless, for selected patients, this may be the strategy of choice as a second intervention. Data from the multicenter, international EXPLANT-TAVR registry reported elevated mortality and stroke rates regardless of the procedure’s timing and primary indication for TAVR explantation [
8]. According to that study, after one year, the overall mortality rate was 28.5% and the stroke rate was 18.7%. Up to 63% of patients undergoing THV explantation needed concomitant procedures, such as aortic repair, mitral or tricuspid interventions, or coronary artery bypass grafting [
9,
10].
In terms of device type, 30-day mortality and need for any concomitant cardiac procedures at the time of TAVR explant were comparable between self- (SEV) and balloon-expandable (BEV) valves, with a higher rate of ascending aortic repair related to self-expandable devices (22% vs. 9%;
p < 0.001) [
9].
Newly released results from the EXPLANTORREDO-TAVR registry, including 542 patients from 29 centers who underwent TAVR reintervention (TAVR-explant or Redo-TAVR) due to THV failure, suggested that neither the mechanism of degeneration (SVD or non-SVD) nor the device design (BEV or SEV) significantly impacted mortality after TAVR reintervention [
11].
As for outcomes of TAVR explant versus aortic root replacement after failed TAVR, overall survival at a mean follow-up of 6.9 months was 81.2%, with no differences in in-hospital, 30-day, and 1-year stroke and mortality rates between the two groups [
12].
4. TAVR-in-TAVR: Procedural Complications
Coronary Obstruction
Coronary artery disease is one of the most frequent comorbidities among TAVR candidates and the optimal management in this population still lacks definitive data [
19]. A few scenarios are supported by current guidelines for percutaneous coronary intervention (PCI) in patients undergoing TAVR; however, the level of evidence is limited, and the recommendation is only moderately strong [
20]. Meanwhile, recent evidence showed no benefit in short- or mid-term mortality with routine PCI pre-TAVR, with a trend towards an increased risk for bleeding events [
21,
22].
Data from a multicenter registry indicate a rate of 0.9% of unplanned percutaneous coronary revascularization after TAVR [
23]. This number is expected to increase given the implantation of THV in patients with lower surgical risk, and a relatively younger population. Although registries report high success rates of coronary cannulation in patients with acute coronary syndromes and THVs [
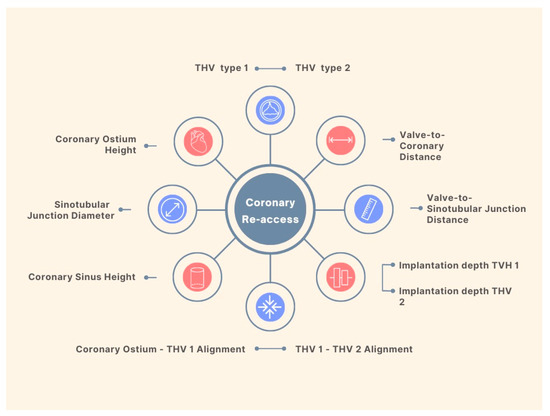
24], the feasibility of coronary access after a Redo-TAVR remains a big concern. Factors impacting coronary re-access after Redo-TAVR procedures are summarized in
Figure 2.
Figure 2. Factors Influencing Coronary Re-Access Following Redo-TAVR.
Researchers compiled CT scans from patients who had undergone TAVR and the findings indicated that, among those with CoreValve/Evolut and Sapien valves, 90% and 67% respectively had coronary arteries positioned below the top of the neoskirt. The risk for technically impossible coronary access was 27% and 10% in CoreValve/Evolut-first and SAPIEN-first cases, respectively [
25].
Detailed analysis of the first TAVR is of utmost importance in planning the second procedure. Knowing the patient’s anatomical characteristics and device type allows the assistant team to anticipate potential challenges such as sinus of Valsalva sequestration and coronary obstruction.
A recent benchtop study evaluated 38 combinations of 5 valve designs (Sapien3, Evolut Pro, Acurate Neo, and Portico in Sapien XT or Evolut R) in order to evaluate neoskirt and implant heights, and their influence on coronary re-access. Taller implants were associated with larger neoskirts in THVs such as Evolut R and Acurate, with the Evolut-in-Evolut combination responsible for the highest value (31.6 mm) [
26].
The choice of the second valve (supra or intra-annular design, balloon or self-expanding) is certainly a critical point in Redo-TAVR. To date, there are no formal guidelines that indicate or contraindicate combinations of devices. Anatomical and post-first TAVR characteristics must be combined with the patient’s profile, the expertise of the medical team, and the resources available at the center.
Although TAVR is proven to be an effective treatment in bicuspid aortic valve disease, there are limited data on Redo-TAVR in these patients [
27,
28]. Based on CT scans, a study found that the risk of coronary obstruction during Redo-TAVR was comparable between tricuspid and bicuspid type 1 aortic valves, while it was significantly lower in type 0 bicuspid aortic valves [
29].
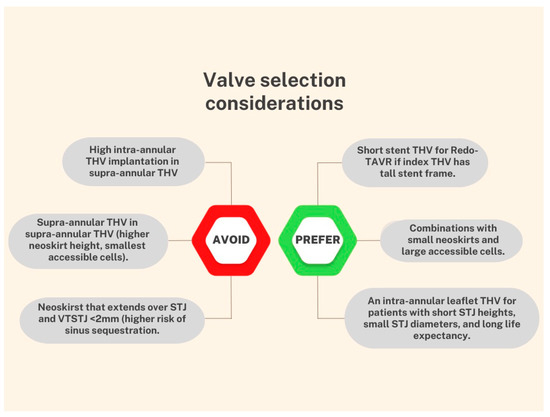
The local heart team plays a crucial role in the decision-making process, and it is essential to anticipate potential complications in advance. The selection of the valve and the associated procedural strategy must be tailored on a case-by-case basis. Based on the available data, some suggestions for device combinations are shown in Figure 3.
Figure 3. Considerations for choosing a device combination.
This entry is adapted from the peer-reviewed paper 10.3390/jcm12144788