Q fever has raised many questions. Coxiella burnetii, the causative agent, is a zoonotic pathogen affecting a wide range of hosts. This airborne organism leads to an obligate, intracellular lifecycle, during which it multiplies in the mononuclear cells of the immune system and in the trophoblasts of the placenta in pregnant females. Although some issues about C. burnetii and its pathogenesis in animals remain unclear, over the years, some experimental studies on Q fever have been conducted in goats given their excretion pattern. Goats play an important role in the epidemiology and economics of C. burnetii infections, also being the focus of several epidemiological studies.Variants of the agent implicated in human long-term disease have been found circulating in goats.
- C. burnetii
- goat
- Q fever
1. Introduction
| Country (Area) | Period | Reference |
|---|---|---|
| Australia | 2012–2014 | [20] |
| Bulgaria | 2004 | [21] |
| 2007–2011 | [22] | |
| China | 2018–2019 | [23] |
| France | - | [24] |
| 2007 | [25] | |
| Newfoundland | 1999 | [26] |
| Slovakia | 1993 | [27] |
| The Netherlands | 2007–2020 | [28,29][28][29] |
| United Kingdom | 1987 | [30] |
| USA | - | [31] |
| 2011 | [32] |
2. Coxiella burnetii: The Microorganism and Its Pathogenesis
3. Infection and Clinical Outcomes in Goats
References
- Derrick, E.H. “Q” fever, a new fever entity: Clinical features, diagnosis and laboratory investigation. Med. J. Aust. 1937, 2, 281–299.
- Davis, G.E.; Cox, H.R.; Parker, R.R.; Dyer, R.E. A Filter-Passing Infectious Agent Isolated from Ticks. Pub. Health Rep. 1938, 53, 2259–2282.
- Bengtson, I.A. Immunological relationships between the rickettsiae of Australian and American “Q” fever. Pub. Health Rep. 1941, 56, 272–281.
- Kaplan, M.M.; Bertagna, P. The geographical distribution of Q fever. Bull. World Health Organ. 1955, 13, 829–860.
- Caminopetros, J.P. La Q-fever en Grece: Le lait source de l’infection pour l’homme et les animaux. Ann. Parasite Paris 1948, 23, 107–118.
- Fox-Lewis, A.; Isteed, K.; Austin, P.; Thompson-Faiva, H.; Wolfgang, J.; Ussher, J.E. A case of imported Q fever in New Zealand. NZMJ 2019, 132, 92–94.
- van den Brom, R.; van Engelen, E.; Roest, H.I.; van der Hoek, W.; Vellema, P. Coxiella burnetii infections in sheep or goats: An opinionated review. Vet. Microbiol. 2015, 181, 119–129.
- World Organisation for Animal Health (WOAH). WAHIS Interface. Available online: https://wahis.woah.org/#/home (accessed on 15 September 2022).
- de Valk, H. Q fever: New insights, still many queries. Eurosurveillance 2012, 17, 20062.
- van Loenhout, J.A.F.; Paget, W.J.; Vercoulen, J.H.; Wijkmans, C.J.; Hautvast, J.L.A.; van der Velden, K. Assessing the long-term health impact of Q-fever in the Netherlands: A prospective cohort study started in 2007 on the largest documented Q-fever outbreak to date. BMC Infect. Dis. 2012, 12, 280.
- Sidi-Boumedine, K.; Rousset, E.; Henning, K.; Ziller, M.; Niemczuck, K.; Roest, H.I.J.; Thiéry, R. Development of harmonised schemes for the monitoring and reporting of Q-fever in animals in the European Union. EFSA Support. Publ. 2010, 7, 48.
- EFSA (European Food Safety Authority). Panel on Animal Health and Welfare (AHAW); Scientific Opinion on Q Fever. EFSA J. 2010, 8, 1595.
- European Centre for Disease Prevention and Control. Risk Assessment on Q Fever—Technical Report; ECDC: Stockholm, Sweden, 2010; p. 40.
- Georgiev, M.; Afonso, A.; Neubauer, H.; Needham, H.; Thiéry, R.; Rodolakis, A.; Roest, J.; Stärk, K.D.; Stegeman, J.A.; Vellema, P.; et al. Q fever in humans and farm animals in four European countries, 1982 to 2010. Eurosurveillance 2013, 18, 20407.
- Farooq, M.; Khan, A.U.; El-Adawy, H.; Mertens-Scholz, K.; Khan, I.; Neubauer, H.; Ho, Y.S. Research Trends and Hotspots of Q Fever Research: A Bibliometric Analysis 1990–2019. BioMed Res. Int. 2022, 2022, 9324471.
- Álvarez-Alonso, R.; Basterretxea, M.; Barandika, J.F.; Hurtado, A.; Idiazabal, J.; Jado, I.; Beraza, X.; Montes, M.; Liendo, P.; García-Pérez, A.L. A Q Fever Outbreak with a High Rate of Abortions at a Dairy Goat Farm: Coxiella burnetii Shedding, Environmental Contamination, and Viability. Appl. Environ. Microbiol. 2018, 84, e01650-18.
- Clark, N.J.; Soares Magalhães, R.J. Airborne geographical dispersal of Q fever from livestock holdings to human communities: A systematic review and critical appraisal of evidence. BMC Infect. Dis. 2018, 18, 218.
- Vellema, P.; Santman-Berends, I.; Dijkstra, F.; van Engelen, E.; Aalberts, M.; Ter Bogt-Kappert, C.; van den Brom, R. Dairy Sheep Played a Minor Role in the 2005-2010 Human Q Fever Outbreak in The Netherlands Compared to Dairy Goats. Pathogens 2021, 10, 1579.
- Byeon, H.S.; Nattan, S.; Kim, J.H.; Han, S.T.; Chae, M.H.; Han, M.N.; Ahn, B.; Kim, Y.D.; Kim, H.S.; Jeong, H.W. Shedding and extensive and prolonged environmental contamination of goat farms of Q fever patients by Coxiella burnetii. Vet. Med. Sci. 2022, 8, 1264–1270.
- Bond, K.A.; Vincent, G.; Wilks, C.R.; Franklin, L.; Sutton, B.; Stenos, J.; Cowan, R.; Lim, K.; Athan, E.; Harris, O.; et al. One Health approach to controlling a Q fever outbreak on an Australian goat farm. Epidemiol. Infect. 2016, 144, 1129–1141.
- Panaiotov, S.; Ciccozzi, M.; Brankova, N.; Levterova, V.; Mitova-Tiholova, M.; Amicosante, M.; Rezza, G.; Kantardjiev, T. An outbreak of Q fever in Bulgaria. Ann. Dell’istituto Super. Sanità 2009, 45, 83–86.
- Genova-Kalou, P.; Vladimirova, N.; Stoitsova, S.; Krumova, S.; Kurchatova, A.; Kantardjiev, T. Q fever in Bulgaria: Laboratory and epidemiological findings on human cases and outbreaks, 2011 to 2017. Eurosurveillance 2019, 24, 1900119.
- Huang, M.; Ma, J.; Jiao, J.; Li, C.; Chen, L.; Zhu, Z.; Ruan, F.; Xing, L.; Zheng, X.; Fu, M.; et al. The epidemic of Q fever in 2018 to 2019 in Zhuhai city of China determined by metagenomic next-generation sequencing. PLoS Negl. Trop. Dis. 2021, 15, e0009520.
- Fishbein, D.B.; Raoult, D. A cluster of Coxiella burnetii infections associated with exposure to vaccinated goats and their unpasteurized dairy products. Am. J. Trop. Med. Hyg. 1992, 47, 35–40.
- King, L.A.; Goirand, L.; Tissot-Dupont, H.; Giunta, B.; Giraud, C.; Colardelle, C.; Duquesne, V.; Rousset, E.; Aubert, M.; Thiéry, R.; et al. Outbreak of Q fever, Florac, Southern France, Spring 2007. Vector Borne Zoonotic Dis. 2011, 11, 341–347.
- Hatchette, T.F.; Hudson, R.C.; Schlech, W.F.; Campbell, N.A.; Hatchette, J.E.; Ratnam, S.; Raoult, D.; Donovan, C.; Marrie, T.J. Goat-Associated Q Fever: A New Disease in Newfoundland. Emerg. Infect. Dis. 2001, 7, 413–419.
- Kovácová, E.; Kazár, J.; Simková, A. Clinical and serological analysis of a Q fever outbreak in western Slovakia with four-year follow-up. Eur. J. Clin. Microbiol. Infect. Dis. 1998, 17, 867–869.
- Gunther, M.J.; Heller, J.; Hayes, L.; Hernandez-Jover, M. Dairy goat producers’ understanding, knowledge and attitudes towards biosecurity and Q-fever in Australia. Prev. Vet. Med. 2019, 170, 104742.
- van der Giessen, J.; Vlaanderen, F.; Kortbeek, T.; Swaan, C.; van den Kerkhof, H.; Broens, E.; Rijks, J.; Koene, M.; De Rosa, M.; Uiterwijk, M.; et al. Signalling and responding to zoonotic threats using a One Health approach: A decade of the Zoonoses Structure in the Netherlands, 2011 to 2021. Eurosurveillance 2022, 27, 2200039.
- Jorm, L.R.; Lightfoot, N.F.; Morgan, K.L. An epidemiological study of an outbreak of Q fever in a secondary school. Epidemiol. Infect. 1990, 104, 467–477.
- Clark, W.H.; Lennette, E.H.; Romer, M.S. Q fever in California. IX. An outbreak aboard a ship transporting goats. Am. J. Hyg. 1951, 54, 35–43.
- Bjork, A.; Marsden-Haug, N.; Nett, R.J.; Kersh, G.J.; Nicholson, W.; Gibson, D.; Szymanski, T.; Emery, M.; Kohrs, P.; Woodhall, D.; et al. First reported multistate human Q fever outbreak in the United States, 2011. Vector Borne Zoonotic Dis. 2014, 14, 111–117.
- Preston, W. Bergey’s Manual of Determinative Bacteriology, 6th ed.; Bergey, D.H., Breed, R.S., Hitchens, A.P., Murray, E.G.D., Eds.; Williams & Wilkins: Baltimore, MD, USA, 1948.
- Drancourt, M.; Roux, V.; Dang, L.V.; Tran-Hung, L.; Castex, D.; Chenal-Francisque, V.; Ogata, H.; Fournier, P.-E.; Crubézy, E.; Raoult, D. Genotyping, Orientalis-like Yersinia pestis, and Plague Pandemics. Emerg. Infect. Dis. 2004, 10, 1585–1592.
- Seshadri, R.; Paulsen, I.T.; Eisen, J.A.; Read, T.D.; Nelson, K.E.; Nelson, W.C.; Ward, N.L.; Tettelin, H.; Davidsen, T.M.; Beanan, M.J.; et al. Complete genome sequence of the Q-fever pathogen Coxiella burnetii. Proc. Natl. Acad. Sci. USA 2003, 100, 5455–5460.
- Sidi-Boumedine, K.; Adam, G.; Angen, O.; Aspan, A.; Bossers, A.; Roest, H.J.; Prigent, M.; Thiéry, R.; Rousset, E. Whole genome PCR scanning (WGPS) of Coxiella burnetii strains from ruminants. Microbes Infect. 2015, 17, 772–775.
- Sidi-Boumedine, K.; Duquesne, V.; Prigent, M.; Yang, E.; Joulié, A.; Thiéry, R.; Rousset, E. Impact of IS1111 insertion on the MLVA genotyping of Coxiella burnetii. Microbes Infect. 2015, 17, 789–794.
- Eldin, C.; Mélenotte, C.; Mediannikov, O.; Ghigo, E.; Million, M.; Edouard, S.; Mege, J.L.; Maurin, M.; Raoult, D. From Q Fever to Coxiella burnetii Infection: A Paradigm Change. Clin. Microbiol. Rev. 2017, 30, 115–190.
- Mege, J.L.; Maurin, M.; Capo, C.; Raoult, D. Coxiella burnetii: The “query” fever bacterium—Model of immune subversion by a strictly intracellular microorganism. FEMS Microbiol. Rev. 1997, 19, 209–217.
- Beare, P.A.; Samuel, J.E.; Howe, D.; Virtaneva, K.; Porcella, S.F.; Heinzen, R.A. Genetic Diversity of the Q Fever Agent, Coxiella burnetii, Assessed by Microarray-Based Whole-Genome Comparisons. J. Bacteriol. 2006, 188, 2309–2324.
- Denison, A.M.; Massung, R.F.; Thompson, H.E. Analysis of the O-antigen biosynthesis regions of phase II Isolates of Coxiella burnetii. FEMS Microbiol. Lettters 2007, 267, 102–107.
- Hoover, T.A.; Culp, D.W.; Vodkin, M.H.; Williams, J.C.; Thompson, H.A. Chromosomal DNA Deletions Explain Phenotypic Characteristics of Two Antigenic Variants, Phase II and RSA 514 (Crazy), of the Coxiella burnetii Nine Mile Strain. Infect. Immun. 2002, 70, 6726–6733.
- Kuley, R.; Smith, H.E.; Frangoulidis, D.; Smits, M.A.; Roest, H.I.J.; Bossers, A. Cell-Free Propagation of Coxiella burnetii Does Not Affect Its Relative Virulence. PLoS ONE 2015, 10, e0121661.
- Coleman, S.A.; Fischer, E.R.; Howe, D.; Mead, D.J.; Heinzen, R.A. Temporal Analysis of Coxiella burnetii Morphological Differentiation. J. Bacteriol. 2004, 186, 7344–7352.
- McCaul, T.F.; Williams, J.C. Developmental Cycle of Coxiella burnetii: Structure and Morphogenesis of Vegetative and Sporogenic Differentiations. J. Bacteriol. 1981, 147, 1063–1076.
- Heinzen, R.A.; Hackstadt, T.; Samuel, J.E. Developmental biology of Coxiella burnetii. Trends Microbiol. 1999, 7, 149–154.
- Seshadri, R.; Hendrix, L.R.; Samuel, J.E. Differential Expression of Translational Elements by Life Cycle Variants of Coxiella burnetii. Infect. Immun. 1999, 67, 6026–6033.
- Sandoz, K.M.; Popham, D.L.; Beare, P.A.; Sturdevant, D.E.; Hansen, B.; Nair, V.; Heinzen, R.A. Transcriptional Profiling of Coxiella burnetii Reveals Extensive Cell Wall Remodeling in the Small Cell Variant Developmental Form. PLoS ONE 2016, 11, e0149957.
- Shannon, J.G.; Heinzen, R.A. Adaptive immunity to the obligate intracellular pathogen Coxiella burnetii. Immunol. Res. 2009, 43, 138–148.
- Amara, A.B.; Ghigo, E.; Le Priol, Y.; Lépolard, C.; Salcedo, S.P.; Lemichez, E.; Bretelle, F.; Capo, C.; Mege, J.L. Coxiella burnetii, the agent of Q fever, replicates within trophoblasts and induces a unique transcriptional response. PLoS ONE 2010, 5, e15315.
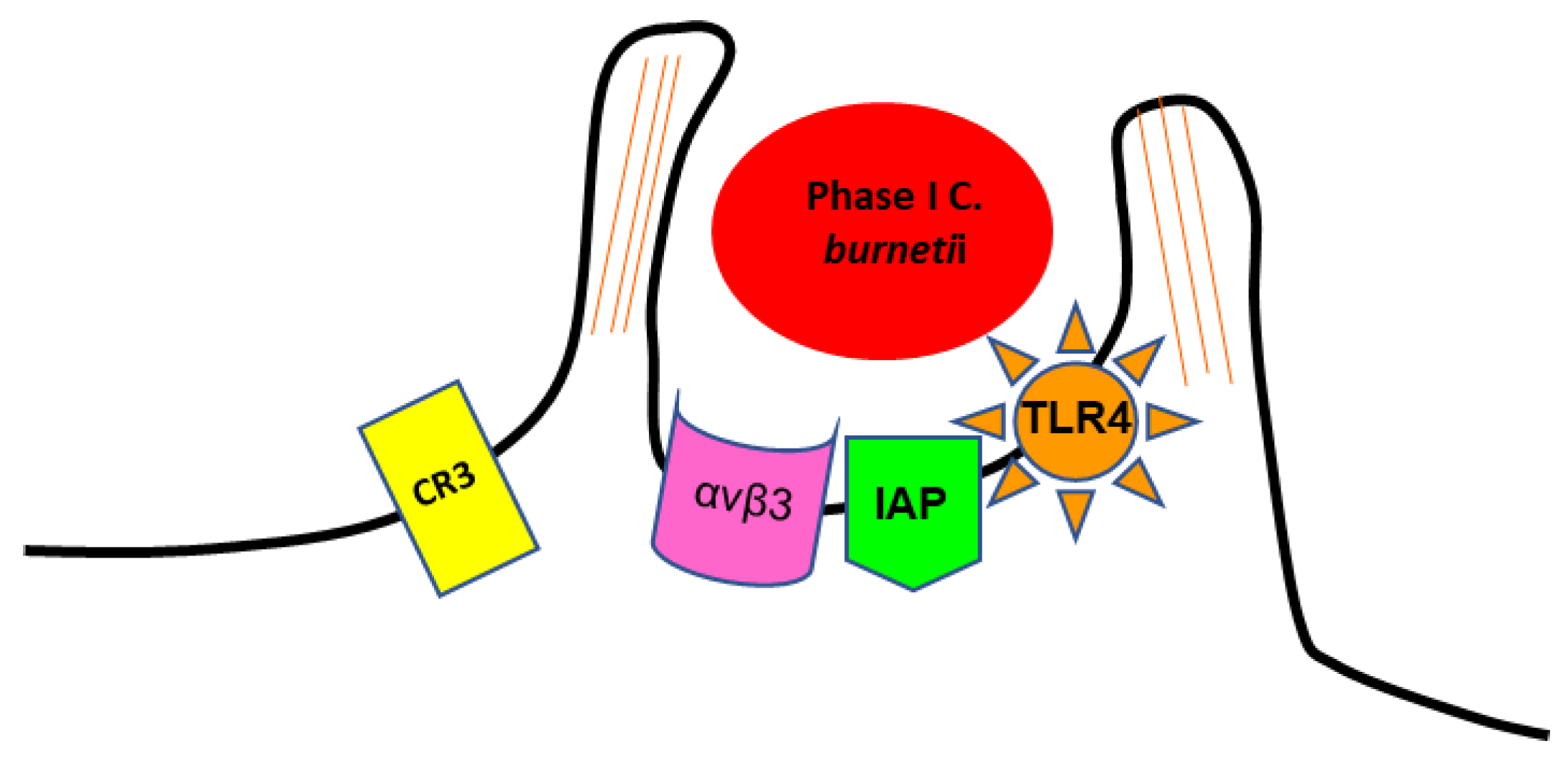
- Capo, C.; Moynault, A.; Collette, Y.; Olive, D.; Brown, E.J.; Raoult, D.; Mege, J.L. Coxiella burnetii avoids macrophage phagocytosis by interfering with spatial distribution of complement receptor 3. J. Immunol. 2003, 170, 4217–4225.
- Dupuy, A.G.; Caron, E. Integrin-dependent phagocytosis: Spreading from microadhesion to new concepts. J. Cell Sci. 2008, 121, 1773–1783.
- Meconi, S.; Jacomo, V.; Boquet, P.; Raoult, D.; Mege, J.L.; Capo, C. Coxiella burnetii Induces Reorganization of the Actin Cytoskeleton in Human Monocytes. Infect. Immun. 1998, 66, 5527–5533.
- Meconi, S.; Capo, C.; Remacle-Bonnet, M.; Pommier, G.; Raoult, D.; Mege, J.L. Activation of protein tyrosine kinases by Coxiella burnetii: Role in actin cytoskeleton reorganization and bacterial phagocytosis. Infect. Immun. 2001, 69, 2520–2526.
- Honstettre, A.; Ghigo, E.; Moynault, A.; Capo, C.; Toman, R.; Akira, S.; Takeuchi, O.; Lepidi, H.; Raoult, D.; Mege, J.L. Lipopolysaccharide from Coxiella burnetii is involved in bacterial phagocytosis, filamentous actin reorganization, and inflammatory responses through Toll-like receptor 4. J. Immunol. 2004, 172, 3695–3703.
- van Schaik, E.J.; Chen, C.; Mertens, K.; Weber, M.M.; Samuel, J.E. Molecular pathogenesis of the obligate intracellular bacterium Coxiella burnetii. Nat. Rev. Microbiol. 2013, 11, 561–573.
- Heinzen, R.A.; Hackstadt, T. A developmental stage-specific histone H1 homolog of Coxiella burnetii. J. Bacteriol. 1996, 78, 5049–5052.
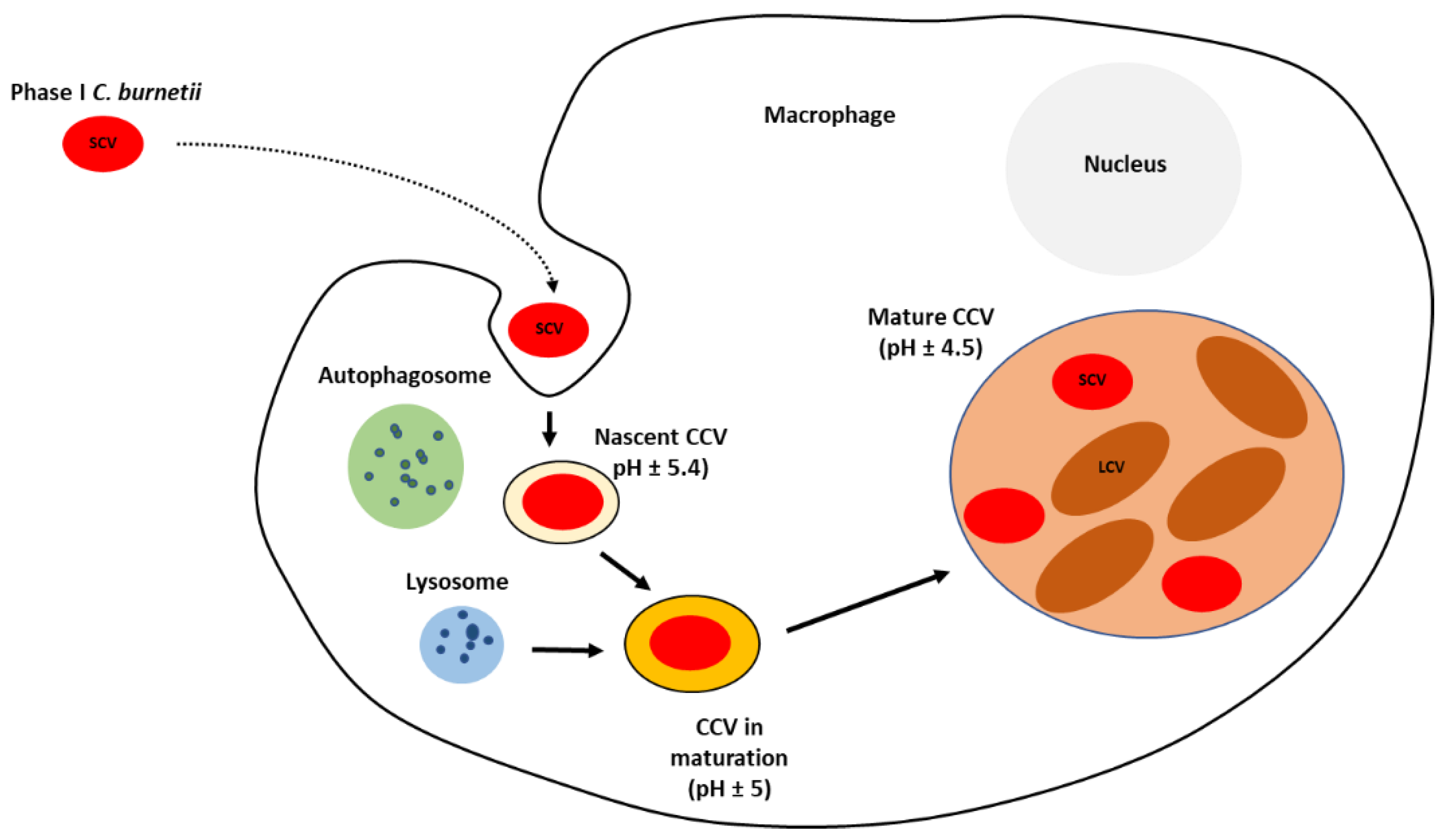
- Kinchen, J.M.; Ravichandran, K.S. Phagosome maturation: Going through the acid test. Nat. Rev. Mol. Cell Biol. 2008, 9, 781–795.
- Howe, D.; Shannon, J.G.; Winfree, S.; Dorward, D.W.; Heinzen, R.A. Coxiella burnetii phase I and II variants replicate with similar kinetics in degradative phagolysosome-like compartments of human macrophages. Infect. Immun. 2010, 78, 3465–3474.
- Berón, W.; Gutierrez, M.G.; Rabinovitch, M.; Colombo, M.I. Coxiella burnetii Localizes in a Rab7-Labeled Compartment with Autophagic Characteristics. Infect. Immun. 2002, 70, 5816–5821.
- Schulze-Luehrmann, J.; Eckart, R.A.; Ölke, M.; Saftig, P.; Liebler-Tenorio, E.; Lührmann, A. LAMP proteins account for the maturation delay during the establishment of the Coxiella burnetii-containing vacuole. Cell. Microbiol. 2016, 18, 181–194.
- Ghigo, E.; Capo, C.; Tung, C.H.; Raoult, D.; Gorvel, J.P.; Mege, J.L. Coxiella burnetii survival in THP-1 monocytes involves the impairment of phagosome maturation: IFN-g mediates its restoration and bacterial killing. J. Immunol. 2002, 169, 4488–4495.
- Howe, D.; Melnicáková, J.; Barák, I.; Heinzen, R.A. Maturation of the Coxiella burnetii parasitophorous vacuole requires bacterial protein synthesis but not replication. Cell. Microbiol. 2003, 5, 469–480.
- Flannagan, R.S.; Jaumouillé, V.; Grinstein, S. The cell biology of phagocytosis. Ann. Rev. Pathol. 2012, 7, 61–98.
- Barry, A.; Mege, J.; Ghigo, E. Hijacked phagosomes and leukocyte activation: An intimate relationship. J. Leukoc. Biol. 2011, 89, 373–382.
- Voth, D.E.; Heinzen, R.A. Lounging in a lysosome: The intracellular lifestyle of Coxiella burnetii. Cell. Microbiol. 2007, 9, 829–840.
- Pareja, M.E.M.; Bongiovanni, A.; Lafont, F.; Colombo, M.I. Alterations of the Coxiella burnetii Replicative Vacuole Membrane Integrity and Interplay with the Autophagy Pathway. Front. Cell. Infect. Microbiol. 2017, 7, 112.
- Lührmann, A.; Roy, C.R. Coxiella burnetii inhibits activation of host cell apoptosis through a mechanism that involves preventing cytochrome c release from mitochondria. Infect. Immun. 2007, 75, 5282–5289.
- Voth, D.E.; Howe, D.; Heinzen, R.A. Coxiella burnetii inhibits apoptosis in human THP-1 cells and monkey primary alveolar macrophages. Infect. Immun. 2007, 75, 4263–4271.
- Voth, D.E.; Heinzen, R.A. Coxiella Type IV Secretion and Cellular Microbiology. Curr. Opin. Microbiol. 2009, 12, 74–80.
- Vázques, C.L.; Colombo, M.I. Coxiella burnetii modulates Beclin 1 and Bcl-2, preventing host cell apoptosis to generate a persistent bacterial infection. Cell. Death Differ. 2010, 17, 421–438.
- Howe, D.; Mallavia, L.P. Coxiella burnetii Exhibits Morphological Change and Delays Phagolysosomal Fusion after Internalization by J774A. 1 Cells. Infect. Immun. 2000, 68, 3815–3821.
- Jones, R.M.; Nicas, M.; Hubbard, A.E.; Reingold, A.L. The Infectious Dose of Coxiella burnetii (Q Fever). Appl. Biosaf. 2006, 11, 32–41.
- Brooke, R.J.; Mutters, N.T.; Péter, O.; Kretzschmar, M.E.E.; Teunis, P.F.M. Exposure to low doses of Coxiella burnetii caused high illness attack rates: Insights from combining human challenge and outbreak data. Epidemics 2015, 11, 1–6.
- Brooke, R.J.; Kretzschmar, M.E.; Mutters, N.T.; Teunis, P.F. Human dose response relation for airborne exposure to Coxiella burnetii. BMC Infect. Dis. 2013, 13, 488.
- Graham, J.G.; MacDonald, L.J.; Hussain, S.K.; Sharma, U.M.; Kurten, R.C.; Voth, D.E. Virulent Coxiella burnetii Pathotypes Productively Infect Primary Human Alveolar Macrophages. Cell. Microbiol. 2013, 15, 1012–1025.
- Marriott, H.M.; Dockrell, D.H. The role of the macrophage in lung disease mediated by bacteria. Exp. Lung Res. 2007, 33, 493–505.
- Stein, A.; Louveau, C.; Lepidi, H.; Ricci, F.; Baylac, P.; Davoust, B.; Raoult, D. Q fever pneumonia: Virulence of C. burnetii pathovars in a murine model of aerosol infection. Infect. Immun. 2005, 73, 2469–2477.
- Roest, H.I.J.; van Gelderen, B.; Dinkla, A.; Frangoulidis, D.; van Zijderveld, F.; Rebel, J.; van Keulen, L. Q fever in pregnant goats: Pathogenesis and excretion of C. burnetii. PLoS ONE 2012, 7, e48949.
- Ammerdorffer, A.; Roest, H.I.; Dinkla, A.; Post, J.; Schoffelen, T.; van Deuren, M.; Sprong, T.; Rebel, J.M. The effect of C. burnetii infection on the cytokine response of PBMCs from pregnant goats. PLoS ONE 2014, 9, e109283.
- Sánchez, J.; Souriauy, A.; Buendía, A.J.; Arricau-Bouvery, N.; Matínez, C.M.; Salinas, J.; Rodolakis, A.; Navarro, J.A. Experimental Coxiella burnetii Infection in Pregnant Goats: A Histopathological and Immunohistochemical Study. J. Comp. Path. 2006, 135, 108–115.
- Roest, H.I.J.; Dinkla, A.; Koets, A.P.; Post, J.; van Keulen, L. Experimental Coxiella burnetii infection in non-pregnant goats and the effect of breeding. Vet. Res. 2020, 51, 74.
- Benoit, M.; Barbarat, B.; Bernard, A.; Olive, D.; Mege, J.L. Coxiella burnetii, the agent of Q fever, stimulates an atypical M2 activation program in human macrophages. Eur. J. Immunol. 2008, 38, 1065–1070.
- Ghigo, E.; Capo, C.; Raoult, D.; Mege, J.L. Interleukin-10 stimulates Coxiella burnetii replication in human monocytes through tumor necrosis factor down-modulation: Role in microbicidal defect of Q fever. Infect. Immun. 2001, 69, 2345–2352.
- Ghigo, E.; Imbert, G.; Capo, C.; Raoult, D.; Mege, J.L. Interleukin-4 induces Coxiella burnetii replication in human monocytes but not in macrophages. Ann. New York Acad. Sci. 2003, 990, 450–459.
- Zhang, G.; Russell-Lodrigue, K.E.; Andoh, M.; Zhang, Y.; Hendrix, L.R.; Samuel, J.E. Mechanisms of vaccine-induced protective immunity against Coxiella burnetii infection in BALB/c mice. J. Immunol. 2007, 179, 8372–8380.
- Roest, H.I.J.; Bossers, A.; Rebel, J.M.J. Q Fever Diagnosis and Control in Domestic Ruminants. Dev. Biol. 2013, 135, 183–189.
- Teunis, P.F.M.; Schimmer, B.; Notermans, D.W.; Leenders, A.C.A.P.; Wever, P.C.; Kretzschmar, M.E.E.; Schneeberger, P.M. Time-course of antibody responses against Coxiella burnetii following acute Q fever. Epidemiol. Infect. 2013, 141, 62–73.
- Langley, J.M.; Marrie, T.J.; Leblanc, J.C.; Almudevar, A.; Resch, L.; Raoult, D. Coxiella burnetii seropositivity in parturient women is associated with adverse pregnancy outcomes. Am. J. Obstet. Gynecol. 2003, 189, 228–232.
- Carcopino, X.; Raoult, D.; Bretelle, F.; On Boubli, L.; Stein, A. Managing Q Fever during Pregnancy: The Benefits of Long-Term Cotrimoxazole Therapy. Clin. Infect. Dis. 2007, 45, 548–555.
- Lennette, E.H.; Holmes, M.A.; Abinanti, F.R. Remove from marked Records, Q. Fever Studies. XIV. Observations on the Pathogenesis of the Experimental Infection induced in Sheep by the Intravenous Route. Am. J. Hyg. 1952, 55, 254–267.
- Martinov, S.P.; Neikov, P.; Popov, G.V. Experimental Q fever in sheep. Eur. J. Epidemiol. 1989, 5, 428–431.
- Berri, M.; Rousset, E.; Hechard, C.; Champion, J.L.; Dufour, P.; Russo, P.; Rodolaskis, A. Progression of Q Fever and Coxiella burnetii shedding in milk after an outbreak of enzootic abortion in a goat herd. Vet. Rec. 2005, 156, 548–549.
- Berri, M.; Rousset, E.; Champion, J.L.; Russo, P.; Rodolaskis, A. Goats may experience reproductive failures and shed Coxiella burnetii at two successive parturitions after a Q fever infection. Res. Vet. Sci. 2007, 83, 47–52.
- Van den Brom, R.; Vellema, P. Q fever outbreaks in small ruminants and people in the Netherlands. Small Rum. Res. 2009, 86, 74–79.
- Arricau-Bouvery, N.; Rodolakis, A. Is Q fever an emerging or re-emerging Zoonosis? Vet. Res. 2005, 36, 327–349.
- Eibach, R.; Bothe, F.; Runge, M.; Fischer, S.F.; Philipp, W.; Ganter, M. Q fever: Baseline monitoring of a sheep and a goat flock associated with human infections. Epidemiol. Infect. 2012, 140, 1939–1949.