Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Camila Xu and Version 1 by Miricescu Daniela.
Hypertension is defined as repeated elevated office systolic blood pressure (SBP) values over 140 mmHg and/or diastolic BP (DBP) over 90 mmHg or average home BP over 135/85 mmHg. Metabolic syndrome (MetS) has serious outcomes regarding the individual’s health, with increasing prevalence nowadays and a significant impact on healthcare systems. Its definition varied over time. MetS consists of several conditions, such as hypertension, elevated fasting glucose (over 100 mg/dL) or type 2 diabetes mellitus (T2DM), decreased high-density lipoprotein cholesterol levels (less than 40 mg/dL in men or 50 mg/dL in women), high triglycerides concentrations (over 150 mg/dL) and waist circumference over 40 inches (men) or 35 inches (women).
- hypertension
- metabolic syndrome
- type 2 diabetes mellitus
1. Introduction
Hypertension, which possesses a significant prevalence in the general population, is one of the main constituents of metabolic syndrome. Hypertension is strongly associated with metabolic syndrome through the pathophysiology which involves obesity. Nevertheless, it represents the major risk factor responsible for elevating cardiovascular mortality and morbidity [1].
Hypertension is defined as repeated elevated office systolic blood pressure (SBP) values over 140 mmHg and/or diastolic BP (DBP) over 90 mmHg or average home BP over 135/85 mmHg [2,3][2][3].
Metabolic syndrome (MetS) has serious outcomes regarding the individual’s health, with increasing prevalence nowadays and a significant impact on healthcare systems. Its definition varied over time. MetS consists of several conditions, such as hypertension, elevated fasting glucose (over 100 mg/dL) or type 2 diabetes mellitus (T2DM), decreased high-density lipoprotein cholesterol levels (less than 40 mg/dL in men or 50 mg/dL in women), high triglycerides concentrations (over 150 mg/dL) and waist circumference over 40 inches (men) or 35 inches (women) [4].
MetS amplifies the risk for insulin resistance, cardiovascular and neurological complications [5]. The pathogenesis of MetS consists of multiple genetic and acquired mechanisms related to insulin resistance and chronic inflammation [6]. The burden of MetS is to be considered since it leads to adverse cardiovascular outcomes, which stand for the number one mortality cause worldwide [6].
Reaven, in 1988, discussed “syndrome X” as a metabolic syndrome represented by glucose intolerance, insulin resistance, dyslipidemia, hypertension and coronary artery disease [7]. However, earlier in 1973, the term “syndrome X” was first introduced by Kemp [8], representing symptoms of myocardial ischemia and electrocardiographic stress changes, but in the absence of atherosclerotic plaques of the coronary arteries [9].
Therefore, to distinguish between these two entities, Reaven’s “syndrome X” was associated with the term “metabolic” [8,9][8][9]. As we know, MetS includes central obesity, hypertension, insulin resistance and dyslipidemia. It is associated with an increased risk of developing complications such as diabetes and atherosclerotic cardiovascular disease [10]. Diabetes mellitus is a chronic metabolic disorder characterized by persistent high blood sugar levels [11]. It is classified into three types by etiology and clinical presentation, but type 2 diabetes accounts for around 90% of all cases [12]. Type 2 diabetes mellitus (T2DM) is an important problem that affects the entire planet and is constantly growing. In developed countries, diabetes is the main cause of cardiovascular diseases [12]. T2DM is characterized by insulin resistance that leads to insulin ineffectiveness. Initially, insulin production is increased to maintain glucose homeostasis, but over time it decreases Although people older than 45 years are most frequently affected, it is more and more common among young people due to multiple factors such as junk food, a sedentary lifestyle, and obesity [12]. Dysglycemia is a term used to describe impaired glucose regulation (or prediabetes) and diabetes mellitus [13]. A recent meta-analysis showed an inverse association between metabolic syndrome and intake of n-3 polyunsaturated fatty acids [14], which might explain why the increased intake of red meat decreases the incidence of dysglycemia [14]. Inadequate glucose metabolism (diabetes mellitus, impaired glucose tolerance, insulin resistance) or dyslipidemia are frequently associated with arterial hypertension [15,16,17][15][16][17]. In conclusion, hypertension is one of the most frequently diagnosed cardiovascular conditions, with well-known metabolic complications (hyperglycemia, diabetes mellitus, hyperlipidemia).
2. Pathogenesis of Hypertension in MetS
There are multiple mechanisms involved in the pathogenesis of MetS. Lifestyle, environmental, genetic, but also epigenetic [18] factors contribute to the development of MetS [6].
Insulin resistance can be found in most patients with impaired glucose tolerance or non-insulin dependent diabetes mellitus, but also in about a quarter of individuals with adequate weight and normal glucose tolerance [7]. Therefore, in these cases, the compensatory mechanism to keep glucose levels in optimal parameters is to increase insulin secretion in pancreatic cells, resulting in hyperinsulinemia [7].
Free fatty acids (FFA) play a role in the connection between insulin resistance, insulin levels and glucose tolerance. Plasma FFA can be lowered as a result of higher insulin concentrations. For that reason, hyperinsulinemia counteracts high FFA levels. When disruptions in these processes appear and hyperinsulinemia cannot be sustained, high FFA concentrations will amplify hepatic glucose production. Even slight elevations of hepatic glucose production can result in remarkable hyperglycemia [7].
There is a connection between hypertension, insulin resistance, hyperglycemia, and hyperinsulinemia [19,20,21,22,23,24,25,26,27][19][20][21][22][23][24][25][26][27]. Hyperinsulinemia is associated with elevated concentrations of plasmatic catecholamines, irrespective of plasmatic glucose levels [28,29][28][29]. Hypertension can also result from sodium and water metabolism through proximal renal tubular reabsorption, favoured by insulin [30].
Experimental studies indicated that hypertension could be induced in animal subjects while feeding them with food rich in fructose [7]. Due to accentuated sympathetic activity, hypertension can also be noted in sucrose-fed mice [31,32][31][32]. They conclude that blood pressure can increase as a response to dietary changes, leading to insulin resistance and hyperinsulinemia [7].
Resistance to insulin-stimulated glucose uptake is linked to hyperinsulinemia, glucose intolerance, hypertension, low HDL-cholesterol, and high triglycerides levels while also being able to influence coronary artery disease [7].
MetS is represented by a relationship between epigenetic, genetic, and environmental factors. The last two mentioned factors can lead to different expressions of orphan G protein-coupled receptors (GPCR) in MetS, such as GPR21 and GPR 82, raising the suspicion that they can represent a possible future therapeutic target gut metabolic syndrome [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33].
MicroRNA (miRNA) are small ribonucleotide acids, which regulate gene expression at the post-transcriptional level by connecting to the 3′UTRs region of messenger RNA, being able to promote or suppress translation [34]. It was observed that suppression of miR-33a can ameliorate the functional status of MetS patients since its activity consists of favoring atherosclerosis and regulation of glucose and cholesterol metabolism. Insulin resistance, statin use, and therefore low cholesterol levels can induce SREBP 1 and 2 genes, with the overexpression of miR-33a and miR-33b. This leads to low fatty acid beta-oxidation, decreased insulin signaling and low HDL-cholesterol levels, thus raising the risk for MetS [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35]. miR-221 and let-7 were found in high concentrations in females with MetS. Let-7 was correlated with hypertension and HDL-cholesterol levels [36].
Insulin resistance leads to hypertension through the loss of the vasodilatory effect of insulin and amplification of vasoconstriction due to FFA through reactive oxygen species [6,7,8,9,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37][6][7][8][9][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37].
Metabolomics also plays a role in the pathogenesis of MetS. Choline, L-carnitine, and trimethylamine-N-oxide are associated with insulin resistance and unfavorable cardiometabolic events [6,38,39,40,41][6][38][39][40][41]. Alanine, glutamine, aspartate, asparagine, arginine, histidine methionine, cysteine, and lysine play a role in the evolution of insulin resistance [42]. Early markers for the possible occurrence of MetS can be phenylalanine, tryptophan, tyrosine, and phospholipids [43,44,45][43][44][45].
3. Links between Hypertension and Metabolic Syndrome
As we know, hypertension is an important element in MetS. The connections between these two entities are multiple, and complicated and they are not fully known until now.
Links that exist between hypertension and MetS include insulin resistance, central/visceral obesity, sympathetic overactivity, activated renin-angiotensin system, oxidative stress, increased inflammatory mediators, and obstructive sleep apnea [46]. In the following lines, we will discuss each separately to see how hypertension occurs in MetS will be discussed.
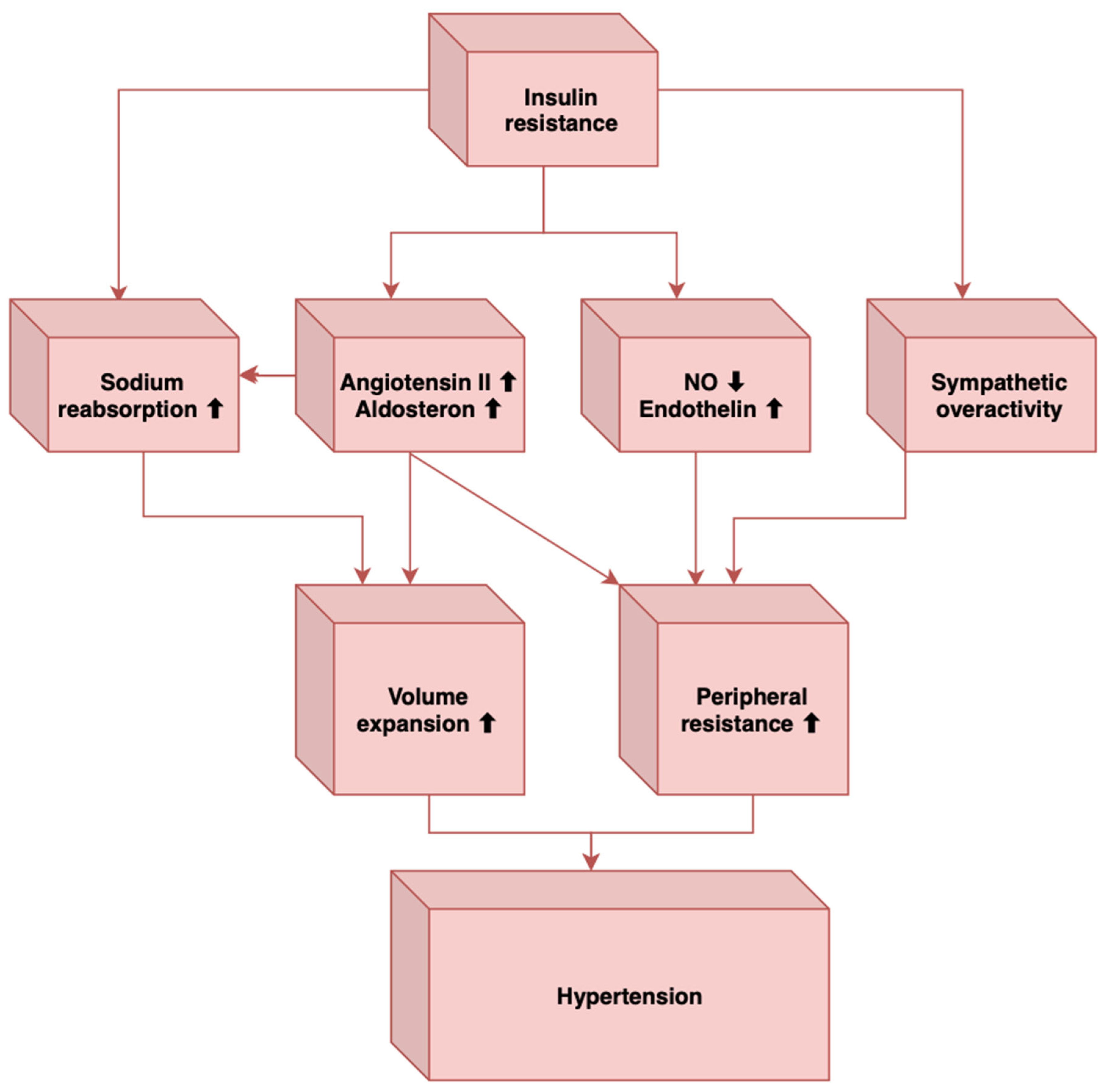
MetS has insulin resistance as its main constituent. Studies have shown that insulin has an anti-natriuretic effect by stimulating sodium reabsorption, an effect that is not only preserved in insulin resistance but can even be increased [46]. Therefore, this can lead to hypertension within the metabolic syndrome. Likewise, other mechanisms by which insulin resistance contributes to the appearance of elevated blood pressure in the metabolic syndrome are the loss of the vasodilator effect of insulin, vasoconstriction caused by free fatty acids, and sympathetic hyperactivation [47].
Another thing worth mentioning about the link between insulin resistance and hypertension is the observation that drugs that improve insulin resistance and reduce hyperinsulinemia (such as metformin and sensitisers glitazones) also control hypertension very well. At the same time, some antihypertensives, such as angiotensin II converting enzyme inhibitors or angiotensin II receptor antagonists, also increase insulin sensitivity [48].
The second link is visceral or central obesity. Studies have shown that adipose tissue is an endocrine organ that secretes adipocytokines such as leptin, tumour necrosis factor-α (TNF-α), interleukin-6 (IL-6), angiotensinogen, and non-esterified fatty acids (NEFA), bioactive substances that have multiple roles in the body. An important effect of adipocytokines is the production of arterial hypertension. In addition, visceral obesity is the leading cause of MetS, which is why we can establish a li link between it and hypertension [46] can be established [46].
Regarding sympathetic overactivity, the level of serum catecholamines and the activity of the sympathetic nervous system are increased in obese patients, especially for those with central obesity. People with obesity have an active renin-angiotensin system and a positive feedback relationship with the sympathetic nervous system, contributing to high blood pressure [38]. The plasma level of leptin is increased by insulin resistance, and leptin positively influences the activity of the nervous system, which leads us to think of hypertension associated with obesity [49].
There is a connection between endothelial dysfunction, which contributes to the appearance of high blood pressure, and insulin resistance, a fact highlighted by some epidemiological studies [38]. A prospective cohort study demonstrated that endothelial vasomotor dysfunction precedes and predicts the development of hypertension [50].
Another element involved in the occurrence of elevated blood pressure is the increase of inflammatory mediators [46]. Among the mediators involved in the pathophysiology of arterial hypertension within the MetS are tumour necrosis factor-α (TNF-α) and interleukin-6 (IL-6). The serum level of TNF-α was correlated with insulin resistance and systolic blood pressure. At the same time, IL-6 stimulates the sympathetic nervous system and induces an increase in the plasmatic level of angiotensinogen and angiotensin II, causing an increase in blood pressure [46].
Sympathetic overactivity has also been associated with obstructive sleep apnea [46], another important element that can contribute to hypertension, and individuals with obstructive sleep apnea have a high prevalence of MetS [49]. In MetS, there is a sympathetic activation induced by the baroreflex dysfunction, which also characterizes obstructive sleep apnea [46]. How obstructive sleep apnea leads to sympathetic stimulation is the stimulation of arterial chemoreceptors through nocturnal hypoxia and hypercapnia [46]. Other mechanisms through which obstructive sleep apnea contributes to elevated blood pressure levels are insulin resistance, endothelial dysfunction, elevated angiotensin II and aldosterone levels, oxidative stress, hyperleptinemia, and inflammation [51,52][51][52]. In conclusion, these factors may induce vasoconstriction, decreased vasodilatation, sympathetic overactivity, and increased intravascular fluid, leading to the development of hypertension in MetS (Figure 1).
References
- Franklin, S.S. Hypertension in the Metabolic Syndrome. Metab. Syndr. Relat. Disord. 2006, 4, 287–298.
- Bergler-Klein, J. What’s New in the ESC 2018 Guidelines for Arterial Hypertension: The Ten Most Important Messages. Wien. Klin. Wochenschr. 2019, 131, 180–185.
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104.
- Swarup, S.; Goyal, A.; Grigorova, Y.; Zeltser, R. Metabolic Syndrome; StatPearls: Treasure Island, FL, USA, 2022.
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int. J. Sports Med. 2021, 42, 199–214.
- Fahed, C.; Aoun, L.; Zerdan, M.B.; Allam, S.; Zerdan, M.B.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786.
- Reaven, G.M. Banting Lecture 1988. Role of Insulin Resistance in Human Disease. Diabetes 1988, 37, 1595–1607.
- Kemp, H.G. Left Ventricular Function in Patients with the Anginal Syndrome and Normal Coronary Arteriograms. Am. J. Cardiol. 1973, 32, 375–376.
- Cheng, T.O. Cardiac Syndrome X versus Metabolic Syndrome X. Int. J. Cardiol. 2007, 119, 137–138.
- Rochlani, Y.; Pothineni, N.V.; Kovelamudi, S.; Mehta, J.L. Metabolic syndrome: Pathophysiology, management, and modulation by natural compounds. Ther. Adv. Cardiovasc. Dis. 2017, 11, 215–225.
- NCBI. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513253 (accessed on 21 December 2022).
- Regufe, V.M.G.; Pinto, C.M.C.B.; Perez, P.M.V.H.C. Metabolic syndrome in type 2 diabetic patients: A review of current evidence. Porto Biomed. J. 2020, 5, e101.
- Jambi, H.; Enani, S.; Malibary, M.; Bahijri, S.; Eldakhakhny, B.; Al-Ahmadi, J.; Al Raddadi, R.; Ajabnoor, G.; Boraie, A.; Tuomilehto, J. The Association Between Dietary Habits and Other Lifestyle Indicators and Dysglycemia in Saudi Adults Free of Previous Diagnosis of Diabetes. Nutr. Metab. Insights 2020, 15, 1178638820965258.
- Jang, H.; Park, K. Omega-3 and omega-6 polyunsaturated fatty acids and metabolic syndrome: A systemic review and meta-analysis. Clin. Nutr. 2020, 39, 765–773.
- Onat, A.; Hergenc, G.; Sari, I.; Turkmen, S.; Can, G.; Sansoy, V. Dyslipidemic hypertension: Distinctive features and cardiovascular risk in a prospective population-based study. Am. J. Hypertens. 2005, 18, 409–416.
- Garcia-Puig, J.; Ruilope, L.M.; Luque, M.; Fernandez, J.; Ortega, R.; Dal-Re, R. Glucose metabolism in patients with essential hypertension. Am. J. Med. 2006, 119, 318–326.
- Chen, W.; Li, F.; He, C.; Zhu, Y.; Tan, W. Elevated prevalence of abdominal glucose metabolism in patients with primary aldosteronism: A meta-analysis. Ir. J. Med. Sci. 2014, 183, 283–291.
- Fathi Dizaji, B. The Investigations of Genetic Determinants of the Metabolic Syndrome. Diabetes Metab. Syndr. 2018, 12, 783–789.
- Stamler, J.; Rhomberg, P.; Schoenberger, J.A.; Shekelle, R.B.; Dyer, A.; Shekelle, S.; Stamler, R.; Wannamaker, J. Multivariate Analysis of the Relationship of Seven Variables to Blood Pressure: Findings of the Chicago Heart Association Detection Project in Industry, 1967–1972. J. Chronic. Dis. 1975, 28, 527–548.
- Florey, C.V.; Uppal, S.; Lowy, C. Relation between Blood Pressure, Weight, and Plasma Sugar and Serum Insulin Levels in Schoolchildren Aged 9–12 Years in Westland, Holland. Br. Med. J. 1976, 1, 1368–1371.
- Jarrett, R.J.; Keen, H.; Mccartney, M.; Fuller, J.H.; Hamilton, P.J.S.; Reid, D.D.; Rose, G. Glucose Tolerance and Blood Pressure in Two Population Samples: Their Relation to Diabetes Mellitus and Hypertension. Int. J. Epidemiol. 1978, 7, 15–24.
- Persky, V.; Dyer, A.; Stamler, J.; Shekelle, R.B.; Schoenberger, J.; Wannamaker, J.; Upton, M. The Relationship between Post-Load Plasma Glucose and Blood Pressure at Different Resting Heart Rates. J. Chronic. Dis. 1979, 32, 263–268.
- Voors, A.W.; Radhakrishnamurthy, B.; Srinivasan, S.R.; Webber, L.S.; Berenson, G.S. Plasma Glucose Level Related to Blood Pressure in 272 Children, Ages 7-15 Years, Sampled from a Total Biracial Population. Am. J. Epidemiol. 1981, 113, 347–356.
- Lucas, C.P.; Estigarribia, J.A.; Darga, L.L.; Reaven, G.M. Insulin and Blood Pressure in Obesity. Hypertension 1985, 7, 702–706.
- Singer, P.; Gödicke, W.; Voigt, S.; Hajdu, I.; Weiss, M. Postprandial Hyperinsulinemia in Patients with Mild Essential Hypertension. Hypertension 1985, 7, 182–186.
- Modan, M.; Halkin, H.; Almog, S.; Lusky, A.; Eshkol, A.; Shefi, M.; Shitrit, A.; Fuchs, Z. Hyperinsulinemia. A Link between Hypertension Obesity and Glucose Intolerance. J. Clin. Investig. 1985, 75, 809–817.
- Manicardi, V.; Camellini, L.; Bellodi, G.; Coscelli, C.; Ferrannini, E. Evidence for an Association of High Blood Pressure and Hyperinsulinemia in Obese Man. J. Clin. Endocrinol. Metab. 1986, 62, 1302–1304.
- Rowe, J.W.; Young, J.B.; Minaker, K.L.; Stevens, A.L.; Pallotta, J.; Landsberg, L. Effect of Insulin and Glucose Infusions on Sympathetic Nervous System Activity in Normal Man. Diabetes 1981, 30, 219–225.
- Christensen, N.J.; Gundersen, H.J.G.; Hegedüs, L.; Jacobsen, F.; Mogensen, C.E.; Østerby, R.; Vittinghus, E. Acute Effects of Insulin on Plasma Noradrenaline and the Cardiovascular System. Metabolism 1980, 29 (Suppl. 1), 1138–1145.
- Baum, M. Insulin Stimulates Volume Absorption in the Rabbit Proximal Convoluted Tubule. J. Clin. Investig. 1987, 79, 1104–1109.
- Landsberg, L.; Young, J.B. Diet and the Sympathetic Nervous System: Relationship to Hypertension. Int. J. Obes. 1981, 5, 79–91.
- Hwang, I.S.; Ho, H.; Hoffman, B.B.; Reaven, G.M. Fructose-Induced Insulin Resistance and Hypertension in Rats. Hypertension 1987, 10, 512–516.
- Romero-Nava, R.; García, N.; Aguayo-Cerón, K.A.; Sánchez Muñoz, F.; Huang, F.; Hong, E.; Villafaña, S. Modifications in GPR21 and GPR82 Genes Expression as a Consequence of Metabolic Syndrome Etiology. J. Recept. Signal Transduct. Res. 2021, 41, 38–44.
- Ionescu, R.F.; Enache, R.M.; Cretoiu, S.M.; Cretoiu, D. The Interplay Between Gut Microbiota and MiRNAs in Cardiovascular Diseases. Front. Cardiovasc. Med. 2022, 9, 856901.
- Gharipour, M.; Sadeghi, M. Pivotal Role of MicroRNA-33 in Metabolic Syndrome: A Systematic Review. ARYA Atheroscler. 2013, 9, 372.
- Wang, Y.T.; Tsai, P.C.; Liao, Y.C.; Hsu, C.Y.; Juo, S.H.H. Circulating MicroRNAs Have a Sex-Specific Association with Metabolic Syndrome. J. Biomed. Sci. 2013, 20, 72.
- Tripathy, D.; Mohanty, P.; Dhindsa, S.; Syed, T.; Ghanim, H.; Aliada, A.; Dandona, P. Elevation of Free Fatty Acids Induces Inflammation and Impairs Vascular Reactivity in Healthy Subjects. Diabetes 2003, 52, 2882–2887.
- Lent-Schochet, D.; McLaughlin, M.; Ramakrishnan, N.; Jialal, I. Exploratory Metabolomics of Metabolic Syndrome: A Status Report. World J. Diabetes 2019, 10, 23–36.
- Yamada, J.; Tomiyama, H.; Yambe, M.; Koji, Y.; Motobe, K.; Shiina, K.; Yamamoto, Y.; Yamashina, A. Elevated Serum Levels of Alanine Aminotransferase and Gamma Glutamyltransferase Are Markers of Inflammation and Oxidative Stress Independent of the Metabolic Syndrome. Atherosclerosis 2006, 189, 198–205.
- Velasquez, M.T.; Ramezani, A.; Manal, A.; Raj, D.S. Trimethylamine N-Oxide: The Good, the Bad and the Unknown. Toxins 2016, 8, 326.
- Tang, W.H.W.; Hazen, S.L. Microbiome, Trimethylamine N-Oxide, and Cardiometabolic Disease. Transl. Res. 2017, 179, 108–115.
- Hart, L.M.T.; Vogelzangs, N.; Mook-Kanamori, D.O.; Brahimaj, A.; Nano, J.; van der Heijden, A.A.W.A.; van Dijk, K.W.; Slieker, R.C.; Steyerberg, E.W.; Ikram, A.; et al. Blood Metabolomic Measures Associate With Present and Future Glycemic Control in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2018, 103, 4569–4579.
- Adams, S.H. Emerging Perspectives on Essential Amino Acid Metabolism in Obesity and the Insulin-Resistant State. Adv. Nutr. 2011, 2, 445–456.
- Chen, T.; Zheng, X.; Ma, X.; Bao, Y.; Ni, Y.; Hu, C.; Rajani, C.; Huang, F.; Zhao, A.; Jiia, W.; et al. Tryptophan Predicts the Risk for Future Type 2 Diabetes. PLoS ONE 2016, 11, e0162192.
- Oxenkrug, G.; van der Hart, M.; Summergrad, P. Elevated Anthranilic Acid Plasma Concentrations in Type 1 but Not Type 2 Diabetes Mellitus. Integr. Mol. Med. 2015, 2, 365–368.
- Yanai, H.; Tomono, Y.; Ito, K.; Furutani, N.; Yoshida, H.; Tada, N. The Underlying Mechanisms for Development of Hypertension in the Metabolic Syndrome. Nutr. J. 2008, 7, 10.
- Manrique, C.; Lastra, G.; Sowers, J.R. New Insights into Insulin Action and Resistance in the Vasculature. Ann. N. Y. Acad. Sci. 2014, 1311, 138–150.
- Mendizábal, Y.; Llorens, S.; Nava, E. Hypertension in Metabolic Syndrome: Vascular Pathophysiology. Int. J. Hypertens. 2013, 2013, 230868.
- Alvarez, G.E.; Beske, S.D.; Ballard, T.P.; Davy, K.P. Sympathetic Neural Activation in Visceral Obesity. Circulation 2002, 106, 2533–2536.
- de Jongh, R.T.; Serné, E.H.; Ijzerman, R.G.; de Vries, G.; Stehouwer, C.D.A. Impaired Microvascular Function in Obesity: Implications for Obesity-Associated Microangiopathy, Hypertension, and Insulin Resistance. Circulation 2004, 109, 2529–2535.
- Kirpichnikov, D.; Sowers, J.R. Diabetes Mellitus and Diabetes-Associated Vascular Disease. Trends Endocrinol. Metab. 2001, 12, 225–230.
- Umeda, M.; Kanda, T.; Murakami, M. Effects of Angiotensin II Receptor Antagonists on Insulin Resistance Syndrome and Leptin in Sucrose-Fed Spontaneously Hypertensive Rats. Hypertens. Res. 2003, 26, 485–492.
More