Polymorphism (rs1805086), c.458A>G, p.Lys(K)153Arg(R), (K153R) of the myostatin gene (MSTN) has been associated with a skeletal muscle phenotype (hypertrophic response in muscles due to strength training). The K153R polymorphism is significant in the development of muscle mass and strength. The rare R variant increases the inhibition of MSTN synthesis, thereby leading to an increase in skeletal muscle mass and muscle strength. The R variant is favorable for sports in which muscle strength and mass are important, such as bodybuilding, powerlifting, weightlifting, arm wrestling, kettlebell lifting, shot put, and bobsleigh. It can be assumed that the strong effect of this allele on the ability to become a successful athlete in weightlifting and speed-power sports is based on the inhibition of MSTN synthesis.
- myostatin
- MSTN
- muscle
- strength
1. History
1.1. MSTN Inhibitors
There are a number of factors that act as inhibitors of MSTN synthesis, including the myocyte 2 enhancing factor (MEF2); γ-receptors activated by peroxisome proliferator (PPARγ); MyoD; and hormones, such as insulin-like growth factor (IGF-1), angiotensin II, thyroid hormone, erythropoietin [17][22], sex steroids, follistatin, and estradiol [18][23]. One of the main factors in sports that significantly affects the level of MSTN secreted is power-oriented physical activity, hypoxia, and dietary supplements. Moreover, the production of MSTN is influenced by essential amino acids, which are often consumed by athletes after intensive training [19][24]. Currently, the study of antibodies against MSTN, e.g., MYO—029 and BYM338, are attracting much attention, but their effectiveness is still poorly studied [20][21][25,26]. In addition to antibodies, other MSTN inhibitors, such as hormone follistatin, can also suppress its activity [22][23][24][27,28,29]. Recent studies have shown that essential amino acids suppress MSTN expression in human skeletal muscles [25][26][30,31]. In high-performance sports, MSTN inhibition is prohibited by WADA (https://www.wada-ama.org/en/resources/world-anti-doping-program/2023-prohibited-list, accessed on 15 October 2022; page 11 class S4). MSTN is a potential genetic marker of the athletic abilities in strength sports because of the involvement of a large number of skeletal muscles and the functions of myokines. Some research related to the study of MSTN and its role in hypertrophy and skeletal muscle strength seemed contradictory [27][28][29][20,32,33].1.2. Mechanism of Effect of
MSTN
on Skeletal Muscle Mass and Strength
Physical activity causes muscle hypertrophy and performing physical power-oriented exercises clearly demonstrated this. This type of exercise causes mechanical damage to sarcomeres and sarcolemmas. After a certain period of time, the balance shifts toward protein synthesis and, as a result, phenotypic changes increase the volume and strength of skeletal muscles. These processes release active MSTN, which affects satellite cells and fibroblasts located near the damaged area. MSTN can cause protein degradation in myofibrils, which are important for the normal functioning of muscle fibers as they remove unnecessary, wasted proteins from the muscle cells [30][34]. MSTN is one of the main factors associated with muscle atrophy. In studies involving humans, it was found that by the 25th day of the sedentary regime, the level of MSTN increased by 12% [9]. MSTN can regulate the function of muscle fibers and nearby cells, which include fibroblasts and satellite cells or satellites. Mature muscle fibers are the products of final differentiation [23][28]. An increase in muscle size is achieved by the fusion of satellite-proliferating cells with fibers. Primarily, microtrauma in a single muscle fiber acts as a stimulus for the proliferation of satellite cells in adult organisms. When these cells are activated and emerge from a dormant state, genes characteristic of myoblasts are also activated. Therefore, satellite cells become myoblasts that migrate to the damaged areas of muscle tissue and depending on the degree of damage, either merge with the damaged muscle fiber (hypertrophy) or merge with each other, thus creating new fibers (hyperplasia). Therefore, satellite cells regulate the functional state of skeletal muscles in the adult body (Figure 12). They are necessary for the restoration of damaged muscle fibers and are a source of additional nuclei in case of muscle hypertrophy after training sessions. MSTN negatively affects the proliferation of satellite cells [31][35]. Power-oriented training sessions result in mechanical stretching of the muscle and lead to microdamage. There is also evidence that MSTN negatively regulates the activation of resting satellite cells, hindering their development. Such inhibitory effects are necessary for normal muscle regeneration as a premature fusion of satellite cells with myofibrils can impair muscle fiber functions.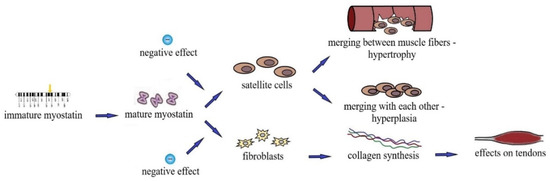
1.3. Effect of MSTN on Tendons and Bones
Tendons are an important component in the manifestation of the maximum strength of the skeletal muscle. Weightlifting and speed-strength sports athletes with high indicators of skeletal muscle strength often have tendon injuries as their muscle strength exceeds their endurance. During strength training, fibroblasts proliferate, collagen synthesis increases and the cross-sectional area of the tendons increases to make them stiffer. This allows the tendons to withstand high-intensity physical loads and reduce the risk of damage to them [35][39]. MSTN can change the mechanical properties of tendons by impairing their ability to stretch, increasing the risk of damage. Such data cast doubt on the feasibility of inhibiting MSTN expression for sports purposes [31][35]. The exact mechanisms of the effect of MSTN on tendons and ligaments are still unknown, and further studies are needed to assess its regulatory role in these processes [36][40]. When studying the regeneration of muscles and tendon fibroblasts, it is assumed that MSTN affects the expression of type 1 collagen. Recent studies have reported that local injections of exogenous MSTN during tendon healing increase the cross-sectional area of the tendon [37][41]. In both human and animal studies, there is evidence that MSTN is an important regulator of muscle mass as well as bone density. The mechanisms by which MSTN regulates bone formation are not completely understood, but it is clear that it has a direct effect on the proliferation and differentiation of stem cells [38][39][42,43]. Since MSTN and its receptor are expressed during bone regeneration, it affects bone density [39][43]. It is likely that MSTN directly affects bones, increasing bone mineral density. Some features of different phenotypes may be associated with increased biomechanical load, e.g., in weightlifters or under the influence of other factors, such as mechanical growth factors or growth hormones. These issues have yet to be studied in more detail, but if a number of studies prove that MSTN does have an effect on bones, then it can be assumed that MSTN inhibitors will be useful not only for increasing muscle mass but also for bone density. This assumption is supported by recent data showing that MSTN significantly increases bone volume during fibular healing [40][44].2. Myostatin Mutations
2.1.
MSTN
Mutation (rs397515373,
c.373 + 5 G>A
)
This mutation is very rare, with an average prevalence of 0.0004% in the population. It was necessary to obtain 500,000 samples to detect a mutation once. In 2004, a paper describing a case of MSTN mutation in a child was published. In both the allelic copies of MSTN, the newborn boy had mutations that suppressed the synthesis of the functioning MSTN protein. The child was observed to have enlarged muscles of the thighs and upper extremities at birth. Ultrasonography of this child showed that the cross-section of the quadriceps femoris muscle was 7.2 SD, which was higher than the average (± standard deviation) value for 10 persons matched for age and gender. Moreover, the thickness of his subcutaneous fat was 2.88 SD below the average value of that of his peers. All reflexes of the child were normal, except for those associated with tendons. Interestingly, this mutation was also present in other members of this family. One of the relatives was extraordinarily strong, and the 24-year-old mother of the child was a professional athlete and had developed muscles, although to a lesser extent than her son. It showed for the first time that the MSTN rs397515373 mutation (c.373 + 5 G>A) leads to an increase in muscle mass and strength [41][49].2.2.
MSTN A55T
Mutation (rs180565, 163
G>A
)
A55T is important for the stability of the inhibitory activity of MSTN and affects the mature MSTN [42][50]. A study devoted to physical exercise reported that after 8 weeks of exercise with weights the subjects with A55T polymorphism AT and TT genotypes had greater muscle hypertrophy than those with AA genotype [43][51]. Studies have shown that MSTN polymorphisms can affect the skeletal muscle phenotype after exercise with weights. However, previous studies of MSTN SNPs associated with muscle hypertrophy in response to prolonged power-oriented strength exercises have not confirmed pronounced muscle hypertrophy after strength physical load [44][52]. Chinese scientists found that people with the MSTN A55T AT + TT genotype showed a significant increase in the thickness of biceps (0.292 ± 0.210 cm, P = 0.03) but not of quadriceps (0.254 ± 0.198 cm, P = 0.07) compared to those of AA genotype carriers. Thus, the obtained results suggest a possible association between A55T polymorphism and muscle hypertrophy caused by strength training in Chinese individuals [43][51]. Korean researchers have found that the A55T polymorphism is associated with skeletal muscle recovery after strength training. The study sample included 48 young, healthy college students (age 24.8 ± 2.2 years, height 176.7 ± 5.3 cm, weight 73.7 ± 8.3 kg) who performed 50 repetitions in strength exercises. After strength exercises subjects with heterozygous AT showed significantly faster muscle recovery than those in the AA group (P = 0.042). These results prove that the A55T polymorphism AT genotype is associated with a faster recovery of skeletal muscle strength after intense strength exercise [45][54].2.3. Mutation of
MSTN E164K
rs35781413 (
c.490G>A, p.Glu164Lus
)
In a number of studies related to the influence of this genotype on the phenotype of athletes and people not engaged in sports, the results of experiments showed no statistically significant differences [46][58]. According to the website http://www.ensembl.org (accessed on 15 October 2022), the average frequency of a rare allele was 1%. There are only indirect assumptions that this mutation can affect the manifestation of muscle mass and strength in humans. These assumptions are based on the fact that this polymorphism can make a significant contribution to the biochemical variability of mature MSTN, and accordingly, affect the state of the vertebrate muscular system.2.4. Mutation of
MSTN K153R
(rs1805086,
p.Lys153Arg, c.458A>G
)
The MSTN rs1805086 RR genotype gene is more common in top-class weightlifting athletes [47][59]. Some researchers found a positive association between the K153R rs1805086 polymorphisms and the manifestation of strength abilities and muscle hypertrophy [13][43][48][49][13,46,51,60], whereas other researchers did not find any significant connection [29][48][50][33,46,61]. Some studies have proven a connection with high performance in high jumps (P < 0.05) [48][46]. Studies on the relationship between K153R and skeletal muscle phenotypes in elderly Caucasian women have shown that the heterozygote MSTN rs1805086 KR is a favorable polymorphism for the increased muscle mass in the biceps of the shoulder [51][62].2.5.
MSTN K153R
(rs1805086) Polymorphism Frequency
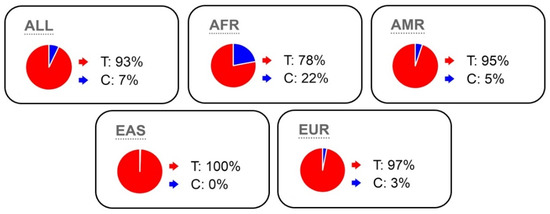
According to the Ensembl database, the frequency of the rare variant K153R is on an average 7% (3% in Caucasians and 22% in Africans), and large sample sizes are necessary to reliably identify the association of this polymorphism with strength abilities and muscle hypertrophy (Figure 23).