Speech is a communication method found only in humans that relies on precisely articulated sounds to encode and express thoughts. Anatomical differences in the maxilla, mandible, tooth position, and vocal tract affect tongue placement and broadly influence the patterns of airflow and resonance during speech production. Alterations in these structures can create perceptual distortions in speech known as speech sound disorders (SSDs). As craniofacial development occurs, the vocal tract, jaws, and teeth change in parallel with stages of speech development, from babbling to adult phonation. Alterations from a normal Class 1 dental and skeletal relationship can impact speech. Dentofacial disharmony (DFD) patients have jaw disproportions, with a high prevalence of SSDs, where the severity of malocclusion correlates with the degree of speech distortion.
1. Development from Birth to Seven Months Old
Speech and the craniofacial complex simultaneously develop during childhood (
Figure 1). Immediately after birth, vocal development begins as a baby takes its first cry. At birth, the mandible is underdeveloped with a short ramus (Class II profile), the larynx is high in the throat, and the tongue takes up much of the oral cavity space
[27,28][1][2]. The alveolar ridges develop along with the underlying tooth buds, and gum pads eventually begin to touch
[28][2]. Anatomical changes in the jaws, tongue, alveolus, and vocal tract affect the types of sounds infants are able to produce.
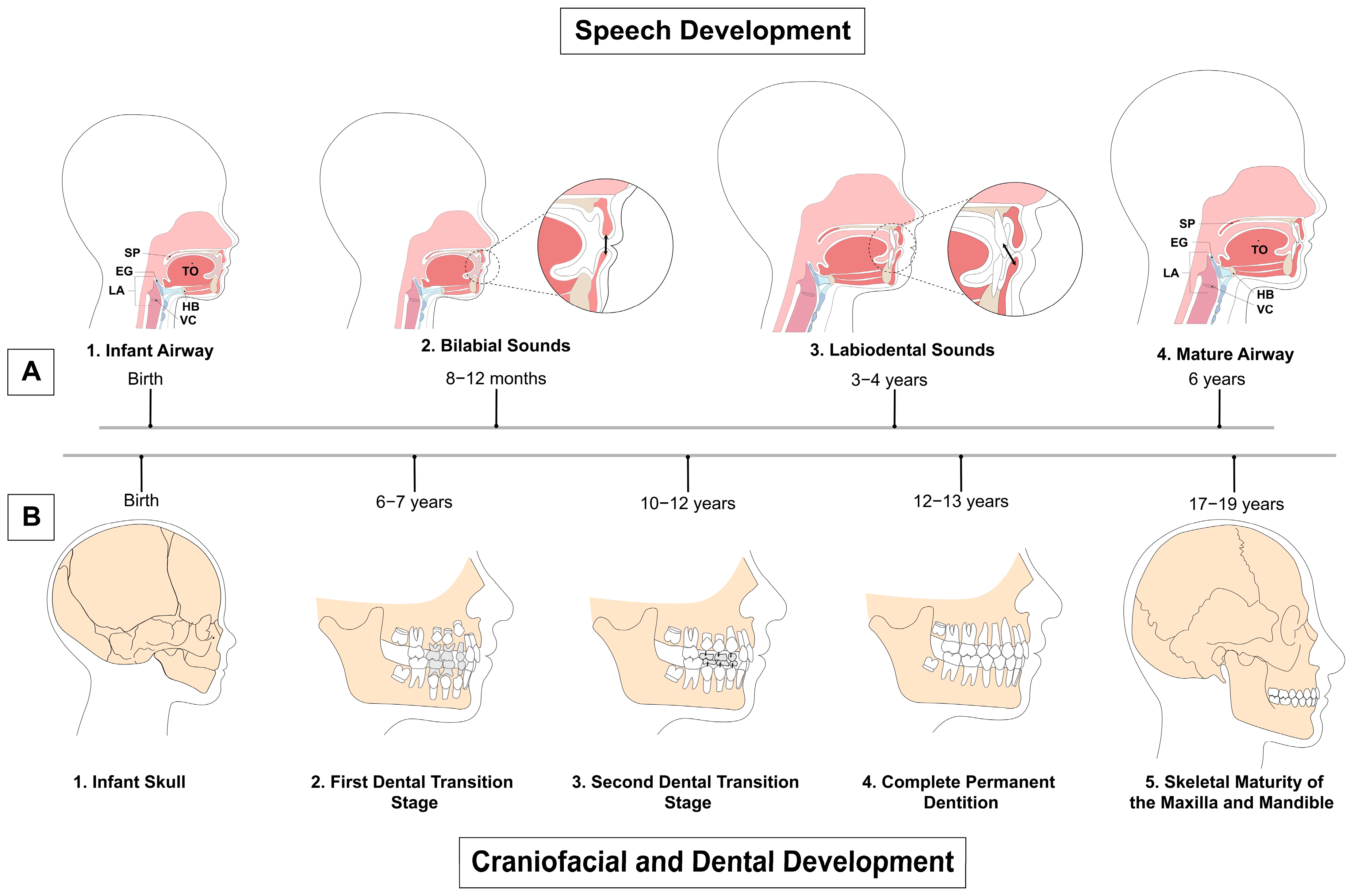
Figure 1. Timeline of speech, craniofacial, and dental development. (A) Speech development from birth to maturity. 1. Airway structures in a child at birth. 2. At 8 to 12 months, the child produces primarily bilabial sounds with the absence of teeth. 3. Labiodental sounds start to be produced at 3 to 4 years old with the eruption of teeth, similar to the adult stage. 4. Maturity of the airway at 6 years old. Structures are consistent through adulthood. (B) Craniofacial and dental development from infancy to adulthood. 1. Infant skull at birth. 2. First transition stage of dental development with eruption of first permanent molars, and central and lateral incisors at 6 to 7 years old, establishing the mixed dentition. The first transition stage is followed by the interphase dental period from 8 to 9 years old, when the mixed dentition remains stable. 3. The second dental transition stage from 10 to 12 years old includes exfoliation of all remaining primary teeth, with replacement of deciduous canines and premolars with permanent successors. 4. Complete permanent dentition at 12 to 13 years old. 5. Skeletal maturity of the maxilla and mandible at 17 to 19 years old. SP: soft palate; EG: epiglottis; LA: larynx; TO: tongue; HB: hyoid bone; VC: vocal cords.
The stages of infant sound development include phonation (i.e., crying), the goo/coo stage, expansion, reduplicated and no-reduplicated babbling, and the one-word and then the two-word stages
[27][1]. From birth to one month of age, an infant communicates through crying, which consists of vowel sounds such as “oohs” and “aahs” during the phonation stage. At two months, the infant enters the cooing period and begins to develop front and central vowels along with back consonants such as [k], hence the name of the stage. At around four months of age, the larynx, hyoid, and tongue descend, and the laryngopharynx lengthens, allowing for a wider range of sound production including isolated vowels and the beginning of other consonants
[29][3]. The expansion stage (four to seven months) is initiated when the mandible undergoes downward and forward growth, increasing oral space for vowel production
[27][1].
2. Development from Seven to Twelve Months Old
The babbling period occurs from seven to twelve months and begins with infants imitating speech and understanding word meaning. Often, their first word stems from babbling and imitation (such as ma-ma-ma), which is then reinforced by those around them repeating the word mama. From eight to twelve months, oral stops [b, p] and nasals ([m] mama and [n] no) are the most frequently produced consonants. Sounds produced in babbling are typically acquired in order of ease of production. Bilabials (e.g., [b] baba) tend to be amongst the first sounds produced due to their strong visual cues. Stops (e.g., [p] pea), nasals, and glides (e.g., [j] yes and [w] why) also dominate speech in the early periods, while fricatives (e.g., [s] see), affricates (e.g., [tʃ] cheer), and liquids (e.g., [l] led, [ɹ] red) appear later, suggesting greater motor control is required for these sounds. At the end of the babbling period, children use approximately two times as many vowels as consonants and begin to develop stops and fricatives
[26][4]. Stops, such as the /p/ sound, are made when complete closure of the vocal tract prevents air from escaping, while fricatives such as [f] involve air escaping through a small constriction producing turbulent airflow
[30][5].
3. Development from One to Three Years Old
Speech development, during and after the babbling period, is influenced by the eruption of primary teeth and the development of the supporting bony alveolus. At around six months of age, the primary central and lateral incisors begin to erupt, when infants are ready to be weaned, and by twenty-three to thirty-three months of age, babies have a full complement of primary dentition (twenty primary teeth in total). A concomitant increase in vertical facial height yields space between the gum pads to accommodate the erupting primary teeth
[11][6]. The alveolus and dentition significantly develop and can assume their roles as passive articulators for the tongue and lips to act against as active articulators. At one to two years of age, children acquire nearly as many consonants as vowels and begin to learn both dental and postdental sounds such as [f] and [d]
[31][7]. As this occurs, deciduous (i.e., primary) canines and first molars begin to erupt into the oral cavity, while deciduous incisors have fully erupted
[32][8].
4. Development from Three to Five Years Old
Two to four months after children’s first word, they begin their two-word stage, forming short telegraphic sentences (such as mama go). Typically, the two-word stage begins following the acquisition of roughly forty words
[33][9]. Entering the third year, children can recursively combine phrases, allowing multiword phrases, and children learn to produce all vowels and around two-thirds of consonants and liquids (liquids are vowel-like consonants such as the [l] in led and the [ɹ] in red)
[34][10]. Children learn they can communicate through speech: crying when sad or complaining when angry motivates actions from those around them. Dentally, second primary molars erupt to complete the primary dentition between twenty-three and thirty-three months
[32][8]. During early years, non-nutritive sucking habits are common (i.e., thumb sucking) and are seen in 73% of children at ages two to five
[35][11]. Sucking habits are associated with anterior open bites and posterior crossbites, impacting speech, and need to resolve by four to six years old for self-correction to occur without orthodontic intervention.
As children continue to develop, their oral functions become refined, including breathing, sucking, swallowing, and chewing
[36][12]. By the age of four, children typically know 77% of sounds; knowledge of sounds continues expanding until the age of seven or eight. By four, the mandible will have increased in length and ramus height, leading to a decreased gonial angle; by seven, the cranial base will have lengthened, moving the maxilla and mandible downward and forward
[28,37][2][13]. The pattern of downward and forward facial growth continues throughout craniofacial development
[28][2]. The maxilla and mandible develop as modeled by Scammon’s growth curves, with the maxilla developing earlier (similar to the neural curve) and the mandible growing longer and later (similar to the somatic general body curve)
[28][2]. The maxilla undergoes anterior surface remodeling (i.e., resorption) and growth via bone apposition (i.e., deposition) at its superior and posterior sutures, displacing the maxilla downward and forward and increasing the oral cavity size; bony deposition at the posterior aspect of the alveolar processes creates more space for distal molar tooth eruption
[28,38][2][14]. Mandibular growth occurs later than maxillary development, up through 18–20 years of age, and includes downward and forward displacement, with the condyle growing upward and backward; the posterior ramus undergoes appositional growth, and the anterior ramus resorbs, increasing space for distal molar tooth eruption
[28,39][2][15]. Oral cavity size increases, with increasing facial dimensions in the transverse, anterior–posterior, and vertical dimensions
[40,41][16][17]. The vocal tract also lengthens, lowering its resonant frequencies
[42][18].
5. Development from Six to Nine Years Old
From age six to seven, the permanent first molars erupt distal to the primary second molars, lengthening the dental arch; additionally, deciduous central incisors and then lateral incisors are exfoliated with the eruption of their permanent successors as part of the first transition stage of dental development
[32][8] (
Figure 1). The interphase dental period then begins from ages eight to nine (i.e., the intermediate intertransitional phase), which is the one to two-year span when the mixed dentition remains relatively stable, with permanent incisors and first molars
[43][19]. If articulation errors exist at age eight to nine, self-correction is unlikely, and intervention may be needed. By eight years old, children typically have mastered the sounds of their primary language
[31][7].
Generally, early speech deficits are referred to a Speech-Language Pathologist (SLP); however, due to the mild nature of most deficits, most children are not referred until school age, at which time they may be diagnosed with an SSD
[26][4]. An articulation disorder is a type of SSD characterized by “atypical production of speech sounds characterized by substitutions, omissions, additions or distortions that may interfere with intelligibility”
[10][20]. Articulation disorders are often seen in DFD patients with severe malocclusions and jaw disproportions
[19,26,44][4][21][22]. Starting at age seven, the
American Association of Orthodontists (AAO) recommends that children be referred to an orthodontist for an initial evaluation
[45][23]. As a result, orthodontists can play an important role in diagnosing significant malocclusions and speech abnormalities, and appropriately referring to SLPs for treatment in conjunction with Phase I and II orthodontic care.
6. Development from Ten to Twelve Years Old
The second dental transition stage occurs from ages ten to twelve years old and includes the replacement of deciduous canines and molars with permanent canines and premolars and a slight reduction in dental arch length
[46][24]. By puberty, when most patients are undergoing comprehensive Phase II orthodontic treatment and vocal tracts are lengthening, speech development has concluded, with few corrections, if any, occurring without intervention
[2][25]. Speech sound acquisition is judged to be complete, with adult-like motor control, at about eleven or twelve years old
[47][26]. It is interesting to note that speech errors are engrained by the interphase period of dental development (ages eight to nine) and that speech development fully plateaus when the permanent dentition is in place at puberty. Speech, craniofacial, and dental development occur in parallel with one another, with each developmental process influencing the other.