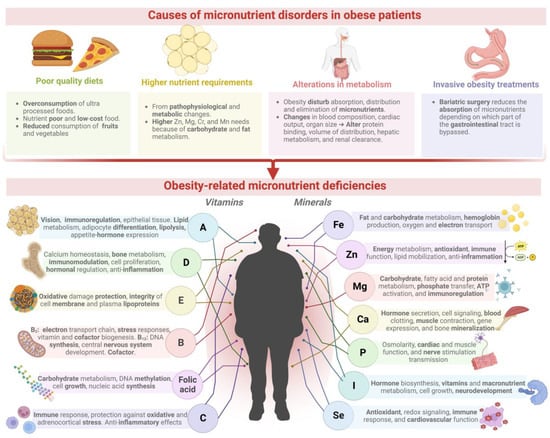
Obesity is a critical medical condition worldwide that is increasingly involved with nutritional derangements associated with micronutrient deficiencies, including iron, zinc, calcium, magnesium, selenium, and vitamins A, C, D, and E. Nutritional deficiencies in obesity are mainly caused by poor-quality diets, higher nutrient requirements, alterations in micronutrient metabolism, and invasive obesity treatments. The current conventional agricultural system is designed for intensive food production, focusing on food quantity rather than food quality, consuming excessive agricultural inputs, and producing nutrient-deficient foods, thus generating severe health and environmental problems; agricultural food products may worsen obesity-related malnutrition. Therefore, modern agriculture is adopting new biofortification technologies to combat micronutrient deficiencies and improve agricultural productivity and sustainability.
- agri-food systems
- beneficial soil microorganisms
- biofertilization
- micronutrients
- nanofertilization
- obesity
- malnutrition
1. Introduction
2. Nutritional Deficiencies Associated with Overweight or Obese Patients
| Micronutrient | Micronutrient Physiologic and Metabolic Function | Deficiency in Obese Patients | Type of Condition | Reference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Vitamin A and carotenoids | Retina and epithelial tissue development, lipid metabolism, immune system function. Inhibition of adipocyte differentiation by enhancing lipolysis. Reduction in leptin and resistin expression [14][47]. | Retina and epithelial tissue development, lipid metabolism, immune system function. Inhibition of adipocyte differentiation by enhancing lipolysis. Reduction in leptin and resistin expression [14,47]. | Carotenoids (α-carotene, β-carotene, ζ-carotene, lutein, and lycopene) ≈ 44.4%. | Male (n = 29) and female (n = 37) individuals between 49 and 58 years old with a body mass index (BMI) > 30 kg/m | 2 | . | [48] | |||
| All evaluated patients presented a deficiency of vitamin A (<30 µg/dL). | Individuals with a BMI over 25 kg/m | 2 | (overweight) and 30 kg/m | 2 | (obesity) aged 18–65 years (n = 127). | [6] | ||||
| Vitamin D | Calcium homeostasis, bone metabolism, immunomodulation, cell proliferation, and control of hormonal systems. Upregulates anti-inflammatory cytokines [49]. | Approximately 16.5% presented a deficiency of serum 25 hydroxy vitamin D (<30 nmol/L). | Danish individuals; 6–18 years old (n = 1484) with overweight/obesity; body mass index standard deviation score (BMI Z-score) > 2.33. | [50] | ||||||
| The prevalence of deficiency (≤20 ng/mL) is around 90%. | Obese individuals class II and III (BMI ≥ 35 and ≥40 kg/m | 2 | ). | [2] | ||||||
| Vitamin E | Protection of cell constituents from oxidative damage, such as polyunsaturated fatty acids found in the membrane and plasma lipoproteins [51]. | Deficiency of 61.5% (11.5 ± 12.2 mg/L), and 47.8% (15.6 ± 12.2 mg/L) in obese and metabolic syndrome patients, respectively. | Individuals 10–16 years old from Central Turkey with obesity (BMI Z-score > 2) (n = 73) or metabolic syndrome (waist circumference ≥ 90 cm (n = 64). | [52] | ||||||
| Vitamin B | 2 | Mitochondrial electron transport chain function and homocysteine metabolism. Its derivatives, flavin mononucleotide and flavin adenine dinucleotide, are implicated in stress responses and vitamin and cofactor biogenesis [53]. | Deficit of 48.9% in the obese group (89.1 ± 35 μg/L); 33.1% in the metabolic syndrome group (116.7 ± 65.2 μg/L). | Individuals 10–16 years old from Central Turkey with obesity (BMI Z-score > 2) (n = 73) or metabolic syndrome (waist circumference ≥ 90 cm (n = 64). | [52] | |||||
| Deficiency of 38.8% (<5 ng/mL). | Children 11–17 years old (n = 50) with obesity (BMI Z-score ≥ 2). | [54] | ||||||||
| Vitamin B | 12 | DNA synthesis, conversion of homocysteine to methionine, and central nervous system development. Cofactor in the one-carbon metabolism and propionate catabolism [55][56]. | DNA synthesis, conversion of homocysteine to methionine, and central nervous system development. Cofactor in the one-carbon metabolism and propionate catabolism [55,56]. | Insufficiency of 23% (< 150 pmol/l) in cohort 1 and 18.3% in cohort 2. | Two cohorts of pregnant women (16–18 weeks) (n = 244 and n = 60) with average BMI = 26.5 ± 5.5 kg/m | 2 | for cohort 1 and BMI = 32.6 ± 11.2 kg/m | 2 | for cohort 2. | [57] |
| Deficiency of around 29% (397.5 ± 26.3 ng/L). | Forty obese adults (BMI > 35 kg/m | 2 | ) aged 21–49 underwent bariatric surgery. | [58] | ||||||
| Folic acid | Well-functioning carbohydrate metabolism (15). DNA methylation, cell growth, and nucleic acid synthesis [56]. | Prevalence of 54% (obese) and 65% (patients after bariatric surgery). | Patients with morbid obesity before (BMI > 30 kg/m | 2 | ) and after bariatric surgery (BMI > 35 kg/m | 2 | ). | [56] | ||
| Inadequacies (<10 nmol/L) per area: America (0.8–2.1%), Europe and Eastern Mediterranean (40.9%), Africa (24.4%), Southeast Asia, and Western Pacific (1.1–3.7%). | Women with a rising prevalence of overweight and/or obesity (BMI > 18.5 kg/m | 2 | ) in reproductive age (15–49 years old) in 17 population surveys. | [59] | ||||||
| Vitamin C | Immune response, protection against oxidative and adrenocortical stress. Anti-inflammatory effects [60]. | Deficit of 24.6%, 32.8%, and 34.6% for sarcopenic, osteopenic, and osteosarcopenic obese individuals. | Korean women (n = 1344) postmenopausal (>50 years old) with osteosarcopenic (BMI = 27.15 kg/m | 2 | ), sarcopenic (BMI = 28.12 kg/m | 2 | ), and osteopenic (BMI = 26.24 kg/m | 2 | ) obesity. | [61] |
| Iron | Fat and carbohydrate metabolism, hemoglobin production, oxygen transport, DNA synthesis, and electron transport [14][62]. | Fat and carbohydrate metabolism, hemoglobin production, oxygen transport, DNA synthesis, and electron transport [14,62]. | Deficiency of 31.8% in male and 25.9% in female patients. | Children 8–9 years old (n = 160) with high body fat (BMI Z-score > 1) in Sri Lanka. | [63] | |||||
| Insufficiency in patients with peripheral (16.9%) and central (10.7%) adiposity. | Overweight and/or obese American young women (23–43 years old; BMI ≥ 25 kg/m | 2 | ; n = 81). | [64] | ||||||
| Zinc | Energy metabolism with antioxidant and immunological properties. Stimulates the function of zinc-α2-glycoprotein (adipokine with lipid mobilizing and anti-inflammatory activity) [65]. | Prevalence of 24–74% after bypass surgery: biliopancreatic bypass (45–91%), gastric bypass (15–21%), laparoscopic sleeve gastrectomy (11–14%). | Patients with morbid obesity before (BMI > 30 kg/m | 2 | ) and after bariatric surgery (BMI > 35 kg/m | 2 | ). | [56] | ||
| Deficiency prevalence of 84.7% (<70 µg/dL fasted). | Women rising prevalence of overweight and/or obesity (BMI > 18.5 kg/m | 2 | ) in reproductive age (15–49 years old). | [59] | ||||||
| Magnesium | Carbohydrate metabolism, phosphate transfer reactions, fatty acid and protein synthesis, ATP activation, and immune system function [62][66]. | Carbohydrate metabolism, phosphate transfer reactions, fatty acid and protein synthesis, ATP activation, and immune system function [62,66]. | Deficiency in males was 6.6%, and, in females, was 7.7%. | Children 8–9 years old (n = 160) with high body fat (BMI Z-score > 1) in Sri Lanka. | [63] | |||||
| Calcium | Hormone secretion, intracellular signaling, blood clotting, muscle contraction, gene expression, and bone mineralization [67][68]. | Hormone secretion, intracellular signaling, blood clotting, muscle contraction, gene expression, and bone mineralization [67,68]. | Deficiency of 50.2% in obese women. | Obese women (35.37 ± 2.09 years old) with average BMI = 34.68 ± 0.61 kg/m | 2 | (n = 70). | [69] | |||
| Potassium | Cellular osmolarity, acid–base equilibrium, cardiac and muscle function, and nerve stimulation transmission [70]. | Deficiency of 59.6% in obese women. | Obese women (35.37 ± 2.09 years old) average BMI= 34.68 ± 0.61 kg/m | 2 | (n = 70) | [69] | ||||
| 100% of patients showed deficiency (<3.5 mmol/L). | Individuals with a BMI over 25 kg/m | 2 | (overweight) and 30 kg/m | 2 | (obesity) aged 18–65 years (n = 127). | [6] | ||||
| Iodine | Thyroid hormones biosynthesis, vitamins, macronutrient metabolism, and cell growth fetal and child neurodevelopment [71][72]. | Thyroid hormones biosynthesis, vitamins, macronutrient metabolism, and cell growth fetal and child neurodevelopment [71,72]. | Insufficiency prevalence of 24.4%. | Overweight (BMI > 25 kg/m | 2 | ) and obese (BMI > 30 kg/m | 2 | ) children (11–13 years old) residing in iodine-sufficient areas (IS) and mildly iodine-deficient areas (ID). | [73] | |
| Selenium | Antioxidant defense, redox signaling, immune response, and cardiovascular function [74]. | Deficiency of 25.9% in plasma and 34.2% in the erythrocyte. | Obese women aged 20–50 years (BMI ≥ 35 kg/m | 2 | , n = 63). | [75] | ||||
| Copper | Electron transport, protein structure, mitochondrial respiratory chain, immune function, antioxidant defense. Cofactor of redox enzymes [56][76]. | Electron transport, protein structure, mitochondrial respiratory chain, immune function, antioxidant defense. Cofactor of redox enzymes [56,76]. | Concentration decreased by 16% 12 months after bariatric surgery. | Norwegian patients (85% women) 27–59 years old, eligible for bariatric surgery (BMI = 42.4 ± 3.6 kg/m | 2 | , n = 46). | [77] | |||
| Prevalence of 46.7%. | Overweight/obese children aged 6–16 years (average BMI = 24.78 ± 3.93 kg/m | 2 | , n = 69). | [78] |