Hematopoietic cell transplant (HCT), used for treatment of many malignant and non-malignant pediatric diseases, is associated with serious complications, limiting this therapy’s benefit. Acute kidney injury (AKI), seen often after HCT, can occur at different stages of the transplant process and contributes to morbidity and mortality after HCT. The etiology of AKI is often multifactorial, including kidney hypo-perfusion, nephrotoxicity from immunosuppressive and antimicrobial agents, and other transplant-related complications such as transplant-associated thrombotic microangiopathy and sinusoidal obstructive syndrome. Early recognition of AKI is crucial to prevent further AKI and associated complications. Initial management includes identifying the etiology of AKI, preventing further kidney hypo-perfusion, adjusting nephrotoxic medications, and preventing fluid overload. Some patients will require further support with kidney replacement therapy to manage fluid overload and AKI.
1. Acute Kidney Injury
AKI is a relatively common complication after HCT, with a reported incidence rate of 21–84% [
1,
2]. Common risk factors for kidney injury include myeloablative conditioning, older age, acute GVHD, and SOS. Satwani et al. observed a significant increase in the incidence of kidney injury in children who received myeloablative conditioning versus reduced intensity conditioning (45.7% and 17.1% respectively) [
6]. In addition to its contribution to a higher rate of mortality, previous AKI predisposes patients to chronic kidney disease (CKD). In a cohort of 158 adult allogeneic HCT survivors, the risk of CKD ≥ stage 3 was approximately 10-fold higher in patients in whom AKI developed following HCT [
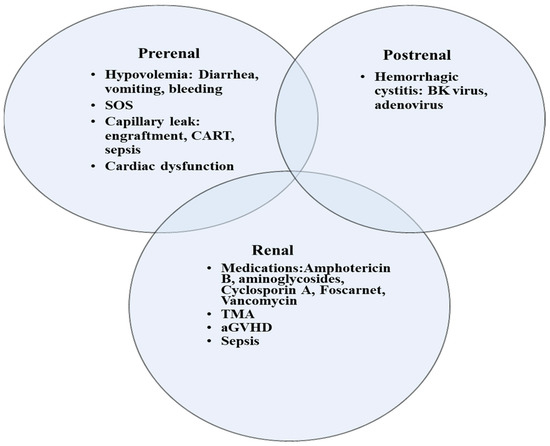
13]. AKI is encountered at any stage in the transplant process, although often at the earlier stages. Early in the pre-transplant phase, many children receive myeloablative conditioning regimen with or without total body irradiation (TBI) that can induce kidney injury. Shortly after transplant, nephrotoxic immunosuppressive medications such as calcineurin inhibitors are given to mitigate the risk of GVHD. In addition, children are at a higher risk of infection and subsequent sepsis due to their immune-compromised status. In many instances, the etiology of AKI is multifactorial and includes hypoperfusion in the setting of capillary leak or sepsis resulting in acute tubular necrosis, drug induced nephrotoxicity, thrombotic microangiopathy (TMA), and sinusoidal obstruction syndrome (SOS) (
Figure 1) [
1]. Drug induced nephrotoxicity is relatively common in HCT patients. Antimicrobials that are often used to treat infections post HCT such as aminoglycoside, vancomycin, or amphotericin can induce direct kidney injury. Nephrotoxicity is also encountered with calcineurin inhibitors such as cyclosporin or tacrolimus that can cause kidney arteriolar vasoconstriction via activation of the renin–angiotensin–aldosterone system [
14]. In addition, calcineurin inhibitors may trigger endothelial injury and subsequent TMA [
15]. Moreover, kidneys can be a target of GVHD, although less described than other organs like skin, liver, and lungs. Kidney injury related to GVHD is mediated by donor T-cells as well as proinflammatory cytokines. Kidney GVHD can present as AKI, nephrotic syndrome, glomerulonephritis, and TMA [
16]. However, the most common presentation is nephrotic syndrome with a high degree of proteinuria, hypoalbuminemia, and edema. Hemorrhagic cystitis can cause obstructive kidney injury when clots in the bladder obstruct the outflow tract. The etiology of hemorrhagic cystitis is usually multifactorial, but often encountered with the use of cyclophosphamide or in the context of reactivation of virus infections such as BK virus, adenovirus, and cytomegalovirus. Treatment include hyperhydration, diuresis, and bladder irrigation with a three-way bladder catheter.
Figure 1. Etiologies of AKI in children following HCT. SOS, sinusoidal obstructive syndrome; TMA, thrombotic microangiopathy; aGVHD, acute graft versus host disease; CART, Chimeric antigen receptor (CAR) T-cell therapy.
3. Special Disease Conditions Post HCT That Are Associated with AKI
3.1. Transplant-Associated Thrombotic Microangiopathy
Transplant-associated thrombotic microangiopathy (TA-TMA) is a life-threatening complication that is encountered early in the post-HCT phase. The incidence of TA-TMA in children is 16%, with a median onset of 47 days post-transplant [
18]. Risk factors for TA-TMA include acute GVHD, infectious process (especially viral), mismatched donor, multiple HCTs, and myeloablative conditioning [
18]. The pathophysiology of TA-TMA involves an initial endothelial injury triggered by factors such as chemotherapy or infection that results in an increase in the proinflammatory cytokines, procoagulant factors, and soluble adhesion molecules. This combination promotes further endothelial injury and initiates and propagates the complement cascade, resulting in platelet aggregation, fibrin deposition, and microthrombi formation.
Eculizumab is a monoclonal antibody against the complement component C5, which blocks the formation of the membrane attack complex (MAC or C5b-9) and thus prevents endothelial damage. In a cohort of 64 pediatric HCT patients with high-risk TA-TMA and multiorgan dysfunction, the survival rate improved dramatically with the use of eculizumab (66% in 1-year post HCT in treated vs 16.7% in a previously reported untreated cohort) [
22].
3.2. Sinusoidal Obstruction Syndrome
Sinusoidal obstruction syndrome (SOS) is associated with multiorgan dysfunction and a high mortality rate [
23]. SOS occurs in the early stage post HCT secondary to cytotoxic therapy or radiotherapy [
24]. The incidence rate is 20–60%. Diagnosis of SOS is based on the following criteria (two or more criteria present) [
25]:
-
Consumptive and transfusion-refractory thrombocytopenia;
-
Weight gain on 3 consecutive days despite the use of diuretics, or a weight gain of >5% above baseline weight within 72 h;
-
Increase in bilirubin from baseline on 3 consecutive days, or bilirubin ≥ 2 mg/dL within 72 h;
-
Hepatomegaly (best if supported by imaging) above baseline value;
-
Ascites (best if supported by imaging) above baseline.
Kidney injury in SOS is attributed to hypoperfusion and vasoconstriction and is associated with fluid overload. Managing the kidney injury requires fluid restriction and use of diuretics to reduce fluid overload. Renal replacement therapy may be necessary if fluid overload persists, and urine output remains inadequate despite diuretic treatment [
26].
3.3. Fluid Overload
Fluid overload (FO) is common in critically ill children and negatively affects outcome [
29,
30]. Additionally, FO can exacerbate kidney injury by worsening kidney venous hypertension, impairing perfusion pressure capacity of the glomerular capillaries. Cumulative fluid balance is often used interchangeably with fluid overload and is calculated as follows: Fluid intake – Fluid output (L)/ICU admission weight (kg) × 100 [
31]. FO can also be calculated by comparing current weight to admission weight if fluid balance information is not available. FO > 10% is common in critically ill children and was observed in 33% of a large cohort of 1017 critically ill children [
29]. FO was associated with higher risk of mortality, kidney adverse events, and increased duration of mechanical ventilation (MV) and ICU stay. A metanalysis including 44 pediatric studies showed a 6% increase in odds of mortality with each 1% increase in FO [
30]. The adverse effect of FO is also prevalent in the pediatric HCT population [
32,
33].
3.4. CAR T-Cell Therapy
Chimeric antigen receptor (CAR) T-cell therapy, used for treatment of hematologic malignancies, involves the utilization of engineered cytotoxic T-cell to recognize specific tumor antigen. AKI occurs with this therapy secondary to cytokine release syndrome (CRS), a well described complication of this therapy which can lead to organ dysfunction. Hypoperfusion secondary to capillary leak and proinflammatory cytokines contribute to AKI encountered post CAR-T cell therapy. AKI is usually mild in these cases [
36].
4. Continuous Kidney Replacement Therapy
Nearly one-third of patients with AKI require kidney replacement therapy (KRT) [
1]. CKRT is used often in the ICU to deliver KRT because it is tolerated better than intermittent hemodialysis (IHD) in hemodynamically unstable critically ill children. During CKRT, fluid removal and solute clearance occur continuously, promoting better control of fluid status. Solute clearance occurs by either convection, diffusion, or both, whereas fluid is removed via ultrafiltration. Hemofiltration modes of CKRT can increase removal of small and medium-sized solutes by convection (solute drag); in contrast, hemodialysis modes mainly remove small-sized molecules by diffusion (concentration gradient).
No consensus exists on the optimal time for initiation of CKRT and whether early initiation can improve outcome. Most evidence is from adult randomized trials that compared the early initiation of CKRT to using a standard strategy. One of the largest adult trials, the STARRT-AKI trial, randomized 3019 critically ill adults with AKI to either an accelerated RRT strategy (initiated within 12 h in adult critically ill patients with Stage 2 or Stage 3 AKI) or a standard strategy. The accelerated RRT strategy did not reduce mortality compared to the standard strategy, and survivors of the accelerated RRT strategy had a higher risk of adverse events and dependence on kidney replacement therapy [
41]. In contrast, in the ELAIN trial that included 231 critically ill patients with AKI, a lower mortality in the early RRT group compared to the delayed initiation group was observed (39% versus 54% respectively) [
42].
5. Transition from CKRT to IHD/Discontinuation of CKRT
The optimal timing for successful discontinuation of CKRT or switch to IHD is difficult to predict. Renal recovery is usually preceded by an increase in urine output. Urine output > 500 cc/day is used in some adult patients as a criterion to discontinue KRT [
47]. Factors that have been shown to predict successful liberation include the hourly urine output within 12 h before CKRT discontinuation, serum creatinine level within 24 h before liberation, and the cumulative fluid balance (from ICU admission to CKRT discontinuation) [
48]. In general, children are switched from CKRT to IHD when FO is resolved and they are hemodynamically stable.
6. Outcomes of KRT
ICU mortality in children post HCT requiring CKRT is estimated to be 52–65% [
2,
49]. The 1-year overall survival rate is also poor (27.4% (95% CI: 16–40.5%,
p < 0.0001)) [
1]. Reported factors that are associated with mortality include FO > 10%, mechanical ventilation, vasoactive support, and neutropenia at the end of CKRT [
2].
7. Biomarkers of AKI in Children with HCT
Given the potential shortcomings of sCr as a marker of AKI, several additional biomarkers of AKI have been developed and studied. These biomarkers measure either glomerular function or renal tubular damage and can aid in early detection of AKI (Table 3).
Table 3. Biomarkers in AKI.
| Biomarker |
Characteristic |
Detection Time |
Peak |
AUC for AKI Detection |
Limitations |
| Glomerular injury |
| Cystatin C |
13-kDa protein that is present in all nucleated cells, protease inhibitor |
2–48 h |
6–8 h |
|
Influenced by inflammation, muscle mass, and high-dose steroids |
| Renal tubular injury |
| NGAL |
25-kDa protein of the family of lipocalins with bacteriostatic function |
2–24 h |
6–12 h |
0.8 (0.72–0.87) |
False elevation in sepsis and malignancy |
| NAG |
>130-kDa proximal tubular lysosomal enzyme |
2–4 h |
|
0.6 |
Elevated in diabetes and albuminuria |
| KIM 1 |
38.7-kDa type I transmembrane glycoprotein |
1–24 h |
|
0.85 |
Slow rise and non-specific
May be elevated in the settings of chronic proteinuria and inflammatory diseases |
| Interleukin-18 |
24-kDa cytokine |
4–48 h |
12 h |
0.75 |
Low sensitivity/specificity |
| L-FABP |
14-kDa lipid binding protein |
12–72 h |
|
|
May lose its specificity when liver disease is present |
| TIMP 2 |
21-kDa protein, endogenous inhibitor of metalloproteinase activities, involved in G1 cycle arrest |
1–12 h |
|
0.8 |
Proteinuria interferes with the test results
Elevated in diabetes |
| IGFBP7 |
29-kDa protein, IGF-1 receptor antagonist, involved in G1 cycle arrest |
|
|
0.76 |
|
This entry is adapted from the peer-reviewed paper 10.3390/curroncol30030253