Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Rosália Maria Pereira de Oliveira e Sá and Version 2 by Rita Xu.
Klinefelter syndrome (KS), caused by the presence of an extra X chromosome, is the most prevalent chromosomal sexual anomaly, with an estimated incidence of 1:500/1000 per male live birth (karyotype 47,XXY). High stature, tiny testicles, small penis, gynecomastia, feminine body proportions and hair, visceral obesity, and testicular failure are all symptoms of KS. Endocrine (osteoporosis, obesity, diabetes), musculoskeletal, cardiovascular, autoimmune disorders, cancer, neurocognitive disabilities, and infertility are also outcomes of KS.
- Klinefelter syndrome
- epidemiology
- etiology
- genetic causes
- metabolic syndrome
1. Definition and Clinical Aspects
Klinefelter syndrome (KS) is a congenital trisomy of male sex chromosomes, characterized by the presence of one or more extra X chromosomes [1][2][1,2], phenotypically presenting with testicular failure and hypergonadotropic hypogonadism [3][4][5][6][7][3,4,5,6,7].
About 80–90% of KS cases present a non-mosaic karyotype (47,XXY), while the remaining 10–20% evidence a mosaic karyotype (47,XXY/46,XY), higher grade aneuploidies (48,XXXY or 48,XXYY) or a structurally abnormal X chromosome (e.g., 47,iXq,Y), with mosaic cases originating a less severe KS phenotype [3][4][8][9][10][11][12][3,4,8,9,10,11,12].
KS is the most common chromosomal sexual anomaly and the most common chromosomal anomaly in men [3]. In a Danish population study of more than 2 million live births, the prevalence (existing cases) of KS was estimated to be about 0.15% (150:100,000 males) [13], varying with region and ethnicity [14], and the incidence (new cases) of KS was estimated to be around 1:500–1:1000 (0.1%–0.2%) male live births [7][9][13][7,9,13].
In its typical clinical picture, KS is phenotypically characterized by high stature (long limbs), small and hard testicles, small penis, gynecomastia (in late puberty), absence of body, pubic and facial hair, visceral obesity (feminine distribution of adipose tissue), eunuchoid body proportions (wide hips), and signs of androgen deficiency and infertility (mainly azoospermia) [15][16][17][18][15,16,17,18]. Patients with KS are diagnosed throughout their lives. Findings from a national survey of 200 patients with KS in Denmark showed that 20% were diagnosed prenatally, 35% were diagnosed during childhood, due to excessive growth and/or behavioral problems, and the remaining 45% were diagnosed in adulthood, typically as part of infertility evaluation [19].
In KS, hypogonadism is caused by a primary testicular disease. Hypergonadotropic hypogonadism is derived from structural and functional dysfunction of testicular Leydig cells (LCs) and Sertoli cells (SCs), and the hypothalamic–pituitary–gonad (HPG) axis. LCs present luteinizing hormone receptor (LHR) alterations, leading to luteinizing hormone (LH) resistance. This causes a subsequent decrease in testosterone (T) synthesis and secretion. Failure to respond to LH induces a state of elevated serum LH levels, which are thought to induce a compensatory LC hyperplasia; however, due to the small size of the testes and LC incompetence, LC hyperplasia does not compensate for the loss of androgen production. Normally, T exerts negative feedback over the hypothalamus, eliciting a decrease in gonadotropin-releasing hormone (GnRH) release. As GnRH acts over the adenohypophysis/anterior pituitary to induce the release of follicular stimulating hormone (FSH) and LH, this release is diminished. Additionally, T also exerts negative feedback on LH release from the adenohypophysis. These negative feedbacks are not observed in KS, which indicates the presence of a disrupted HPG axis, thus being also responsible for the rise in serum LH levels. Regarding the SC, these usually present receptors for androgens and FSH. By binding to the SCs, they elicit the synthesis and release of several molecules that act on the germ cells to induce and stimulate spermatogenesis. In KS, SCs do not respond to FSH, inducing a compensatory state of high serum FSH levels. FSH serum levels also remain high due to the SC decrease in the synthesis and release of inhibin-B, which would act on the adenohypophysis, where, by a negative feedback mechanism, it would lead to a decrease in the synthesis and release of FSH [20][21][22][23][20,21,22,23].
Low androgen levels are responsible for the observed androgen insufficiency (hypogonadism) in KS, with clinical features also dependent on other effects caused by an extra X chromosome [3][24][3,24]. Signs and symptoms may not always exist, their type and intensity vary, and their appearance also depends on the patient’s age, with the phenotype worsening with advancing age due to the cumulative influence of comorbidities [4][25][26][27][28][4,25,26,27,28]. Consequently, patients with KS exhibit a broad spectrum of phenotypes, with varying degrees of androgen deficiency severity [4]. Clinical characteristics of KS range from severe signs of androgen insufficiency to normally virilized men with just mild physical abnormalities, which explains why they do not receive clinical attention and are frequently underdiagnosed until adulthood, when they seek medical advice for infertility [10][12][10,12]. As a result, several patients who resort to infertility treatments are diagnosed here for the first time as having a 47,XXY karyotype. These patients have elevated FSH and LH serum levels but normal T serum levels. They do not exhibit signs and symptoms of decreased libido or androgenization, nor do they evidence endocrine, vascular, neurocognitive, or psychiatric disorders [29][30][31][29,30,31].
Newborn characteristics (length, weight and head circumference) are within normal limits, albeit slightly lower [30][32][33][34][35][30,32,33,34,35]. Subtle dysmorphic signs (fingers, palate, eyes) and congenital anomalies are uncommon and not pathognomonic [30][32][35][36][30,32,35,36]. They often present some degree of hypotonia, passive temperament, and developmental delays [30][35][37][30,35,37]. More frequently, genital anomalies (micropenis, cryptorchidia, bifid scrotum and hypospadias) are found [25][30][32][34][35][36][38][39][40][41][42][25,30,32,34,35,36,38,39,40,41,42]. These genital malformations are supposedly due to the effects of the extra X chromosome or androgen deficiency [3][4][3,4]. Longer legs [28][43][44][28,43,44] and speech disabilities [45][46][45,46] were attributed to the genetic abnormality rather than hypogonadism [3][4][16][39][3,4,16,39]. Small, hard testes are seen in all cases, and are caused by progressive tubulohyalinization and interstitial testicular fibrosis [1][3][4][16][30][39][1,3,4,16,30,39]. Hypogonadism also causes sexual dysfunction (decreased libido and erectile dysfunction) [3][4][47][3,4,47].
KS has multisystemic consequences, with higher morbidity and mortality than the general population, especially if not diagnosed and treated with T as early as possible [48]. Endocrine effects include osteoporosis, metabolic syndrome, obesity, and type 2 diabetes. It is also associated with musculoskeletal, cardiovascular and visual diseases, autoimmune disorders, cancer, neurocognitive disorders (learning disabilities), and behavioral disorders (psychosocial disturbances) [4][5][6][14][24][30][49][50][51][52][4,5,6,14,24,30,49,50,51,52].
Several metabolic disturbances are related to KS hypogonadism. Hypogonadism causes loss of muscle synthesis (causing a decrease in muscle mass), loss of glucose turnover (causing hyperglycemia), loss of fat turnover (causing fat deposition, truncal/visceral), and insulin resistance. Increased insulin resistance also produces LCs, aggravating the negative impact on T production [14][30][14,30]. Decreased muscle mass translates into decreased muscle strength and coordination, with hypotonia observed in most children. A metabolic syndrome develops as a result of an increase in fat mass, which is associated with increased serum levels of leptin (adipocyte-produced hormone) and ghrelin (gastro-pancreatic hormone that regulates hunger), hyperglycemia, increased insulin resistance (associated with development of type 2 diabetes), and dyslipidemia [14][30][14,30].
This metabolic state promotes the development of cardiovascular diseases, with a higher prevalence of atherosclerosis, arterial hypertension, myocardial infarction, stroke, arrhythmia, and heart failure. As T acts as a vasodilator, tissues tend towards a vasoconstrictor state due to decreased T levels, aggravating cardiovascular diseases. Low T levels and the metabolic syndrome, on the other hand, cause changes in hemostasis (clotting factors), which favor the development of thrombophlebitis, pulmonary thrombosis, and lower limb ulcers. The main hypothesis proposes that insulin resistance, obesity, and the metabolic syndrome increase plasminogen activator inhibitor (PAI) levels, conducting to a decreased fibrinolytic state (blockage of thrombus formation) [14][52][53][14,52,53]. PAI glycoprotein is a physiological inhibitor of tissue-type and urokinase-type plasminogen activators. Because these enzymes convert inactive plasminogen into plasmin, which then degrades fibrin, increased levels of PAI inhibit fibrinolysis, favoring thrombolysis [54][55][54,55].
Endocrine disorders also lead to abnormalities in bone metabolism, resulting in osteoporosis and tooth defects. In addition to hypogonadism, decreased lean body mass (all tissues and organs except fat body mass) and increased adiposity have been associated with low bone mass. Low bone mass is also associated with low levels of vitamin D (which ensures calcium ion absorption, facilitating calcium deposition in bones) in KS cases. Patients also evidence increased bone resorption. Bone resorption is mediated by the hormone insulin-like peptide 3 (INSL3), released by LCs in response to LH stimulation. INSL3 stimulates bone anabolism by acting on osteoblasts. However, individuals with KS have low serum levels of INSL3 due to LC insufficiency, which stimulates the secretion of sclerostin, which will exert catabolic effects on osteoblasts, favoring osteoporosis [56].
Patients with endocrine disorders and the metabolic syndrome are more likely to develop sexual dysfunction (erectile dysfunction and premature ejaculation), which can result in libido loss, anxiety, and depression [7][14][7,14].
Patients with KS may have neurocognitive deficits, including a decrease in intelligence quotient without loss of intellectual capacity, a delay in the development of complex learning and experience skills, and verbal deficits (verbal memory, processing speed, and vocabulary), which include language receptive skills (comprehension, ability to decode the meaning of words using auditory discrimination and processing, which depends on auditory capabilities and semantic memory) and expressive language skills (expression using the vocal motor part, which includes speech vocalization, articulation, and verbal fluency), deficits in reading and writing (dyslexia leads to comprehension and communication difficulties), and deficits in cognitive control processes (organization, planning, judging, decision-making, focused and sustained attention over time, inhibition of irrelevant information and information processing). Patients may have reduced attention, working memory, and cognitive flexibility, as well as a reduced capacity to evaluate facial expressions and form interpersonal relationships. Intriguingly, brain structure research demonstrated a reduced brain volume due to gray and white matter loss [14][30][57][14,30,57].
In general, patients report that the disease has a negative impact on their quality of life since childhood (physical, psychosocial, emotional, and social), pointing to decreased vitality and general health, insomnia, lower-paying jobs, greater difficulty in living with a partner, increased medication needs, and infertility [49].
In KS patients, various psychiatric illnesses such as schizophrenia, bipolar disorder, autism, attention deficit hyperactivity disorder, depression, and anxiety are more commonly documented [30][58][59][30,58,59].
KS is also associated with an increased prevalence of autoimmune diseases (Addison’s disease, type 1 diabetes, multiple sclerosis, rheumatoid arthritis, disseminated lupus erythematosus, and Sjögren’s syndrome) and cancer (breast, mediastinal, and hematological). Although no gene or genetic mechanism has been identified, this increase is most likely due to additional X chromosomal material, [14][30][14,30].
2. Testicular Sperm Retrieval
Male infertile individuals with severe oligozoospermia or secretory azoospermia may be able to father children with the development of ICSI [60][61][62][152,153,154] and testicular sperm extraction (TESE) [63][64][65][66][67][155,156,157,158,159]. The existence of focal spermatogenesis in KS patients also has allowed for successful spermatozoa recovery (SSR) from the seminiferous tubules [68][69][70][160,161,162]. The spermatozoa retrieval rate (SRR) in adolescents (15–19 y) and young adults (20–24 y) was 52%, 40–66% in adults and 30% in cases of cryptorchidism [31][71][72][73][31,89,163,164]. The kind of spermatogenesis failure with the SRR was specified in some instances. Although 38 (76%) of 50 KS patients had tubular sclerosis and atrophy, 9 (18%) had complete or incomplete germ-cell aplasia (only SC), and 3 (6%) had complete or incomplete maturation arrest, authors were able to retrieve spermatozoa in 24 (48%) of these cases. Unfortunately, authors did not specify the testicular phenotype in relation to successful sperm retrieval [74][165]. Another report of 47 KS patients revealed 34 cases with SCs alone (71% SRR), 9 with LC hyperplasia alone (33% SRR), 1 with maturation arrest (without sperm retrieval), and 3 with focal spermatogenesis (67% SRR) [75][166]. In another study of 45 KS patients, 58% of total SRR was obtained, with 29 (64.4%) cases presenting tubular sclerosis and atrophy (59% SRR), 12 (26.7%) presenting complete germ cell aplasia–LC hyperplasia (50% SRR), and 4 (8.9%) presenting maturation arrest (75% SRR) [76][167]. Another report of 6 KS patients with 35% of total SSR revealed 1 case with hypospermatogenesis and 5 cases with only SCs [77][168]. In a study of 9 KS patients, 6 presented only SCs (64% SRR), 2 presented foci of spermatogenesis (100% SRR), and 1 evidenced only LC hyperplasia (without sperm retrieval) [78][169]. These observations suggested that even in KS patients with a negative histopathological finding, a focus of spermatogenesis might be found.2.1. Predictive Factors of Testicular Sperm Retrieval
Several markers were described in non-mosaic KS cases to characterize their androgen insufficiency and spermatogenesis dysfunction in comparison to the healthy population [79][80][81][82][83][84][85][128,136,170,171,172,173,174]. There are currently no clinical or biological parameters that can predict an SSR with certainty in these KS patients. However, several patient characteristics were shown to be related to SSR cases as compared to unsuccessful sperm retrieval cases. Several studies found a significant increase in SSR with lower age [29][76][77][86][87][88][89][90][91][92][93][94][29,167,168,175,176,177,178,179,180,181,182,183], lower time of infertility [29], lower age, lower FSH levels, and high T levels [93][182], higher testicular volume and higher T levels [95][96][184,185], higher T levels [91][93][97][180,182,186], presence of 46,XY spermatogonia [98][103], higher androgen-binding protein levels [98][103], and with lower LH levels and higher T levels [92][181]. Other studies, on the other hand, did not find a significant increase in the SSR with regard to age, testicular volume (decreased), FSH (increased), and T (normal) levels [99][100][187,188], as well as in testicular echogenicity and intratesticular blood flow resistance [101][94]; age, testicular volume, FSH, LH (increased), and T (normal) levels, as well as in the FSH:LH ratio or in the androgen sensitivity index (LH x T) [74][165]; age, testicular volume, FSH, and T (decreased) levels [102][189]; testicular volume, FSH, LH, and T (low-normal) levels [86][103][104][175,190,191]; testicular volume, FSH, LH, and T (normal) levels [76][104][167,191]; age, testicular volume, FSH, LH, T (decreased), PRL (normal), E2 (normal) and inhibin (decreased) levels [105][192]; testicular volume, FSH, LH, T levels (low-normal), and PRL (normal) levels [77][168]; testicular volume, FSH, and inhibin B (decreased) values [89][178]; age, testicular volume, FSH, LH, and T (normal) values [106][193]; FSH and LH levels or serum inhibin B (decreased) levels [89][107][178,194]; FSH and LH levels [91][180]; or age, time of infertility, hormone levels, number of fragments at TESE, time of search at TESE [31]. Other studies were conducted to identify potential spermatogenesis markers, but without comparing cases with SSR versus cases with unsuccessful sperm retrieval. These included the findings of decreased testicular volume [108][195], decreased testicular volume, increased FSH and LH levels, and decreased T levels [70][109][110][111][162,196,197,198]; decreased testicular volume, high levels of FSH and LH, with normal T values [112][113][114][105,199,200]; increased levels of FSH and LH, slightly increased levels of PRL, with normal values of T and E2 [115][201]; increased levels of FSH and LH, normal levels of PRL and decreased T levels [116][117][118][202,203,204]; decreased testicular volume, high levels of FSH and LH, with normal PRL and T levels [119][205]; and decreased testicular volume, increased FSH levels, and decreased inhibin B levels [120][95]. The goal of T replacement therapy in young boys (early-to-mid-puberty) with KS is to promote linear growth, increase muscle mass, preserve bone density, and allow for the development of secondary sexual characteristics [121][206]. Although T replacement therapy improves symptoms of androgen insufficiency caused by KS, it also inhibits spermatogenesis at the spermatogonia stage in adults. Furthermore, while T may aid in LH suppression, LC synthesis of the germ cell protector INSL3 will be decreased [3][33][3,33]. Adult T replacement therapy should thus be used solely in patients who are not interested in infertility treatments and have androgen deficiency. It should be discontinued for at least 4–6 months prior to infertility treatment if used [83][84][172,173].2.2. Techniques of Testicular Sperm Retrieval
Many KS patients have sought infertility treatment as adults, with no other symptoms or signs besides infertility. These patients had decreased testicular volume, high FSH and LH mean serum levels, and normal or slightly lower T concentrations. This group of patients did not belong to the main group (65–85%) of KS patients reported as having low T levels [82][171]. For patients, the testicular SRR is critical. Previous reviews showed a mean SRR of 44% [9], with a range of 30–70% [10]. This observed variability in the SRR suggests a possible effect of the different number of patients studied, retrieval technique, and differences in patient characteristics. According to studies, non-mosaic KS patients with low T levels should be treated with aromatase inhibitors first to decrease E2 levels and therefore enhance T intratesticular availability. This was suggested to potentially improve spermatogenesis in KS cases with foci of spermatogenesis [83][172]. When applied to men with low T levels or low T:E2 ratios, a higher retrieval rate (66%) has been reported using pre-treatment with aromatase inhibitors to equilibrate the T:E2 ratio [70][75][88][162,166,177]. However, these success rates could also be attributed to the simultaneous use of microsurgical testicular sperm extraction (mTESE). Because of the scarcity of research in KS patients and the absence of comparisons between conventional TESE (cTESE) and mTESE in patients treated with aromatase inhibitors, this kind of treatment is not routinely followed in cases with low T levels and high FSH and LH values. In fact, there have been cases of SSR after cTESE in patients with slightly low T levels who did not receive aromatase pre-treatment (29, 31). Nevertheless, aromatase treatment should be administered in those circumstances [88][93][177,182]. The mTESE [122][207] is a very promising TESE procedure, presenting high rates of SSR (47–69%) in KS patients [75][76][86][87][88][90][96][103][105][111][114][123][124][166,167,175,176,177,179,185,190,192,198,200,208,209], though none of these reports compared mTESE to cTESE. Although not in KS patients, both approaches were compared in the pioneering work of Schlegel [122][125][207,210], with authors obtaining an SRR of 63% by mTESE vs. an SRR of 41% by cTESE. There have been very few reports comparing cTESE to mTESE in KS patients. A study compared 28 cases using cTESE (50% SRR) to 10 cases with mTESE (10% SRR) [106][193]. Another report compared 23 cases using cTESE (0% SRR) to 20 cases with mTESE (33% SRR) [97][186]. A third report compared 43 cases using cTESE (51% SRR) to 40 cases with mTESE (33% SRR) [99][187]. In cTESE (37 reports), the SRR was 44% (228/516), with a range of 16–100%. There were 3 reports with ≥50 KS cases (SRR of 38, 40, and 48%) [29][31][74][29,31,165], with none presenting an SRR greater than 50%. Of the other 34 cases, there were 16 case reports with 100% SRR [20][23][65][70][110][111][115][116][117][118][119][126][127][128][129][130][20,23,88,104,157,162,197,198,201,202,203,204,205,211,212,215], one with 4 patients and 75% SRR [120][95], one with 18 cases and 28% SRR [107][194], one with 19 cases and 21% SRR [101][94], another with 5 patients and 20% SRR [131][218], one with 25 patients and 16% SRR [102][189], and 13 reports exhibited an SRR of 30–57% [68][69][72][77][89][95][98][112][132][133][134][135][136][103,105,114,115,118,160,161,163,168,178,184,213,214]. In mTESE (18 reports), the SRR was 43% (427/991), with an SRR range of 17–100%. There were 7 reports with ≥50 KS cases (SRR of 20, 28, 33, 43, 47, 57, and 66%) [76][88][91][92][93][96][167,177,180,181,182,185], of which 2 cases presented an SRR of more than 50% (57, 66%) [76][88][167,177]. The other 11 KS cases evidenced SRRs ranging from 17% [104][191] to 40–74% [75][78][90][105][123][137][138][139][166,169,179,192,208,217,219,220], with 2 cases displaying a 100% SRR, one with 2 patients [114][200] and the other with 9 patients [140][216]. The mTESE requires a surgical unit and specialized equipment, is aggressive (the testis is completely opened transversally), complex, time-consuming, and expensive. Many authors perform cTESE in a surgical unit, and the procedure is also time-consuming and expensive, as multiple testicular openings are performed if spermatozoa are not found [94][183]. A very efficient modified cTESE procedure, on the other hand, involves spermatic cord block (local anesthesia) in an outpatient setting (without a surgical unit), with a single 1 cm scrotum excision to reach the tunica vaginalis space. Thereafter, a 0.5 cm incision is made to expose the seminiferous tubules, followed by a biopsy of a small fragment (1–2 mm) that is immediately examined for spermatozoa. Wherever necessary, the testis is simply rotated exposing its different faces, eliminating the need for additional scrotal incisions. The procedure takes about 30–45 min and no complications were observed [29][31][29,31]. cTESE, like mTESE, requires the services of a highly skilled experienced urologist (Figure 1).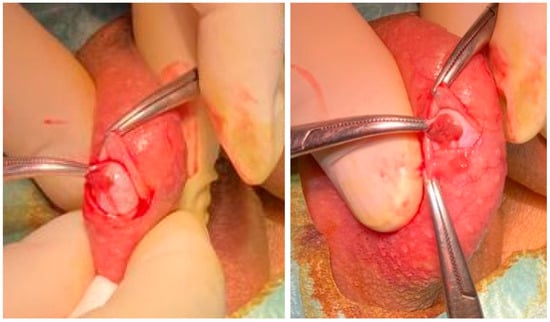
Figure 1. Outpatient conventional TESE employing local anesthesia using the three-finger technique and spermatic cord block. Left. Exposure of the tunica albuginea after entering the tunica vaginalis space. Right. Exposure of the seminiferous tubules.