Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Goran Šimić and Version 2 by Sirius Huang.
Alzheimer’s disease (AD) is the most common cause of dementia worldwide (60–70% of cases), affecting over 55 million people. The role of metals in the pathogenesis of AD is still debated. Although previous research has linked changes in essential metal homeostasis and exposure to environmental heavy metals to the pathogenesis of AD, more research is needed to determine the relationship between metals and AD.
- Alzheimer’s disease
- essential metals
- heavy metals
- biomarker
- Mendelian randomization
1. Molecular Mechanisms through Which Metals Contribute to Alzheimer’s Disease Pathology
Increased metal concentration in the brain may contribute to various AD-associated pathological processes including Aβ-aggregation [1][2][30,31], hyperphosphorylation of tau protein [3][4][32,33], neuroinflammation [5][34], oxidative stress [6][35], blood–brain barrier (BBB) impairment [7][36], apoptosis and necrosis of neurons [8][9][37,38], and autophagy [10][39] (Figure 1). Experimental evidence indicates that both essential metals and heavy metals increase the aggregation of Aβ [1][11][12][30,40,41] and the hyperphosphorylation and aggregation of tau protein [4][13][14][15][33,42,43,44]. Furthermore, the exposure of young rats to a mixture of heavy metals induced neuroinflammation dependent on oxidative stress [16][45]. In addition, some essential metals such as Fe [17][46], Cu [18][47], Zn, and calcium (Ca) [10][39] can induce oxidative stress. Fe participates in Fenton reactions and can therefore contribute to the formation of reactive oxygen species [17][46]. Both the observed disruption of the BBB [19][20][48,49] and the apoptosis and necrosis of neurons [8][9][37,38] upon exposure to heavy metals may be preceded by oxidative stress, according to experimental evidence. Neurons are extremely sensitive to oxidative stress. Wang et al. [10][39] proposed that metal ion imbalance could induce oxidative stress, with the following downstream effects: (1) imbalance of protein kinases and phosphatases, increasing tau protein phosphorylation, and (2) imbalance of secretases, resulting in an increase in Aβ production (reviewed in [10][39]). On the other hand, essential metals also serve as cofactors in enzymes that combat oxidative stress. Cu, Zn, and manganese (Mn) are enzyme components of superoxide dismutase enzymes, while selenium is an enzyme component of glutathione peroxidase [21][50].
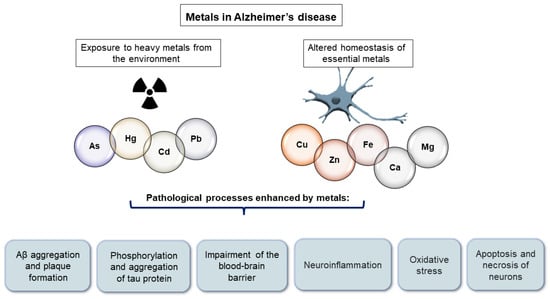
Figure 1.
Pathological processes enhanced by metals in Alzheimer’s disease.
Although there is a substantial body of evidence linking metals to AD-related pathological processes, it is unclear whether disrupted metal homeostasis is involved in the pathogenesis of AD, results from AD pathological processes, or both. Given that AD is a complex disease driven by both genetic and environmental factors, it is unlikely that AD pathogenesis will be explained by a single factor, but rather by the interaction of many.
2. Heavy Metals in Alzheimer’s Disease
Heavy metals including arsenic (As) [22][51], cadmium (Cd) [20][49], lead (Pb) [23][52], and mercury (Hg) [23][52] can cross the BBB and accumulate in the brain, or they can bypass the BBB and enter the brain directly through the olfactory pathway [24][53]. Some researchers have hypothesized that early exposure to heavy metals is associated with the later development of AD. Based on their observations of experimental animals, they concluded that early-life exposure to As [25][54], Pb [26][55], and Cd [27][56] may contribute to the development of neurodegeneration later in life, which is consistent with the developmental hypothesis of AD [28][29][30][57,58,59].
2.1. Arsenic
As is a metalloid that can be ingested through contaminated water, soil, and air, but primarily through drinking contaminated water. More than 220 million people are estimated to consume water that exceeds the permissible level of 10 µg/L [31][60]. Epidemiological studies suggest that As contributes to cognitive impairment [32][61] and an increased risk of AD [33][62], and that elevated As levels in soil are associated with an increase in AD-related mortality [34][63]. As exposure has also been associated with memory impairments in animal studies [35][36][37][64,65,66]. As exposure also increases Aβ levels [38][67], promotes tau hyperphosphorylation [3][39][40][32,68,69], tau aggregation [3][32], oxidative stress caused mainly by mitochondrial dysfunction [41][70], vascular damage [42][71], neuroinflammation [5][34], and apoptosis and the necrosis of neurons [8][9][37,38] (Figure 1). In the majority of human studies, there were no significant differences in As levels between AD patients and the controls, although some studies observed a significant increase in As levels in AD patients [43][44][72,73] and a positive association with CSF AD biomarkers [45][74].
2.2. Cadmium
Humans are exposed to Cd through food, air, and water [46][75]. Smokers have Cd levels that are two to four times higher than nonsmokers [47][76]. Cd may also play a role in the development of AD pathological changes. Cd has been linked in human studies to increased mortality due to AD [48][49][77,78] and cognitive decline [50][51][52][79,80,81]. Ruczaj and Brzoska proposed that Cd primarily exerts its effects by inducing oxidative stress [53][82]. Nevertheless, it also interacts with Aβ [54][83] and increases Aβ aggregation [1][11][30,40], promotes tau hyperphosphorylation [4][33] and aggregation [13][42], impairs the BBB [19][20][48,49], impairs cholinergic transmission and causes the death of cholinergic neurons in the basal forebrain [55][84], and disrupts intracellular cation homeostasis by being an anti-metabolite of Zn and replacing it in Zn enzymes [56][85] (Figure 1). In human studies, there is either an increase [57][86] or no difference [58][87] in Cd levels between AD patients and healthy controls.
2.3. Mercury
Exposure to Hg occurs through food, air, and water, with seafood consumption being the primary source of mercury poisoning [59][152]. Three- to 5-fold increases in Hg levels in the air and water have been documented as a result of industrialization [60][153]. A systematic review [61][154] and meta-analysis [62][155] demonstrated an association between Hg exposure and cognitive decline and progression of AD, but a subsequent report [63][156] did not confirm these findings. In addition, a neuropathological study of 286 brains by Morris et al. revealed no correlation between higher brain Hg levels and neuropathological alterations [59][152]. However, there are multiple molecular mechanisms through which Hg may contribute to the pathogenesis of AD. It promotes Aβ production [64][157] and aggregation [1][30], tau hyperphosphorylation [65][66][158,159] and aggregation [67][160], induces oxidative stress [6][35], and alters calcium homeostasis [68][161] (Figure 1). Human body fluid Hg measurements yielded contradictory results. Both an increase and a decrease were observed in Hg levels between the AD and control subjects, or there was no change. In addition, the CSF Hg level was positively correlated with several CSF AD biomarkers [45][74], whereas the blood Hg level was positively correlated with the CSF Aβ1–42 level [69][145].
2.4. Lead
In addition to food, air, and water, humans are also exposed to lead [70][29] through ingestion. Epidemiological studies have demonstrated that lead exposure contributes to cognitive impairment [71][72][162,163]. Moreover, experimental studies have reported an association between Pb and AD pathological changes. Pb interacts with Aβ [2][31] and increases Aβ production [16][73][45,164] and aggregation [2][31], increases tau hyperphosphorylation [74][165], compromises the BBB [7][36], induces epigenetic modifications by altering the expression of AD-related genes [75][76][166,167], disrupts intracellular cation homeostasis by interfering with Ca homeostasis and replacing Zn ions in Zn enzymes [77][168], and induces oxidative stress [78][169]. In human studies, there was a decrease or no difference in the Pb levels between the AD patients and control subjects, whereas a recent MR study found that higher blood Pb levels were a risk factor for AD [79][170].
2.5. Aluminum
Aluminum (Al), the most abundant metal in the Earth’s crust [80][171], is not an essential element for life; however, in its free, solvated, and trivalent forms, Al3+ is biologically reactive [81][172], accumulating in the central nervous system [82][83][173,174]. In AD-affected brain regions including the entorhinal cortex, hippocampal region, and amygdala, the concentration of Al is higher [84][85][175,176]. Al was co-deposited with fibrillar Aβ in amyloid plaques in a study of brain tissue samples from donors with familial AD (fAD) and the PSEN1-E280A (Glu280Ala) mutation [81][86][172,177]. Cortical Aβ levels are elevated in donors with this mutation, and this mutation is associated with an aggressive etiology of AD [87][178]. Aluminum’s unique association with Aβ and the high levels of Al found in these brain tissues suggest that Al plays a role in the neuropathology of fAD [86][177].
When Al binds to various proteins, oligomerization can occur, resulting in conformational changes that prevent proteases from degrading the proteins. In addition, Al3+ binds strongly to phosphorylated amino acids, causing highly phosphorylated cytoskeleton proteins to aggregate and accumulate [88][179]. As a result, Al induces the apoptotic death of neurons and glial cells. Al-Aβ co-deposition in fAD has been hypothesized, but its association with intraneuronal NFTs has not been confirmed [86][89][177,180], as demonstrated by Mold et al. [90][181]. While Al binding to Aβ in amyloid plaques is anticipated in the early stages of disease progression [86][87][91][177,178,182], an association with tau may occur in later disease stages [86][87][91][177,178,182]. Numerous studies have investigated the association between oral exposure to Al in drinking water and AD [92][183]. According to Martyn et al. [93][184], AD is more prevalent in regions with high levels of Al in their drinking water. In conclusion, even though Al has been proposed as a potential risk factor for AD, there is insufficient evidence to support a causal relationship. Many studies have investigated the association between oral exposure to Al in drinking water and AD; however, more research is required to better understand how genetic, environmental, and lifestyle factors influence the onset and progression of AD.
3. Essential Metals in Alzheimer’s Disease
The homeostasis of essential metals is altered in AD patients [94][95][96][26,27,28]. This term refers to metals that are naturally present in the body and play a role in the function of numerous proteins and enzymes or act as second messengers. Sodium (Na), Ca, and magnesium (Mg) are the most abundant essential metals in the human body, while Fe, Cu, Zn, molybdenum (Mo), cobalt (Co), Mn, and chromium (Cr) are present in trace amounts. Many previous studies have also demonstrated the association between essential metals (primarily Fe, Cu, and Zn) and AD pathological changes.
3.1. Iron
Many biological processes in the body including the brain are regulated by Fe ions. Fe is essential for protein synthesis [97][197], cell growth and differentiation [98][99][198,199], the regulation of Fe-dependent enzymes [100][200], oxygen transport [101][201], and the electron transfer chain in oxidation–reduction reactions [101][201]. Fe is also crucial for the processes of myelination [102][202], development [103][203], and the function of numerous neurotransmitter systems [104][204]. Both amyloid plaques and NFTs have been found to have elevated Fe concentrations [105][205]. Fe is also involved in oxidative stress and the formation of reactive oxygen species in the brains of AD patients via the Fenton reaction [17][46]. Fe also promotes in vitro Aβ aggregation [106][206], tau protein phosphorylation [107][108][109][207,208,209], and tau aggregation [110][210] (Figure 1). It is interesting to note that APP is necessary for the persistence of ferroprotein (iron exporter) on the cell surface, and thus promotes Fe release [111][211].
In meta-analyses, a significant decrease in Fe levels was observed in the plasma [58][87] and serum [112][129] of AD patients, but no significant change was observed in the CSF [112][129]. In contrast, a number of studies observed a correlation between the Fe levels in CSF and various CSF AD biomarkers [45][113][114][74,188,193]. Nonetheless, in many observational studies, there was no difference in the Fe levels between the AD patients and controls.
3.2. Zinc
The brain has a higher Zn concentration than other organs [115][212]. Zn is essential for neurotransmission because, as an antagonist of glutamate NMDA (N-methyl-D-aspartate) receptors, it protects neurons from glutamate-induced excitotoxic damage [116][213]. Zn accumulates in amyloid plaques [117][214], binds to Aβ, and promotes Aβ aggregation and plaque formation [117][214]. Zn also promotes tau protein aggregation [118][215], phosphorylation [119][120][216,217], and translation [120][217] (Figure 1). In meta-analyses, however, a significant decrease in Zn levels was observed in the serum and plasma [121][123] as well as in the hair of AD patients [58][87], whereas there was no significant change in the CSF [121][123] and brain [122][115] levels. To date, MR studies have not identified Zn as a risk factor for AD [123][124][125][218,219,220]. An in vivo study demonstrated positive effects of Zn supplementation in mouse models of AD [126][221], and a small double-blind clinical trial observed the stabilization of cognitive abilities in AD patients after six months [127][222]. Thus, adding Zn to the diet has been suggested to improve the cognitive abilities of AD patients [128][223], whereas Loef et al. found no significant benefit of Zn supplementation in AD [129][224]. In addition, in vivo studies have shown that Zn supplementation promotes the formation of NFTs [130][225] and Aβ deposition [131][226].
3.3. Copper
Normal brain function requires optimal Cu levels, as indicated by the disruption of its metabolism. Patients with Menkes syndrome, for example, suffer from intellectual deficits and neurodegeneration. This disorder is caused by a sex-linked mutation of the ATP7A gene on the X chromosome (which encodes a protein involved in the transmembrane transfer of Cu ions) and is characterized by the decreased absorption of Cu in the intestine, and consequently, a decreased concentration of Cu in the cytosol of all body cells except in the intestines and kidneys [132][227]. In Wilson’s disease, excessive Cu accumulation in the body is associated with psychosis, parkinsonism, and dementia [133][134][228,229]. Cu homeostasis is also impaired in AD [96][28]. Cu promotes the formation and accumulation of Aβ-oligomers by binding to Aβ [12][41]. Cu chelation can prevent the cytotoxic effect of the Cu-Aβ complex [135][230]. Cu accumulates in plaques [136][137][231,232], and the interaction between Cu and APP has been demonstrated [137][232]. Cu can induce both the phosphorylation and aggregation of tau [13][14][42,43] (Figure 1) and its interaction with apolipoprotein E (ApoE) contributes to the pathogenesis of AD. ApoE2 has the highest binding affinity for divalent Cu, Zn, and Fe ions, while ApoE4 has the lowest [138][139][233,234]. In meta-analyses, Cu levels in the serum of AD patients increased significantly [58][140][141][142][87,92,122,133], whereas Cu levels in the brains of AD patients decreased [140][92]. Recent MR studies [123][125][218,220] have surprisingly found that higher Cu levels are protective against AD risk.
3.4. Calcium
Ca is an indispensable second messenger that regulates hundreds of signaling pathways crucial for the normal functioning of memory and cognition-related cells and networks [143][235]. Many neurodegenerative diseases including AD [144][236] are characterized by a disruption of cellular Ca signaling. The excessive entry of Ca ions through ionotropic glutamate receptors is a known mechanism of excitotoxic neuronal death [145][146][237,238]. Ca homeostasis disruption promotes Aβ and tau pathology [147][239]. However, human studies have produced contradictory results, with both decreased [148][149][240,241] and increased Ca [150][151][186,242] being risk factors. In recent MR studies, higher Ca levels were shown to reduce the risk of AD [149][152][241,243], or no association between Ca levels and AD risk has been observed [123][125][218,220].
3.5. Manganese
Mn is a crucial element for protein synthesis, lipid and glucose metabolism, and oxidative stress protection [153][244]. However, Mn is also an environmental toxin, and elevated Mn levels have been linked to diminished cognitive performance [154][155][156][187,245,246]. A rise in Mn levels has also been observed in patients with AD [157][109]. Nonetheless, a meta-analysis by Du et al. [158][89] revealed a significant decrease in Mn levels between AD and the controls.
3.6. Magnesium
Human studies have demonstrated that Mg deficiency impairs memory [159][247] and that Mg supplementation can improve memory in dementia patients [160][161][162][248,249,250]. In addition, a decrease in Mg concentration has been observed in the tissues of AD patients [163][164][251,252]. However, no change in Mg concentration was observed in the brains of AD patients in some studies (reviewed in [165][253]). Mg influences the processing and transport of APP, with low Mg levels favoring the β-secretase pathway and high Mg levels favoring the α-secretase pathway [166][254], whereas the treatment of experimental animals with Mg sulfate reduces tau phosphorylation and influences the maintenance of cognitive functions and synaptic plasticity [167][255]. According to the meta-analysis by Du et al. [158][89], the serum and plasma Mg concentrations were lower in the AD patients than in the controls, whereas the CSF Mg concentrations did not differ between groups. Thomassen et al. [168][95] did not find an association between the plasma Mg levels and the risk of AD in a study involving more than 100,000 participants. Kieboom et al. demonstrated that both low and high Mg concentrations were associated with an increased risk of dementia. They concluded that the relationship between Mg and the risk of dementia was U-shaped rather than linear [169][108].
3.7. Other Essential Metals
AD also perturbs the homeostasis of Na, K, and Co. Previous studies have associated elevated Na levels with AD [95][170][171][172][27,96,256,257]. Both increased [173][102] and decreased [174][195] K levels have been associated with AD, whereas in some studies, no change in the K levels was observed in AD. Co is an essential component of vitamin B12 and is an environmental toxin. Zheng et al. showed that mice exposed to Co develop age-related neurodegeneration [175][258].