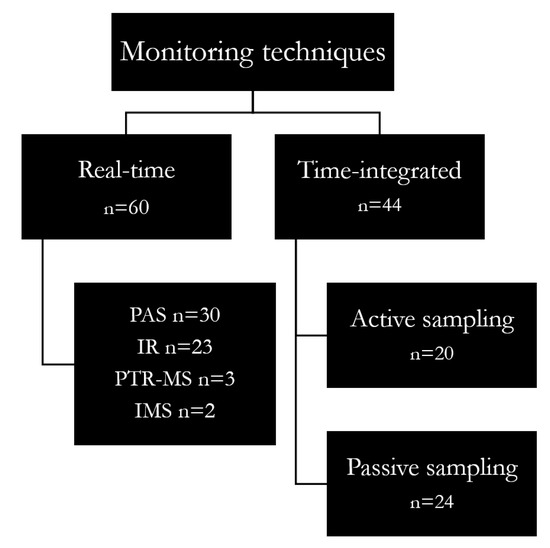
Other real-time techniques can be used for real-time WAGs monitoring, such as the proton-transfer-reaction mass spectrometry (PTR-MS) and ion mobility spectrometry (IMS).
2.2.2. Time-Integrated Sampling
In a considerable part of the selected articles (39%), anaesthetic gas concentrations were collected through time-integrated approaches allowing the collection of information about the average concentration throughout an entire work shift (about 8 h), which is well-suited for long-term exposure assessment. In such a case, sampling methods can be classified as active (44%) or passive (56%).
In general, active sampling of anaesthetic gases is performed using sorbent tubes packed with a suitable material (e.g., Anasorb 747, XAD-2 or ORBO-33) and connected to a low-flow sampling pump. Direct air sampling using collection containers (e.g., the FKV Bottle-Vac) or Nalophan bags was also used in a few cases. Active sampling works by means of a pump which, connected to the sample collector, sucks the air that passes through the absorber for WAGs collection.
Passive or diffusive sampling requires a longer sampling time than the active sampling to collect the same amount of analyte, but is characterized by ease of use and cheapness
[40][41][63,71]. Specifically, the SKC VOC-Check, 3M 3500, Draeger Orsa 5, Zambelli TK200 and ISC Maugeri Radiello
® were used. Furthermore, diffusive sampling is particularly suitable for use in the operating room because of its very small size
[21]. The sampling time varies upon the sampler type, the chemical of interest and the expected concentrations, for instance from less than 1 h to some weeks.
Either active or passive sampling implies sample collection onto collection media, which must be subsequently analysed in a laboratory, typically by gas chromatography after chemical or thermal desorption.
Chemical desorption is usually carried out with carbon disulfide. Instead, thermal desorption is a two-stage process occurring at high temperatures (100–300 °C) and using cold traps as refocusing devices. Desorption is followed by capillary gas chromatography, with mass spectrometric of flame ionization detection
[42][43][44][45][72,73,74,75]. These approaches allow us to obtain the most reliable long-term exposure data for testing compliance with 8 h time-weighted average occupational exposure limit values (e.g., TLV–TWAs). Available studies outlined that gas chromatography is generally used for sample analysis (95%). However, in a few cases, samples collected in reservoir bags were analysed by infrared spectrometry
[31][46][45,76].
2.2.3. Real-Time vs. Time-Integrated Monitoring
In recent years, there has been an increasing use of real-time analysers (PAS and IR monitors) compared to time-integrated approaches (active and passive sampling), probably because these techniques allow immediate feedback of exposure levels as well as the identification of the work phases and practices most at risk, also making possible an immediate adjustment of incorrect risk management practices
[47][77].
In fact, more and more portable real-time instruments have been developed and are now available on the market, which allows the acquisition of the best dataset for short-term exposure assessment (peak exposures). As an example, portable gas chromatographs can be regarded as promising techniques for real-time monitoring of gas at fixed positions in the environment
[48][78]. This method can quantify the air concentrations of anaesthetic agents offering a simultaneous, selective and continuous monitoring of several different halogenated gases in a single analytical run. These instruments also offer modular arrangements so that various detectors can be used. The most sensitive monitor is based on mass spectrometry (GC-MS), which delivers lab-quality results in minutes.
It is worth noting that, in some cases, time-integrated and real-time approaches were combined
[31][49][50][45,79,80], using a diffusive or active sampling for personal monitoring and a real-time monitor placed in a fixed position to measure air contamination in different operating rooms or also in different areas of the same one. In particular, real-time approaches (e.g., photoacoustic spectroscopy, ion mobility spectroscopy, infrared spectroscopy, portable gas chromatography (GC)) can be useful to investigate exposure profiles and to identify exposure peaks, which is crucial to assess short-term exposures by comparison with short-term exposure limits
[51][81]. However, the real-time methods are generally less reliable (in terms of accuracy, sensitivity, precision and specificity to the chemical/variable of interest) if compared to reference-grade methods
[52][82]. Overall, real-time methods are being successfully used complementary to reference monitoring, but they are not yet validated as alternative techniques for reference instruments. On the other hand, time-integrated measurements, typically based on diffusive or active sampling and following GC analysis, are recommended for a robust determination of 8 h averaged exposures and can be very useful for the a posteriori correction of real-time data to achieve better accuracy.
3. Conclusions
In conclusion, despite the observation that environmental monitoring is dominant, it may be useful to combine it with biomonitoring to get a complete picture for risk assessment purposes, including biomarkers of early effects. For this reason, it would be very important to identify valid biomarkers of exposure to complement environmental monitoring information to be used in the practice of occupational hygiene. Furthermore, since sevoflurane is increasingly used in anaesthetic practice, it is important to derive health-based limit values for sevoflurane capable of protecting workers from acute and chronic effects. Real-time techniques are mostly used with sampling intervals consistent with the considered limit value (e.g., the NIOSH REL, 60 min). However, it can be also useful to measure the WAGs by a real-time analysis combined with a contextual time-integrated monitoring to improve accuracy and obtain the most reliable data for testing the compliance with 8 h occupational exposure limit values (e.g., TLV–TWAs) as well as for risk management purposes. As a general rule, it is very important to know in detail the uncertainty of exposure measurements and/or some analytical figures of merit such as the analytical specificity, precision and accuracy for a reliable identification of exposure events/patterns and for a sound quantification of health risks
[53][83].