Dry eye disease (DED) is a widespread and frequently reported multifactorial ocular disease that not only causes ocular discomfort but also damages the cornea and conjunctiva. Topical administration is the most common treatment modality for DED. Due to the existence of multiple biological barriers, instilled drugs generally exhibit short action times and poor penetration on the ocular surface. To resolve these issues, several advanced drug delivery systems have been proposed.
Dry eye disease (DED) is a widespread and frequently reported multifactorial ocular disease that not only causes ocular discomfort but also damages the cornea and conjunctiva. Topical administration is the most common treatment modality for DED. Due to the existence of multiple biological barriers, instilled drugs generally exhibit short action times and poor penetration on the ocular surface.
1. Introduction
Dry eye disease (DED) is resulted from decreased tear production, excessive evaporation of tears, or both, ultimately leading to inflammation of the ocular surface
[1]. It is manifested by diverse and complex pathological processes. Presently, the association of these processes is not fully established. In 1995, the American Academy of Ophthalmology (AAO) classified DED into two subtypes, namely evaporative dry eye and aqueous-deficient dry eye. However, most patients with DED present symptoms of both subtypes
[2]. Epithelial lesions of the ocular surface, inflammation, and neurosensory abnormalities caused by DED can lead to the manifestation of diverse clinical symptoms, such as redness, pain, blurred vision, and sleep disorders. These discomforts not only reduce the patients’ productivity but also seriously affect their quality of life
[3][4][3,4]. Epidemiological studies reveal that the prevalence of DED is approximately 7% in Europe and America, 12.5–21.6% in Japan and Republic of Korea, and 21–30% in China. In some areas of Russia, the prevalence has been reported to be 40–55%
[5][6][7][8][9][5,6,7,8,9]. Aging, female gender, prior eye surgery, and widespread use of video terminals have been reported as high-risk factors contributing to the development of DED
[10]. China has a huge and aging population, where the prevention and treatment of DED are discouraging. With the significant progress in epidemiological studies of DED in recent years, it is recognized that DED has become an important public health concern
[11][12][11,12].
Presently, various treatment modalities, such as warm compresses, meibomian gland expression, intranasal tear neurostimulation, contact lenses, and topical medications have been prescribed for DED, among which the topical application of medications represents the most important one
[13][14][15][16][13,14,15,16]. However, multiple biological barriers on the ocular surface, such as the tear film barrier and the corneal and conjunctival barrier, result in rapid drug clearance and low bioavailability. Specifically, the presence of the tear film leads to rapid drug loss and the dense epithelium of the conjunctiva hinders drug entry
[17]. Cornea is in fact an amphiphilic tissue, the epithelium layer of which is hydrophobic, so it is difficult for hydrophilic drugs to stay or diffuse. However, if the drug has high lipophilicity, it is difficult for it to penetrate the hydrophilic stromal layer. As a result, drugs must have balanced hydrophilicity and lipophilicity to pass through the entire cornea
[18]. These determine that topically applied drugs generally demonstrate extremely low bioavailability. To improve the bioavailability of drugs in the eye, numerous drug delivery systems have been developed (
Figure 1)
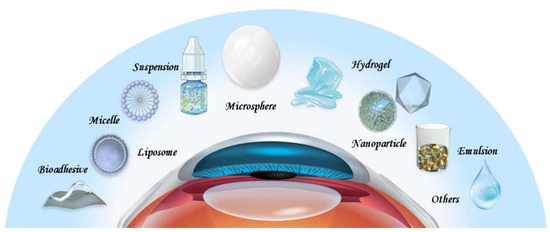
[19][20][21][19,20,21]. For example, nanoparticles are employed to improve the corneal penetration of drugs, hydrogels are employed to extend the retention time of drugs on the ocular surface, and microspheres are employed to achieve sustained release. While eye drops remain the most common delivery vehicles for DED drugs, drug-loaded implants, drug sprays, and microneedles are increasingly being explored. DED is characterized by a vicious cycle triggered by the multifactorial disruption of the ocular surface microenvironment, which leads to inflammation and decreased tear film stability
[22]. To ameliorate this chronic condition, long-term treatments are inevitable. However, the long-term use of medications can be associated with serious side effects. The DEWS II report suggests that short-term and long-term treatments should be combined flexibly for different patient conditions to maximize the therapeutic benefits
[23]. For patients with mild DED, the use of artificial tears alone can achieve satisfactory therapeutic effects. In contrast, for patients with moderate-to-severe DED, single or multiple drugs are often warranted. As a result, there is an attempt to improve the delivery of drugs with rationally designed drug delivery systems according to the properties of intended drugs and the disease conditions for better outcomes. Some of these delivery systems have led to innovative therapies which are under clinical investigation or even enter the clinic
[21][24][25][26][27][21,24,25,26,27].
Figure 1. Drug delivery systems for DED.
2. Drug Delivery Systems for DED
2. Drug Delivery Systems for DED
2.1. Suspensions
2.1. Suspensions
Suspension refers to a liquid formulation formed by dispersing insoluble drug particles in a liquid medium. Common methods for the preparation of suspension include direct dispersion, precipitation, and controlled flocculation. Drug particles in the suspension settle slowly at a rate that does not interfere with correct dosing. They do not agglomerate and can be dispersed evenly through shaking, even after long-term storage. After topical application, drug particles in the suspension can be retained in the cul-de-sac, which leads to prolonged ocular action duration [28]. The hydrophobic drugs currently used for the treatment of DED are often administered in this manner.
Suspension refers to a liquid formulation formed by dispersing insoluble drug particles in a liquid medium. Common methods for the preparation of suspension include direct dispersion, precipitation, and controlled flocculation. Drug particles in the suspension settle slowly at a rate that does not interfere with correct dosing. They do not agglomerate and can be dispersed evenly through shaking, even after long-term storage. After topical application, drug particles in the suspension can be retained in the cul-de-sac, which leads to prolonged ocular action duration [28]. The hydrophobic drugs currently used for the treatment of DED are often administered in this manner.
Alrex® (Bausch & Lomb, Clearwater, FL, USA) is an FDA-approved loteprednol etabonate suspension primarily used as an anti-inflammatory agent. Clinical trials have confirmed that DED can be treated effectively by monotherapy with this drug or combination therapy containing artificial tears [29,30]. Furthermore, suspensions of the immunosuppressant cyclosporine and the mucin-stimulating drug rebamipide have also been approved for treating DED [22,31]. In a randomized multicenter phase III study, 2% rebamipide suspension and 0.1% sodium hyaluronate were randomly instilled in 188 patients with DED, which demonstrated that the 2% rebamipide suspension was more effective in relieving foreign body sensation as well as eye pain [32].
Alrex® (Bausch & Lomb, Clearwater, FL, USA) is an FDA-approved loteprednol etabonate suspension primarily used as an anti-inflammatory agent. Clinical trials have confirmed that DED can be treated effectively by monotherapy with this drug or combination therapy containing artificial tears [29][30]. Furthermore, suspensions of the immunosuppressant cyclosporine and the mucin-stimulating drug rebamipide have also been approved for treating DED [22][31]. In a randomized multicenter phase III study, 2% rebamipide suspension and 0.1% sodium hyaluronate were randomly instilled in 188 patients with DED, which demonstrated that the 2% rebamipide suspension was more effective in relieving foreign body sensation as well as eye pain [32].
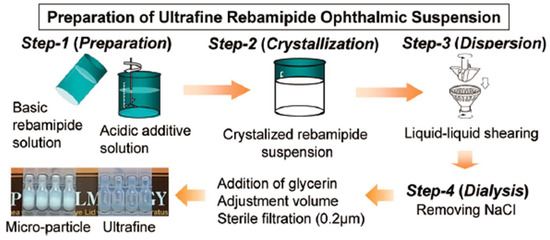
Although rebamipide suspension is advantageous for the treatment of DED, it is a milky liquid and blurs the patient’s vision temporarily, which reduces visual quality. To overcome this shortcoming, Matsuda et al. [33] formulated rebamipide particles into an ultrafine state (approximately 640 nm in size) to obtain a highly transparent (light transmittance: 59%) suspension (Figure 2). The duration of blurred vision was thus reduced. Moreover, an in vivo pharmacokinetics study revealed that the concentrations of rebamipide in cornea and conjunctiva were higher than those of conventional suspension, which indicated accelerated absorption rates and improved bioavailability. The particle size and transparency of this suspension remain unchanged for 3 years when stored at 25 °C, which demonstrated its excellent physicochemical stability. Augmenting the mucus-penetrating abilities of drugs represents another strategy to obtain improved outcomes. In this regard, Eysuvis® (Kala Pharmaceuticals, Arlington, MA, USA) is an original loteprednol nanosuspension developed by Kala using the AMPPLIFY mucus-penetrating particle drug delivery technology. This technology permits loteprednol to reach the ocular surface without being degraded in the tear film. A single application of Eysuvis® can increase the concentrations of loteprednol in the aqueous humor, cornea, and conjunctiva by up to three times compared with the commercial product Lotemax® (0.38% loteprednol etabonate eye gel, Bausch & Lomb, Clearwater, FL, USA). Eysuvis® showed high efficacy in DED treatment [34,35]. Moreover, a multicenter randomized clinical trial demonstrated it was safe and well-tolerated for short-term use (2–4 weeks) [36]. However, the long-term in vivo safety of it remains to be determined.
Although rebamipide suspension is advantageous for the treatment of DED, it is a milky liquid and blurs the patient’s vision temporarily, which reduces visual quality. To overcome this shortcoming, Matsuda et al. [33] formulated rebamipide particles into an ultrafine state (approximately 640 nm in size) to obtain a highly transparent (light transmittance: 59%) suspension. The duration of blurred vision was thus reduced. Moreover, an in vivo pharmacokinetics study revealed that the concentrations of rebamipide in cornea and conjunctiva were higher than those of conventional suspension, which indicated accelerated absorption rates and improved bioavailability. The particle size and transparency of this suspension remain unchanged for 3 years when stored at 25 °C, which demonstrated its excellent physicochemical stability. Augmenting the mucus-penetrating abilities of drugs represents another strategy to obtain improved outcomes. In this regard, Eysuvis® (Kala Pharmaceuticals, Arlington, MA, USA) is an original loteprednol nanosuspension developed by Kala using the AMPPLIFY mucus-penetrating particle drug delivery technology. This technology permits loteprednol to reach the ocular surface without being degraded in the tear film. A single application of Eysuvis® can increase the concentrations of loteprednol in the aqueous humor, cornea, and conjunctiva by up to three times compared with the commercial product Lotemax® (0.38% loteprednol etabonate eye gel, Bausch & Lomb, Clearwater, FL, USA). Eysuvis® showed high efficacy in DED treatment [34][35]. Moreover, a multicenter randomized clinical trial demonstrated it was safe and well-tolerated for short-term use (2–4 weeks) [36]. However, the long-term in vivo safety of it remains to be determined.
Figure 2. Schematic illustration for the preparation of rebamipide ultrafine suspension. Reprinted with permission from [33]. Copyright 2017 The Pharmaceutical Society of Japan.
2.2. Emulsions
Emulsion refers to a two-phase liquid in which the two phases are immiscible with each other. It generally consists of an aqueous phase (denoted by W), an oil phase (denoted by O), and an emulsifier. One phase is dispersed in the other in the form of small droplets, leading to a heterogeneous dispersion. The oil-in-water (O/W) emulsion serves as a good delivery vehicle for hydrophobic ophthalmic drugs, because the oil phase of it can be harnessed to dissolve poorly water-soluble molecules. As a result, improved ocular bioavailability is obtained [37]. Restasis® (Allergan, Waco, TX, USA), an O/W anionic nanoemulsion containing cyclosporine, is the first commercially available ophthalmic emulsion for DED. It is obtained by dissolving cyclosporine in castor oil using polysorbate as the emulsifier. The drug droplets of Restasis® spread easily on the ocular surface after instillation, thus allowing fast drug absorption and onset of action [38]. Emulsions also increase the solubility of hydrophobic drugs and offer ease of scale production in industrial settings [39].
Ikervis® is an O/W cationic nanoemulsion of cyclosporine developed by Santen Pharmaceutical (Osaka, Japan). The drug concentration of Ikervis® is the highest in the clinic. It is used in patients with severe DED that cannot be ameliorated by artificial tears. Because the emulsion droplets in Ikervis® are smaller than those in Restasis®, the penetration of cyclosporine into the cornea is enhanced. Moreover, the unique cationic Ikervis® can interact electrostatically with the negatively charged ocular surface, which prolongs residence time of the drug. The dosing frequency of Ikervis® is one time per day. This has been associated with improved patient compliance and therapeutic efficiency. A good safety profile of Ikervis® had also been demonstrated in a 12-month multicenter double-blind clinical trial [40]. Cationic emulsions are prone to cause local side effects, such as mild pain at the instillation site [41][42]. To improve eye comfort and bioavailability of the drug, Bang et al. developed self-emulsifying nanodrug delivery systems, namely, Cyporin-N (SNEDDS-N; Taejoon Pharma, Seoul, Republic of Korea) and T-sporin (SNEDDS-T; Taejoon Pharma, Seoul, Republic of Korea). SNEDDS is an anhydrous homogeneous mixture of oils, drugs, surfactants, and cosurfactants. Compared with the high turbidity and unstable pH of Restasis®, SNEDDS exhibits more uniform particle sizes, better light transmission, and more stable pH. The ability of SNEDDS to restore tear film stability is also superior to that of Restasis® [43]. Currently, SNEDDS has been developed in a variety of forms and diseases, such as solid SNEDDS, controlled-release SNEDDS, mucus-permeable SNEDDS, and targeted SNEDDS [44][45][46]. It is hoped that these innovative formulations will lead to a breakthrough in the management of DED. Apart from drug-loaded emulsions, drug-free emulsions have also been developed for DED. For instance, Cationorm® from Santen Pharmaceutical is a drug-free O/W cationic nanoemulsion. The benzylcetyldimethylammonium chloride presented in Cationorm® is a cationic surfactant that possesses intrinsic antimicrobial activity, which makes Cationorm® a preservative-free dosage form. This design enhances the safety of Cationorm®. Pharmacodynamic studies revealed that Cationorm® not only exhibited moisturizing and lubricating properties but also stabilized the tear film by its oily components, thus making it a safe and effective tear supplement [47][48].
Ikervis® is an O/W cationic nanoemulsion of cyclosporine developed by Santen Pharmaceutical (Osaka, Japan). The drug concentration of Ikervis® is the highest in the clinic. It is used in patients with severe DED that cannot be ameliorated by artificial tears. Because the emulsion droplets in Ikervis® are smaller than those in Restasis®, the penetration of cyclosporine into the cornea is enhanced. Moreover, the unique cationic Ikervis® can interact electrostatically with the negatively charged ocular surface, which prolongs residence time of the drug. The dosing frequency of Ikervis® is one time per day. This has been associated with improved patient compliance and therapeutic efficiency. A good safety profile of Ikervis® had also been demonstrated in a 12-month multicenter double-blind clinical trial [40]. Cationic emulsions are prone to cause local side effects, such as mild pain at the instillation site [41,42]. To improve eye comfort and bioavailability of the drug, Bang et al. developed self-emulsifying nanodrug delivery systems, namely, Cyporin-N (SNEDDS-N; Taejoon Pharma, Seoul, Republic of Korea) and T-sporin (SNEDDS-T; Taejoon Pharma, Seoul, Republic of Korea). SNEDDS is an anhydrous homogeneous mixture of oils, drugs, surfactants, and cosurfactants. Compared with the high turbidity and unstable pH of Restasis®, SNEDDS exhibits more uniform particle sizes, better light transmission, and more stable pH. The ability of SNEDDS to restore tear film stability is also superior to that of Restasis® [43]. Currently, SNEDDS has been developed in a variety of forms and diseases, such as solid SNEDDS, controlled-release SNEDDS, mucus-permeable SNEDDS, and targeted SNEDDS [44,45,46]. It is hoped that these innovative formulations will lead to a breakthrough in the management of DED. Apart from drug-loaded emulsions, drug-free emulsions have also been developed for DED. For instance, Cationorm® from Santen Pharmaceutical is a drug-free O/W cationic nanoemulsion. The benzylcetyldimethylammonium chloride presented in Cationorm® is a cationic surfactant that possesses intrinsic antimicrobial activity, which makes Cationorm® a preservative-free dosage form. This design enhances the safety of Cationorm®. Pharmacodynamic studies revealed that Cationorm® not only exhibited moisturizing and lubricating properties but also stabilized the tear film by its oily components, thus making it a safe and effective tear supplement [47,48].
2.3. Liposomes
Liposomes are tiny vesicles of 10–1000 nm which are consisted of natural or synthetic phospholipid bilayers. They can be classified as small unilamellar vesicles, large unilamellar vesicles, giant unilamellar vesicles, oligolamellar vesicles, multilamellar large vesicles, and multivesicular vesicles [49]. Film hydration, reverse phase evaporation, solvent injection, detergent removal, and the heating method are conventionally used for the preparation of liposomes. Meanwhile, new technologies such as microfluidic methods and the supercritical fluidic method have gained considerable attention [50]. Liposomes improve the delivery of ophthalmic drugs by encapsulating hydrophobic ones in phospholipid bilayers or encapsulating hydrophilic ones in the aqueous core. With similar structure and composition as the cell membrane, liposomes are generally biodegradable and well-tolerated [51][52][53].
Liposomes are tiny vesicles of 10–1000 nm which are consisted of natural or synthetic phospholipid bilayers. They can be classified as small unilamellar vesicles, large unilamellar vesicles, giant unilamellar vesicles, oligolamellar vesicles, multilamellar large vesicles, and multivesicular vesicles [49]. Film hydration, reverse phase evaporation, solvent injection, detergent removal, and the heating method are conventionally used for the preparation of liposomes. Meanwhile, new technologies such as microfluidic methods and the supercritical fluidic method have gained considerable attention [50]. Liposomes improve the delivery of ophthalmic drugs by encapsulating hydrophobic ones in phospholipid bilayers or encapsulating hydrophilic ones in the aqueous core. With similar structure and composition as the cell membrane, liposomes are generally biodegradable and well-tolerated [51,52,53].
The Tears Again® liposome spray developed by Optima Pharmazeutische (Hallbergmoos, Germany) is a new generation of liposome supplements capable of repairing all three layers of the tear film. The phospholipids in the ingredients repair the lipid layer of the tear film, the isotonic solution replenishes the aqueous layer, and the sodium hyaluronate serves as an alternative to the mucus layer. Upon application, the active ingredients are absorbed transdermally. Meanwhile, the preservatives are blocked outside the skin and do not enter the tear film, thereby preventing damage to the eyes. In a double-blind clinical trial, the Tears Again® liposome spray was found to reduce discomfort and stabilize the tear film more efficiently than saline spray and 0.1% sodium hyaluronate [54][55]. In another example, Chen et al. prepared tacrolimus-loaded cationic liposomes using the film hydration method. The resultant formulation prolongs the retention time of FK506 on the ocular surface, increases its concentration in the cornea, and exerts a good therapeutic effect owing to its anti-inflammatory property and ability to promote epithelial cell healing [56]. Ren T et al. formulated adriamycin ion pair loaded liposomes to improve the therapeutic effects of the drug against DED. First, an adriamycin–cholesterol hemisuccinate ion pair was prepared to improve the drug loading. Second, liposomes were prepared by a film hydration method. Finally, the liposomes were sonicated to obtain uniform particle size with high drug loading efficiency [57]. Recently, the macromolecular protein lactoferrin and the antioxidant astaxanthin have also been encapsulated in liposomes, which showed favorable therapeutic effects against DED as proved by in vivo pharmacodynamics studies [58][59][60].
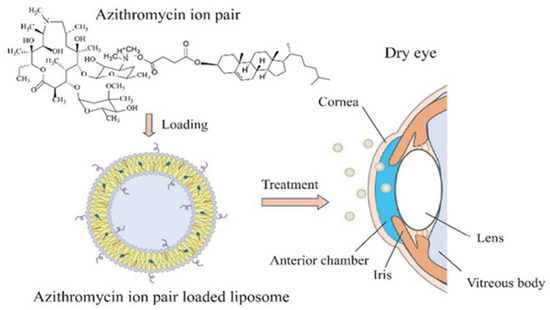
The Tears Again® liposome spray developed by Optima Pharmazeutische (Hallbergmoos, Germany) is a new generation of liposome supplements capable of repairing all three layers of the tear film. The phospholipids in the ingredients repair the lipid layer of the tear film, the isotonic solution replenishes the aqueous layer, and the sodium hyaluronate serves as an alternative to the mucus layer. Upon application, the active ingredients are absorbed transdermally. Meanwhile, the preservatives are blocked outside the skin and do not enter the tear film, thereby preventing damage to the eyes. In a double-blind clinical trial, the Tears Again® liposome spray was found to reduce discomfort and stabilize the tear film more efficiently than saline spray and 0.1% sodium hyaluronate [54,55]. In another example, Chen et al. prepared tacrolimus-loaded cationic liposomes using the film hydration method. The resultant formulation prolongs the retention time of FK506 on the ocular surface, increases its concentration in the cornea, and exerts a good therapeutic effect owing to its anti-inflammatory property and ability to promote epithelial cell healing [56]. Ren T et al. formulated adriamycin ion pair loaded liposomes to improve the therapeutic effects of the drug against DED (Figure 3). First, an adriamycin–cholesterol hemisuccinate ion pair was prepared to improve the drug loading. Second, liposomes were prepared by a film hydration method. Finally, the liposomes were sonicated to obtain uniform particle size with high drug loading efficiency [57]. Recently, the macromolecular protein lactoferrin and the antioxidant astaxanthin have also been encapsulated in liposomes, which showed favorable therapeutic effects against DED as proved by in vivo pharmacodynamics studies [58,59,60].
2.4. Nanoparticles
Figure 3. Schematic illustration for the preparation of adriamycin liposomes. Reprinted with permission from [57]. Copyright 2018 American Chemical Society.
Nanoparticles for drug encapsulation are nanosized delivery vehicles with particle sizes in the range of 1–1000 nm. The majority of them in ophthalmic applications are made from natural or synthetic polymers (gelatin, silk fibroin, chitosan, PLGA, PLA, PCL, etc.). Various methods, such as nanoprecipitation, self-assembly, ionic gelation, and desolvation, have been developed for their preparation. Superior therapeutic effects against ocular diseases are obtained via different mechanisms including increasing the dissolution/solubility of poorly water-soluble drugs, affording sustained release, enhancing ocular retention/penetration, or transporting drugs to targeted tissues/cells [35].
2.4. Nanoparticles
The residence time of eye drops is short due to blink and nasolacrimal duct drainage, which lead to low drug bioavailability. To overcome this drawback, Nagai et al. fabricated a rebamipide-based solid nanoparticle formulation (REB-NPs) via grinding. The thus-obtained rebamipide nanoparticles were elliptical, with particle sizes in the range of 40–200 nm. After being applied to the eyelid, rebamipide can be delivered to the tear film through meibomian glands. The rebamipide nanoparticles prolonged the release duration of rebamipide compared with the conventional rebamipide suspension. Thus, increased mucin levels and tear film restoration were obtained [60]. As the vicious cycle of DED is generally accompanied with a series of changes in the ocular surface microenvironment, nanoparticles with dual or multiple functions are likely to produce synergistic effects and lead to improved therapeutic outcomes. Li YJ et al. developed an AF/Au@Poly-CH nanoparticle formulation with anti-inflammatory and antioxidant functions. AF/Au@Poly-CH was obtained via a one-step self-assembly process. In vivo safety and efficacy studies in rabbit eyes revealed that the resultant nanoformulation was well-tolerated and demonstrated high therapeutic efficacy [62].
Nanoparticles for drug encapsulation are nanosized delivery vehicles with particle sizes in the range of 1–1000 nm. The majority of them in ophthalmic applications are made from natural or synthetic polymers (gelatin, silk fibroin, chitosan, PLGA, PLA, PCL, etc.). Various methods, such as nanoprecipitation, self-assembly, ionic gelation, and desolvation, have been developed for their preparation. Superior therapeutic effects against ocular diseases are obtained via different mechanisms including increasing the dissolution/solubility of poorly water-soluble drugs, affording sustained release, enhancing ocular retention/penetration, or transporting drugs to targeted tissues/cells [35].
Drug-loaded nanoparticles have also been formulated into dosage forms other than eye drops. For example, Ryu et al. developed nanoparticles incorporated tablets, by embedding PLGA nanoparticles containing dexamethasone in an alginate matrix. The table was applied to the ocular surface using a preocular applicator. It was found that the nanoparticles remained on the ocular surface for up to 2 h. This mode of administration not only improves the bioavailability of drugs but also enables their sterile delivery [63][64]. Nanocapsules are nanoparticles with hollow cores, which are mainly used to deliver labile drugs or engineered for targeted delivery. Although several nanocapsule-based delivery systems exist for anti-inflammatory drugs, few reports are available with respect to their application for the treatment of DED [65][66]. Zhang et al. prepared cyclosporine lipid nanocapsule eye drops with the phase-inversion method, which increased bioavailabilities of cyclosporine in the conjunctiva and cornea. In line with the pharmacokinetic study, superior therapeutic effects over conventional cyclosporine emulsion were observed in pharmacodynamic studies [67].
3. Conclusions
Other drug delivery systems, such as microspheres, hydrogels, and bioadhesive polymers have also been engineered to improve therapeutic effects of DED drugs. Indeed, promising results are obtained, which have the potential to lead to innovative therapies. Considering the shortcomings of each drug delivery system, the combination of two or more of them deserves further research. Current treatments for DED generally target one aspect of DED pathophysiology. It is fascinating to explore whether superior outcomes can be obtained with drug delivery systems that target multiple aspects simultaneously. There is also a lack of biodegradability and in vivo safety information concerning the above-mentioned drug delivery systems, as most studies are conducted in the short-term setting. A direct comparison between these delivery vehicles represents another issue to be addressed to determine the most suitable one. Finding answers to these questions constitutes the key areas of future research to improve drug delivery for DED.
The residence time of eye drops is short due to blink and nasolacrimal duct drainage, which lead to low drug bioavailability. To overcome this drawback, Nagai et al. fabricated a rebamipide-based solid nanoparticle formulation (REB-NPs) via grinding. The thus-obtained rebamipide nanoparticles were elliptical, with particle sizes in the range of 40–200 nm. After being applied to the eyelid, rebamipide can be delivered to the tear film through meibomian glands. The rebamipide nanoparticles prolonged the release duration of rebamipide compared with the conventional rebamipide suspension. Thus, increased mucin levels and tear film restoration were obtained [61]. As the vicious cycle of DED is generally accompanied with a series of changes in the ocular surface microenvironment, nanoparticles with dual or multiple functions are likely to produce synergistic effects and lead to improved therapeutic outcomes. Li YJ et al. developed an AF/Au@Poly-CH nanoparticle formulation with anti-inflammatory and antioxidant functions. AF/Au@Poly-CH was obtained via a one-step self-assembly process. In vivo safety and efficacy studies in rabbit eyes revealed that the resultant nanoformulation was well-tolerated and demonstrated high therapeutic efficacy [62].