Decellularized extracellular matrix (dECM) is a promising biomaterial for repairing periodontal defects since dECM maximizes the retention of complex protein arrays, glycosaminoglycans, proteoglycans, and many other matrix components found in natural tissues [
1]. Therefore, dECM provides optimal cell–ECM interactions by providing ideal biological clues to mimic native signaling events to promote the regeneration, repair, and remodeling of damaged periodontal tissue [
2]. For instance, with a three-dimensional network providing a microenvironment to maintain homeostasis, support stem cell ingrowth, promote tissue formation, and initiate tissue repair, dECM has been successful in the regeneration and repair of many tissues, such as heart, nerve, and liver tissues [
3]. During tissue regeneration, cell–ECM interactions coordinated with ECM component changes are vital for directing cell behaviors, functions, and fates, resulting in tissue repair and remodeling, which are regulated by specific enzymes produced by cells [
3].
2. dECM Derived from Different Sources
As a promising biomaterial, dECM has been widely applied in periodontal tissue engineering. Natural ECM generated from decellularized ECM (dECM) can be divided into two groups as decellularized cells/cell sheets (C-dECM) or decellularized tissue-specific ECM (T-dECM) according to the origins.
2.1. (Stem) Cell-Derived dECM (Decellularized Cell Sheet)
Significant efforts have been made to improve the quality and efficiency of the generation of cell-derived ECM with 3D structure. Part of these works involve harvesting cell-derived dECM membranes and then fabricating a 3D scaffold using various physical and chemical techniques [
5]. As shown in
Figure 1, C-dECM-laden scaffolds possess superior biological elasticity and porosity and allow more efficient nutrient exchange that favor cell proliferation, adhesion, and differentiation [
6].
In recent years, scientists have applied certain decellularized cell sheets to periodontal regeneration. Decellularized cell sheet techniques refer to the effective removal of cellular and nuclear components of the cell sheet, especially DNA and RNA, while retaining the basic components, biological activity, and mechanical integrity of the extracellular matrix (dECM) of the sheet. Due to the lack of cells and major tissue structure, the foreign body reaction and immune rejection are significantly reduced or even absent in the cell sheet-derived dECM material, while the original three-dimensional structure, mechanical integrity, biological activity, and good biocompatibility are well preserved. Therefore, the use of decellularized sheets in regenerative medicine is increasing.
Moreover, decellularized membrane sheets combined with cytokines or new materials to achieve better tissue regeneration effects have been used in many tissue regeneration processes, such as dental tissue regeneration [
7], bone regeneration [
8], vascular reconstruction [
9], nerve regeneration [
10], and corneal regeneration [
11]. Specifically, the common C-dECM sources for periodontal regeneration are the periodontal ligament stem cell sheet (PDLSC sheet) [
12], the bone marrow mesenchymal stem cell sheet (BMSC sheet) [
6], the human urogenic mesenchymal stem cell sheet (hUMSC sheet), and others such as dental folicle stem cells and L929 sheet-derived dECM can also be considered.
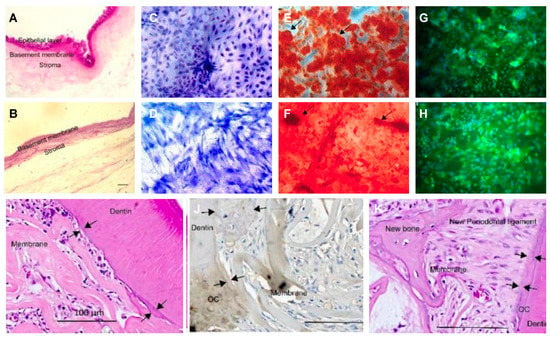
Figure 1. Decellularized amniotic membrane promotes osteogenic differentiation and cementum regeneration both in vitro and in vivo. Histological cross-sections of fresh (A) and decellularized (B) amniotic membrane. Representative areas of adipose-derived stromal cell cultures on polystyrene (C,E,G) and decellularized amniotic membrane (DAM) (D,F,H). ASCs confluence in the presence of supplemented medium (C,D). The osteoinduction medium stimulated the deposition of the mineralized extracellular matrix, which was observed as red calcified deposits (arrows). Osteopontin expression was evidenced by green fluorescence as agglomerates on polystyrene (G) and a diffuse distribution (H) on DAM. (I,J) and exposed old cementum (J,K), as well as a thin acellular cementum layer and thick cellular cementum (J). Transplantation of decellularized amniotic membrane (DAM) (I); DAM associated with extracellular matrix and undifferentiated adipose-derived stromal cells (J); scale bars of 100µm (I–K).
- (1)
-
Periodontal ligament (stem) cell sheets
The biological properties of human periodontal membranes were evaluated in vitro by Jiang et al. [
7]. Decellularized PDLC sheets maintain an intact extracellular matrix structure, and the expression or distribution of type I collagen and fibronectin was similar in decellularized PDLC sheets and natural PDLC sheets, which contributes to the recellularization procedures and retaining the osteogenic potential of allogeneic human periodontal ligament stem cells. Four weeks after surgery, newly formed bone, cementum, and periodontal membranes were observed with a decellularized PDLC sheet combined with 15-Deoxy-Δ (12,14)-prostaglandin J (2) nanoparticles. Thus, it is believed that hPDLC sheets may be a potential extracellular matrix source for periodontal regeneration in the oral inflammatory environment. In addition, other results also indicate that decellularized sheets derived from PDLSC can improve the proliferation and differentiation of mesenchymal stem cells, thus performing regenerative potential in the future of periodontal tissue engineering [
12,
14]. Moreover, PDLSC sheet-derived dECM is believed to preserve growth factors, such as fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), and hepatocyte growth factor (HGF) [
14].
- (2)
-
BMC/BMSC sheet:
The 14-day BMSC sheets cultured in vitro significantly promoted osteogenesis of bone marrow stem cells compared with counterparts by Xu et al. Proteomic analysis showed that the extracellular matrix components of the cell sheet varied over time. Type IV collagen chains in 14-day dECM were higher than those in other membranes and more able to promote osteogenic differentiation of BMSCs [
15]. Type IV collagen was significantly enriched in the activated focal adhesion kinase/phosphatidylinositol-4,5-diphosphate 3-kinase/protein kinase B signaling pathway (FAK/PI3K/AKT). Thus, 14-day dECM with a high content of type IV collagen chain enrichment that could promote osteogenic differentiation of BMSCs may be related to the activation of the FAK/PI3K/AKT signaling pathways [
4].
- (3)
-
Urogenic mesenchymal (stem) cell sheets:
Yang et al. found that the conditioned medium of hUMSC contained components that could promote cementum differentiation [
16]. Xiong et al. seeded human UMSCs on plates and induced the extracellular matrix generation, followed by decellularized processing, leaving the extracellular matrix components on the dishes. Using decellularized hPDLSC sheets and fibronectin-coated plates as controls, hUMSCs had more fibronectin components than hPDLSCs, which better promoted the proliferation, adhesion, and osteogenic differentiation of hPDLSCs [
17].
Many studies have raised the question of whether dECM derived from different cell types has different effects on cell growth. Hoshiba et al. studied dECM extracted chemically or enzymatically from chondrocytes produced from chondrocytes, fibroblasts, and bone marrow mesenchymal stem cells and investigated their effects on articular chondrocyte behavior [
18]. ECM derived from chemical methods is significantly superior to enzymatic methods in cell adhesion, and the number of chondrocytes adhering to chondrocyte-derived ECM is significantly higher than that of fibroblast or mesenchymal stem cell-derived ECM. ECM generated from the same cell lineage as the target tissue has been shown to provide a more appropriate microenvironment for cell growth because of unique molecules and pores of appropriate size, which also promote cell reinoculation and cell adhesion [
18].
C-dECMs are usually harvested after decellularization of cell sheets constructed in vitro for a few weeks. The cell-sheet technique allows target cells to reproduce in large amounts and harvest enough C-dECM for clinical use since ECM is the major component of the cell sheet while cells, especially stem cells, could proliferate indefinitely. Acquiring C-dECM, especially for obtaining dECM from certain progenitors or stem cells, is relatively simpler when compared to the sophisticated fabrication of tissue-like dECM [
19]. Moreover, C-dECMs have an advantage of safety since in vitro cell expansion can reduce the risk of pathogen transfer caused by allogenic ECM and avoid adverse host immune responses induced by xenogeneic ECM. Furthermore, in-vitro cultured cell-derived dECM can be more operable to modify, such as when cocultured with osteogenic inducers to harvest mineralized C-dECM or to graft on other surfaces of biomaterials [
20], such as treated dentin matrix, hydroxyapatite, and biphasic calcium phosphate, to form another excellent periodontal tissue engineering construct [
21].
Although C-dECMs could help to provide a microenvironment with the help of omplicated manufacturing for relative tissue regeneration, reconstructing the natural 3D architecture of the whole organ or tissue in the laboratory is now unrealistic [
22].
Therefore, C-dECM couldn’t perfectly mimic the sophisticated ECM structure and interior architecture, such as the porous structure and the collagen fiber arrangement, which might have an effect on cell adhesion, proliferation, and differentiation [
23]. Furthermore, the mechanical properties and microenvironment conditions of cell-deposited ECM are different from those of native ECM. Unlike allogenic T-dECMs serving as reservoirs for site-specific bioactive molecules, C-dECM was believed to be inferior in preserving tissue niches for tissue regeneration when compared with T-dECM [
12,
24,
25].
2.2. Tissue-Derived Extracellular Matrix for Periodontal Tissue Engineering Constructs
Despite the similar ECM composition between different tissues and organs, subtle differences in function, proportion, structure, and stiffness of the ECM can influence the interaction of cells in determining cell fate (
Figure 2). Tissue dECM can promote tissue-specific and non-tissue-specific stem cells/progenitor cells, primary cell proliferation, and serve as a tissue-specific scaffold for stem cells/progenitor cells. Even without a specific differentiation mediator, the stem cells or progenitor cells still have the corresponding cell lineage differentiation capacity, based on the specific interaction between the cell and the ECM [
28].
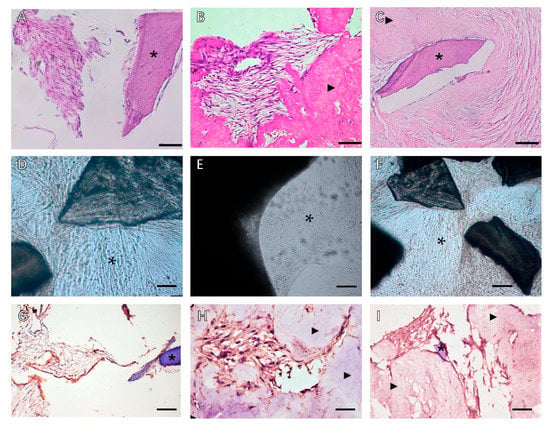
Figure 2. Phase contrast microscopy of decellularized scaffolds cultured with periodontal cells in 3D culture for 14 days. Scale bars, 200 µm in (
A–
C): (
A) PDLSCs around the T-dECM; (
B) periosteum stem cells (PSCs) around and in the dPDL; (
C) PDLSCs + PSCs around the T-dECM and in the dPDL. The asterisk indicates the monolayer of the cells. Histological sections of decellularized scaffolds were cultured with periodontal cells in 3D culture for 14 days. Hematoxylin-eosin staining. Scale bars, 100 µm in (
D), 50 µm in (
E,
F): *: PDLSCs next to the dTM indicated by an asterisk; (
E) PSCs in the dPDL (
F) PDLSCs + PSCs around the T-dECM and in the dPDL (
D) original magnification ×200; (
E,
F) original magnification ×100. Evaluation of the expression of osteogenic differentiation markers in periodontal cells cultured on decellularized scaffolds under 3D culture for 14 days: (
G–
I) Immunohistochemical staining. The positive cells have a brown color. The nuclei were counterstained with hematoxylin. Scale bars, 100 µm in (
G–
I): (
G) OPN staining of PDLSCs next to the T-dECM indicated by an asterisk; (
H) OC staining of PSCs in the dPDL indicated by arrowheads; (
I) OPN staining of PDLSCs + PSCs around the T-dECM and in the dPDL indicated by an asterisk and arrowheads, respectively. *: MSCs around T-dECM(dTM);

: MSCs around T-dECM(dPDL).
2.2.1. Human (Allogenic) Tissue Derived dECMs
- (1)
-
Dental (craniofacial)-related human tissues derived dECM
To achieve the goal of complete periodontal regeneration, many studies have evaluated the effectiveness of decellularized tissue derived from human tooth-related tissue for tissue engineering. Hyoju Son et al. [
30] applied sodium dodecyl sulfate and Triton X-100 separately to treat tooth slices harvested from healthy human third molars, which was verified to efficiently remove nuclear components and maintain intact structure and composition of dECM. Furthermore, T-dECMs can support the regeneration of PDLSCs in the vicinity of cementum and express cementum-related and PDL-related genes. These results indicated that the dentin dECM promoted proliferation and differentiation of MSCs, thus having regenerative potential in future tissue engineering for periodontal regeneration.
The human tooth dECM has also been demonstrated to promote the differentiation of PDLSC, as proved by Ik-Hwan Kim et al. [
31]. The cementum/PDL-anchored structures can be regenerated after PDLSC migration as expected, which suggests that decellularized human tooth material may serve as a biological scaffold for PDLSC loading as a novel therapeutic approach for periodontal defects.
As for the complicated composition of different human-derived tissues dECM and the related functions, they vary from type to type. Dental tissue engineering approaches make it easier to solve this problem with dECM constructs generated from tissues derived from the same origin as extraembryonic mesoderm, which are believed to have more bioactive molecules naturally. Dental-derived tissue dECM has been widely used to promote dental tissue repair and has achieved great success [
32,
33,
34].
- (2)
-
Non-dental-related tissue-derived dECM
- a.
-
Human amnion dECM
Decellularized human amnion has been adopted as a soft tissue replacement and a delivery system for stem cells. Dilcele Silva Moreira Dziedzic et al. applied the decellularized amnion infiltrated by adipose mesenchymal stem cells (ADSCs) with mineralized extracellular matrix to a rat periodontal root bifurcation lesion model [
13]. After being treated with the decellularized amnion/ADSCs/mineralized ECM, periodontal healing was assessed by micro-CT and histological analysis when compared with untreated defects. Decellularized amniotic membranes with or without ADSCs promoted bone healing compared with controls. What’s more, it has also been observed that human-derived decellularized amniotic membranes enhanced periodontal tissue formation in PDLSC defects [
35]. The effects of human decellularized amnion on periodontal regeneration were widely explored and showed great clinical translational potential, as a number of randomized controlled treatments proved [
36,
37,
38,
39].
- b.
-
Human umbilical vein dECM
Allogenic “scaffolds” derived from the human umbilical veins (HUVs) were fabricated, and the biological and mechanical properties during early remodeling events were examined. Human umbilical vein-derived dECM harvested by the osmotic lysis method displayed increased cellular proliferation and reduced metabolic activity compared to HUVs treated with surfactant. Biomechanical properties were largely preserved and similar when subjected to different treatments, and the results suggest that by optimizing processing conditions, biological events associated with remodeling can be modulated to tailor function for specific clinical applications. 3D dECM derived from the HUVs has potential for functioning as a regenerative matrix for tissue regeneration with ideal biomechanical properties [
40]. Allogenic dECM derived from the human umbilical vein [
41] were proved to have ideal biological behavior in promoting proliferation and reducing metabolic activity in mesenchymal-derived cells. The specific structure of the vein has the lumenal surface acting as a barrier to inhibit cell migration, while the ablumenal surface promotes cellular invasion at the interface with the wound site [
40].
2.2.2. Heterogenous Tissue-Derived dECMs
- (1)
-
Heterogenous dental (craniofacial)-related tissues derived from dECM
- a.
-
Decellularized porcine dental matrix
Han et al. [
42] treated the incisor teeth with the decellularized method to obtain the porcine dental dECM, combined the dECM with the immunomodulator RSG, and evaluated the physical and chemical characteristics of the extracellular matrix and its effects on tissue regeneration. The results showed that the extracellular matrix ensured the proliferation and differentiation of odontogenic stem cells with good immune regulation, antagonizing the classical activation of M1 macrophages. Selective activation of M2 macrophages promoted the regeneration of the ligament-bone interface. At the same time, the tissue-engineered scaffold significantly reduces the absorption of bone around the implant and expresses the protein markers of natural cementum and alveolar bone.
- b.
-
Decellularized matrix of dog periodontal ligament
The effect of dog periodontal acellular matrix on periodontal healing was evaluated by Lee et al. [
43]. The mandibular premolars from six beagles were either untreated, decellularized, or treated with root planning before being reimplanted into the extraction site. A chemistry method could satisfy the need for PDL decellularization, as confirmed by cytological, histological, SEM, and TEM analysis. After 8 weeks, both the untreated PDL group and the decellularized PDL group supported periodontal reattachment (especially cementum formation) to some extent at the extraction site. More periodontal regeneration was seen in the decellularized periodontal tissue group than in the teeth in the root planning group.
- c.
-
Decellularized rat mandible matrix
Naoko Nakamura et al. [
44] prepared rat mandible matrix with high pressure perfusion, DNA enzyme, and detergent and evaluated the reconstruction of periodontal structure as periodontal matrix in vivo. After tooth extraction, the decellularized mandible with periodontal matrix was implanted into a rat kidney capsule, and the host cells were observed to migrate into the periodontal matrix and align along the collagen fibers of the periodontal membrane, demonstrating that the decellularized mandibular matrix can reconstruct periodontal tissue by controlling host cell migration and can be used as a novel periodontal therapy.
- (2)
-
Heterogenous, non-dental-related tissue-derived dECM
Solid dECM from non-dental-related tissue sources has recently been studied for periodontal defect regeneration due to its rich resources, economic benefit, massive production, and usually harvesting from discarded tissue, such as treated porcine small intestinal submucosa (SIS) and the extracellular matrix of amnion and pericardium.
- a.
-
SIS
SIS is one of the most commonly used decellularized tissues, with good potential for soft tissue repair and regeneration, but it lacks sufficient mechanical properties to guide bone tissue regeneration unless properly modified. Gu et al. used the pig small intestinal submucosal tissue as a biological collagen membrane for guiding tissue regeneration [
45]. In the rat cranial defect model, the SIS dECM could promote bone tissue regeneration, had a higher bone volume fraction, and regenerated more bone tissue, presenting the potential to promote bone regeneration in periodontal defects.
- b.
-
Decellularized Amnion
Decellularized Amnion is of great biocompatibility and can maintain original tissue structure, support cell attachment, cell infiltration, bone deposition, and periodontal regeneration [
46]. The amniotic membrane from various species were used to regenerate craniofacial bone by a few scientists [
47]. The amniotic membrane contains collagen type I, which helps improve the formation and strength of the bone, and this instinctive property makes it ideal for tissue regeneration procedures.
- c.
-
Decellularized pericardium
Serena Bianchi et al. introduced the decellularized bovine pericardium as a membrane material loading PDLSCs [
48]. The decellularized bovine pericardiums retained the three-dimensional collagen structure for stem cell infiltration. hPDL fibroblasts were seeded on the decellularized bovine pericardium and were healthy, large, and polygonal with filopodia and lamellipodia. Other results show that cells migrate along and within the membrane layer, binding to membrane fibers by filamentous extension, showing that decellularized bovine pericardium could serve as a carrier for PDL fibroblasts [
48].
The porcine pericardium [
49,
50] is also a commonly used material for periodontal ligament regeneration, and Mika Suzuki et al. [
41] verified the important role of the decellularized pericardium in promoting periodontal ligament structural remodeling and promoted the gradient mineralization of the decellularized pericardial surface to promote the formation of ligamento-structure at the soft and hard tissue interface. Rabbit pericardial tissue [
47] has been used to restore craniofacial bone defects, and the decellularized rabbit pericardial was believed to facilitate bone regeneration by inhibiting connective tissue invasion.
- d.
-
To sum up, decellularization of natural tissues to produce extracellular matrix is a promising method for 3D scaffolding and for investigating cell-ECM interaction during regeneration of target tissue [
3,
51]. The fate and behavior of mesenchymal stem cells are influenced by the stem cell niches ideal biochemical and physical cues. Ana Rita Pereira et al. compared the biological behaviors of BMSCs when exposed to C-dECM and T-dECM, and better outcomes were observed in 3D decellularized bone tissue for greater architecture complexity and physicochemical properties [
52]. To sum up, tissue-derived dECM has great potential in the context of endogenous periodontal regeneration, with a better effect on preserving the tissue niche intended for different tissues in periodontal defects.