Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Prattana Punnakitikashem and Version 2 by Dean Liu.
eHealth or digital health innovations expanded tremendously during the COVID-19 pandemic. Innovation and digitalization offer creative solutions to build up a healthy society. The eHealth technologies are quickly taken up by Southeast Asia countries and continue to flourish to alleviate the burden of healthcare challenges.
- e-health
- bibliometric review
- electronic health
1. Introduction
In the contemporary era, the world has been disrupted by digital technologies. With no exception in the healthcare industry, innovation and digitalization deliver promising solutions to build up a healthy society by fostering equitable, affordable, and universally accessible healthcare [1][2][1,2]. Since 2005, the World Health Organization has encouraged nations to use digital health strategies in their health system [3]. With the proper implementation, digital health technologies can escalate the progress toward Universal Health Coverage and health-related Sustainable Development Goals [2][4][2,4].
The term “eHealth” denotes the digital health technologies or the use of emerging information and communication technologies (e.g., Internet, artificial intelligence, big data, mobile device) to improve health and the healthcare system [5][6][7][5,6,7]. There are several subdomains under its broad scope, including telehealth, telemedicine, mHealth, wearable healthcare devices, health information technologies, and robotic and personalized medicine [8][9][8,9]. These technologies have significantly dominated the health system by connecting patients, families, and healthcare providers and enhancing patient-centered care delivery. The world is also receiving help from eHealth to solve the increasing healthcare demand by the aging global population.
Moreover, the recent COVID-19 pandemic highlighted the benefits of telemedicine and other forms of e-medical care [10][11][10,11]. Given the rapid spread of the coronavirus from person to person during the COVID-19 pandemic, hospitals are overwhelmed with virus-infected patients. Governments imposed large-scale lockdowns across the countries to reduce social contact and further spread the virus. However, the news reported that these extensive lockdown measures inflicted the health system as patients cannot easily and timely access the healthcare providers. Thereby, eHealth technologies are mushrooming as they can alleviate the tremendous burden on medical resources and minimize the amount of person-to-person contact required for treatment [12][13][14][12,13,14].
In Southeast Asia, the enhancement of the eHealth strategy was designated as one of the significant public service priorities by the ASEAN Digital Master Plan 2025 [15]. Southeast Asian countries are increasingly taking up eHealth services. Furthermore, eHealth’s implementation fulfills consumers’ rising demand for better healthcare services, especially amid the COVID-19 pandemic [16][17][18][19][16,17,18,19].
2. Intellectual Structure of the eHealth Literature in Southeast Asia
Co-citation analysis measures the similarity between authors, documents, or journals in the field of study. It refers to the frequency with which two units are cited together. The fundamental assumption underlying this analysis is that the more two items are co-cited, the more likely their content is related [20][21][23,63]. By using VOSviewer software, this bibliometric review conducted author co-citation analysis (ACA) to identify the intellectual structure of eHealth in Southeast Asia. Table 1 presents the highly co-cited authors in the eHealth in Southeast Asia literature. In addition, Figure 1 illustrates the ACA map by using the VOSviewer setting at a threshold of at least 23 author co-citations, which yielded a display of 86 scholars on the co-citation map. The size of the bubbles indicates the co-citation frequency. The larger the bubble means, the greater the scholars’ influence in the field of eHealth in Southeast Asia. The colored clusters represent schools of thought, which are the collection of items with similar theoretical perspectives and research interests. There are four distinct, coherent schools of thought in the literature on eHealth in Southeast Asia: “technology for healthcare and disease management” (red cluster with 39 items), “analysis and adoption of hospital information system/eHealth records” (green cluster with 22 items), “user intention and acceptance of information technology” (blue cluster with 15 items), and “m-Health” (yellow cluster with ten items).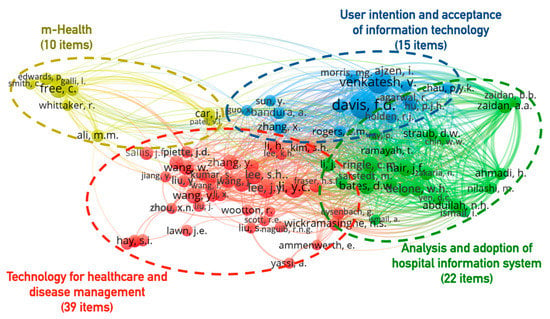
Figure 1. Four clusters representing the intellectual structure of eHealth in Southeast Asia (Threshold 23, Display 86 Authors).
Table 1. Highly co-cited authors in eHealth in Southeast Asia.
| Rank | Author | Nation | Co-Citation | Topical Focus |
|---|---|---|---|---|
| 1 | Davis, F.D. | United States | 112 | User intention and acceptance of IT |
| 2 | Venkatesh, V. | United States | 75 | User intention and acceptance of IT |
| 3 | Li, Y.C. | Taiwan | 70 | Technology for healthcare and disease management |
| 4 | Lee, J.Y. | United States | 58 | Technology for healthcare and disease management |
| 5 | Free, C. | United Kingdom | 53 | m-Health |
| 6 | Ajzen, I. | United States | 50 | User intention and acceptance of IT |
| 7 | Hair, J.F. | United States | 46 | Analysis and adoption of hospital information system |
| 8 | Ringle, C.M. | Germany | 45 | Analysis and adoption of hospital information system |
| 9 | Bates, D.W. | United States | 44 | Analysis and adoption of hospital information system |
| 10 | Lee, S.H. | United Kingdom | 44 | Technology for healthcare and disease management |
| 11 | Wang, Y. | Canada | 44 | Technology for healthcare and disease management |
| 12 | Wang, J. | United States | 42 | Technology for healthcare and disease management |
| 13 | Wang, W. | Singapore | 41 | Technology for healthcare and disease management |
| 14 | Zhang, Y. | China | 41 | Technology for healthcare and disease management |
| 15 | Delone, W.H. | United States | US | Analysis and adoption of hospital information system |
| 16 | Sarstedt, M. | Germany | 39 | Analysis and adoption of hospital information system |
| 17 | Zhang, J. | Singapore | 38 | Technology for healthcare and disease management |
| 18 | Li, H. | Finland | 36 | Technology for healthcare and disease management |
| 19 | Li, J. | Australia | 36 | Technology for healthcare and disease management |
| 20 | Zaidan, A.A. | Malaysia | 36 | Analysis and adoption of hospital information system |
3. Topical Foci of the eHealth in Southeast Asia Knowledge Base
Keyword co-occurrence analysis, also called co-word analysis, identifies key themes and topics within the eHealth in Southeast Asia knowledge base. Co-word analysis frequently identifies co-occurring words in the titles, abstracts, and indexes of documents in the review database [20][23]. This analysis would offer insight into broad topical trends within the literature. Figure 2 shows the density map of the most frequently occurring keywords in the literature: healthcare delivery (316), telemedicine (308), health information system (243), medical information system (164), m-health (162), electronic health record (141), geographical information system (135), public health (124), hospital (120), elderly (115), organization and management (105), and covid-19 (100). These frequently occurring keywords offer insight into the subjects of studies that describe the eHealth in Southeast Asia knowledge base since its emergence in the past four decades.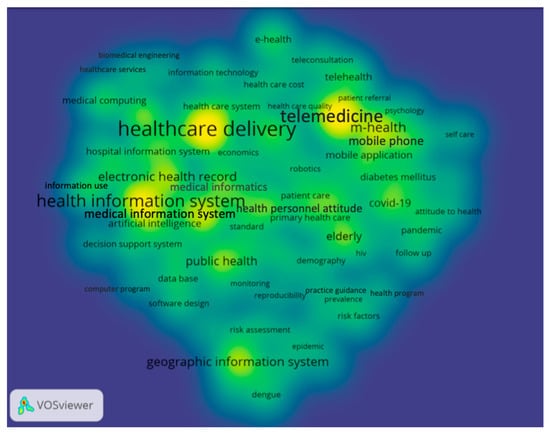
Figure 2. Keyword density heat map of the eHealth in Southeast Asia literature, 1975–2021 (Threshold 25 Occurrences, Display 94 Keywords).
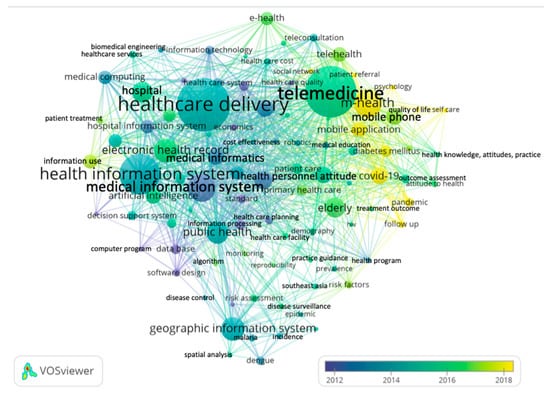
Figure 3. The temporal co-word map of the eHealth in Southeast Asia literature, 1975–2021 (Threshold 25 Occurrences, Display 94 Keywords).