Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Casandra-Maria Radu and Version 2 by Rita Xu.
The extensive use of antibiotics has resulted in the development of drug-resistant bacteria, leading to a decline in the efficacy of traditional antibiotic treatments. Essential oils (EOs) are phytopharmaceuticals, or plant-derived compounds, that possess beneficial properties such as anti-inflammatory, antibacterial, antimicrobial, antiviral, bacteriostatic, and bactericidal effects.
- essential oils
- therapeutic effect
- oral microbiome
- phytopharmaceuticals
1. Introduction
Microbes were discovered in the early 18th century and are prevalent in our environment, affecting every aspect of human life. The oral cavity is home to various microorganisms and habitats that play a crucial role in overall human health. Imbalances in the microbial flora can lead to oral diseases such as dental cavities, periodontitis, gingivitis, oral mucosa diseases, and systemic diseases [1]. Many attempts have been made to develop the ideal antimicrobial agent due to the emergence of antibiotic-resistant bacteria [2]. EOs have been studied for many years as potential antimicrobial agents and are used in various medical fields, including dentistry. In many countries, they are still used as traditional medicine. The earliest known use of EOs is believed to be in Ancient Egypt in 3500 B.C., where they were used in cosmetics, religious ceremonies, and medicinal purposes in various forms such as ointments, inhalations, powders, pills, and maceration extracts [3]. French chemist Rene-Maurice Gattefosse experimented with EOs for wound healing during World War I [4]. India and China also began using herbs as a medicine around the same time as Ancient Egypt, and currently, there is an increasing demand and interest in “natural medicine” due to concerns about synthetic drugs, fertilizers, and pesticides [5]. However, the use of aromatherapy for emotional and mental well-being gained popularity in the 1980s when research on mind–body healing and psychoneuroimmunology increased interest in the potential benefits of aromatherapy. It is commonly believed that certain scents can affect a person’s emotional state [6][7][6,7].
Approximately 3000 EOs are known to be used, and their use is increasingly studied now due to the need for alternative therapies for oral microbiome pathologies [8]. According to the World Health Organization, about 80% of the population uses herbal medicine, and its industrialization has highly increased [9]. EOs are effective as antioxidants, mostly because of their activity in food preservation [10], and they are known to possess anti-carcinogenic, antimicrobial, and anti-inflammatory properties due to over 200 constituents [11][12][11,12]. EOs are a mixture of volatile constituents produced by aromatic plants, serving as a protective mechanism against microorganisms [13]. Clove oil, also known as Eugenol in dentistry, is an aromatic oil extracted from cloves that have been proven to be very useful in root canal treatments in the past decade. However, many more EOs are now being studied for their therapeutic use, such as Tea tree oil, Thyme oil, Cinnamon oil, Citrus oil, Bergamot oil, Lavender oil, and Peppermint oil. In dentistry, the most common pathologies are bacterial and fungal, with pathogens such as Streptococcus mutans (S. mutans), Streptococcus salivarius (S. salivarius), Streptococcus sanguis (S. sanguis), Streptococcus sobrinus (S. sobrinus), Porphyromonas gingivalis (P. gingivalis), Prevotella intermedia (P. intermedia), Enterococcus faecalis (E. faecalis), Candida albicans (C. albicans), and Actinobacillus actinomycetemcomitans (A. actinomycetemcomitans) often modifying the oral microbiome and resisting other known therapies [2][14][2,14]. Increased bacterial resistance, the high costs of therapeutic procedures, and the many adverse effects have led to further research on traditional medicines obtained from plant sources [15][16][15,16]. Despite the widespread use of commercial drugs as trusted therapies, many people still use natural products for primary healthcare [17].
The oral cavity is a habitat for many microorganisms that form a complex structure, the biofilm, that adheres to teeth and oral epithelium. Oral diseases occur when there is an imbalance between the oral ecosystem and the biofilm; thus, the absence of microorganisms is preferred to maintain oral health [18]. As a result, natural agents have become necessary, making EOs great alternatives to antibiotics and other used therapies, such as photoactivation and lasers [19].
2. Composition
EOs, also known as “volatile oils,” are produced by aromatic plants as secondary metabolites and are characterized by their strong smell [20][36]. The chemical composition varies and depends on geographical location, botanical origin, genetics, bacterial endophytes, and extraction techniques [21]. They are synthesized from plants, especially from their leaves, fruits, resins, seeds, woods, barks, and berries, and they are known as “essentials” because they trap the essence of the plant, its taste, and its odor [22][37]. They have attracted the interest of research groups because they can be applied to the development of new solutions used for the improvement of oral hygiene [23][38]. EOs are complex substances that include hundreds of components [10] but are characterized by two or three significant compounds [24][39]. The main composition is made of hydrocarbon terpenes and terpenoids [25][26][25,40], and other common compounds are alcohols, acids, esters, epoxides, aldehydes, ketones, amines, sulfides, oxides, fatty acids, other sulfur derivates; the most critical ones for their activities are terpineol, thujanol, myrcenol, neral, thujone, camphor, carvone [27][28][20,41]. The majority of terpenoids consist of monoterpenes and sesquiterpenes, and the other group is oxygenated derivatives of hydrocarbon terpenes [25]. Due to their potential therapeutic benefits against various illnesses, monoterpenes have been the subject of extensive research [29][42]. EOs have been proven to be a valuable source of antitumor agents. In addition, their effectiveness in both mechanisms of action and clinical use in cancer treatment has been demonstrated [30][43]. The bactericide or bacteriostatic effects are due to terpenes and terpenoids, aromatic, and aliphatic constituents [31][44], and the antimicrobial activity is related to their composition, configuration, amount, and possible interactions [32][45]. The antimicrobial activities might also be due to their major phenolic or alcohol monoterpenes components [33][46], but Table 1 explains that in more detail.Table 1. EOs’ chemical compounds and their bacterial target.
Table 2. Dental diseases and EOs uses.
| Dental Disease | EOs | Therapeutic Effect | Reference | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dental cavities | Clove oil | Sesame oil | Cinnamon oil | Sumac oil | Citrus oil | antibacterial antimicrobial antifungal anticariogenic | ||||||||||
| [ | 36 | ] | [37] | [21,49,50] | ||||||||||||
| antiadhesion properties | [ | 22 | ][47][49][50] | [37,59,61,62] | ||||||||||||
| Periodontitis | Clove oil | Lavender oil | Lemongrass oil | Eucalyptus oil | anti-inflammatory antibiofilm growth effect |
[15][22][38][51] | [15,28,37,63] | Lavender oil | Linalool Terpineol Caryophyllene Limonene | |||||||
| Dental pain | Pinene |
Lavender oil | Clove oilS. aureus | C. albicans | E. coli | [38 | anxiolytic analgesic-like effect anti-inflammatory | ] | [22][39][40] | [28,51,52] | ||||||
| [ | 52 | ] | [53][54 | 66] | Cinnamon oil | Cinnamaldehyde Eugenol Linalool |
S. aureus | S. sobrinus | S. mutans | L. acidophilus | C. albicans | |||||
| Oral cancer | Clove oil | Cinnamon oilP. gingivalis | E. coli | anti-inflammatory antimutagenic cytotoxic immunomodulatory | [41][42] | [53,54] | ||||||||||
| ] | [ | 37 | ,64,65, | [55][56][57][58] | [67,68,69,70] | Eucalyptus oil | Pinene Limonene Terpineol |
S. aureus | S. mutans | [43][44] | [55,56] | |||||
| Lemon oil | Pinene Caryophyllene Linalool Citral Terpineol Limonene |
C. albicans | S. aureus | E. coli | [43][45][46] | [55,57,58] |
3. Applications
4. Therapeutic Properties
The applications of EOs depend on the plant source and are very diverse. They are also used in cosmetics and in the food and pharmaceutical industries. In addition, they have immunomodulatory effects by increasing the number of circulating lymphocytes [59][71]. A certain number of EOs have been reported to be antibacterial, antifungal, and anti-inflammatory agents against oral pathogens, and other therapeutic effects are shown in Figure 1 [60][72]. Additionally, they can alleviate anxiety, depression, and nausea [61][62][63][73,74,75].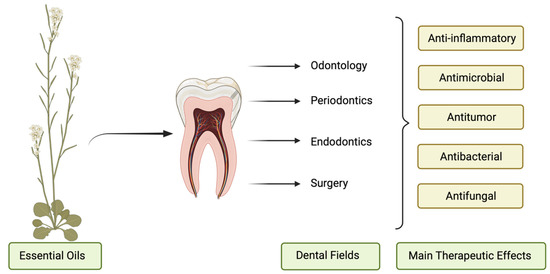
Figure 1. The therapeutic effects of EOs in diverse fields of dentistry.
5. Uses of EOs as Products in Dentistry
EOs are recognized as safe, and they stimulated searchers as a natural treatment of dental diseases [60][72]. However, despite the research progress that has been performed until now, studies regarding EOs’ approaching potential application in dentistry are still not discussed enough [13]. EOs are very useful in dentistry in the following fields: endodontics, periodontics, surgery, and oral prevention [68][80], and can be found in several dental products, as shown in Figure 2. They are known to be useful as oral hygiene adjuncts, anxiolytics, wound dressing, dental implants, and preservatives.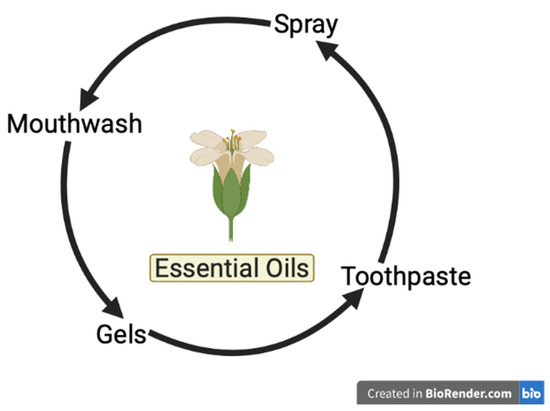
Figure 2. EOs found in dental products.