NAFLD is defined by the presence of >5% of hepatic steatosis demonstrated, either radiographically or histologically, in the absence of significant alcohol consumption. Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease worldwide, with a continuously growing prevalence. The pathophysiology of the disease is complex and includes several mechanisms, with metabolic syndrome and insulin resistance playing a major role. It is crucial to diagnose NAFLD before it advances to nonalcoholic steatohepatitis (NASH), which can progress to cirrhosis, presented by its complications which include ascites, portal hypertension, bleeding varices and encephalopathy. Another important complication of NAFLD and cirrhosis is hepatocellular carcinoma (HCC), a cancer with increasing incidence and poor prognosis. Even with the growing prevalence of NAFLD, diagnosis via liver biopsies is unrealistic, considering the costs and complications. Noninvasive tests, including serum biomarkers and elastography, are cost-effective and convenient, thereby replacing liver biopsies in diagnosing and excluding liver fibrosis
- nonalcoholic fatty liver disease (NAFLD)
- metabolic-associated fatty liver disease (MAFLD)
- nonalcoholic steatohepatitis (NASH)
- advanced fibrosis
1. NAFLD Represents a Wide Spectrum of Diseases
2. Metabolic Profile of NAFLD
Much research on NAFLD has been done, but no accurate mechanism has been described yet. A good understanding of the metabolic and biological mechanisms of this situation could help uspeople in developing good predictors and markers. Several theories were suggested in the context of NASH development. The “double-hit” hypothesis suggests that the first insult or the “first hit” is characterized by lipid accumulation in the liver, resulting in steatosis, which enhances the liver’s susceptibility to the “second hit” characterized by inflammation and necrosis induced by oxidative stress and proinflammatory mediators [66,67][17][18]. The simplistic “double-hit” theory was substituted by a more complex theory, the “multiple-hit” hypothesis, which has become more accepted recently, representing the interaction of multiple metabolic and genetic factors leading to the development of NASH. Such “hits” include insulin resistance, hormones secreted from the adipose tissue, nutritional factors, gut microbiota and genetic and epigenetic factors [68][19].2.1. The Role of Adipose Tissue in NAFLD
Obesity is associated with increased prevalence and severity of NAFLD. The adipose tissue functions as an endocrine organ secreting adipokines and cytokines [69][20]. Adiponectin is anti-inflammatory, and its levels are inversely associated with cardiovascular risk factors and visceral adiposity. It increases free fatty acid (FFA) oxidation and decreases gluconeogenesis resulting in decreased liver steatosis. Furthermore, it acts as a pro-inflammatory inhibitor, opposing the effects of tumor necrosis factor (TNF)-α and interleukin (IL)-6 [66,70,71][17][21][22]. Leptin secretion is directly proportional to the white fat mass. Circulating leptin levels are higher in patients with NAFLD than in healthy patients, and higher levels are associated with the severity [72][23]. Leptin has different effects depending on the stage of the disease. At early stages, it acts as an anti-steatotic and increases insulin sensitivity. At more advanced NAFLD stages, it has an unfavorable effect by promoting inflammation [73,74][24][25]. Pro-inflammatory cytokines are immunoregulatory cytokines that favor and enhance the process of inflammation [75][26]. Fat accumulation in the liver mediates cytokine production in hepatic cells. These cytokines induce inflammation, necrosis, cell apoptosis and mediated liver stiffness and fibrosis. Pro-inflammatory cytokines are also secreted by adipose tissue and are involved in the recruitment and activation of macrophages, a process that leads to chronic low-grade inflammation and the development of insulin resistance and cardiovascular diseases [73,74,75,76,77][24][25][26][27][28].2.2. Lipotoxicity in NAFLD
Lipotoxicity is a leading factor in the development and progression of NAFLD and NASH. The total amount of triglycerides stored in the liver cells is not the main determinant of lipotoxicity [76,77][27][28]. Specific lipid classes, especially free fatty acids (FFA), which accumulate in hepatocyte cytoplasm, act as damaging agents via multiple mechanisms. These include activation of death receptors, modification of mitochondrial function and oxidative stress, which lead to the progression from NAFLD to NASH, its inflammatory form. Insulin resistance plays a major role in lipotoxicity by enhancing lipolysis in adipose tissue and increasing the amount of circulation FFAs [76,77][27][28].2.3. The Role of Glucose in NAFLD
High-carbohydrate diets and NAFLD are strongly correlated [78][29]. Hyperglycemia is strongly associated with oxidative stress [79][30], leading to chronic inflammation and insulin resistance [80][31]. Insulin resistance in NAFLD is characterized by reductions in whole-body, hepatic, and adipose tissue insulin sensitivity. The mechanisms underlying the accumulation of fat in the liver may include excess dietary fat, increased delivery of free fatty acids to the liver, inadequate fatty acid oxidation, and increased de novo lipogenesis. Insulin resistance may enhance hepatic fat accumulation by increasing free fatty acid delivery and by hyperinsulinemia to stimulate anabolic processes. The impact of weight loss, metformin, and thiazolidinedione, all treatments aimed at improving insulin sensitivity, as well as other agents such as vitamin E, have been evaluated in patients with NAFLD and have shown some benefit. However, most intervention studies have been small and uncontrolled [81][32].3. Risk Stratification
In light of the increased morbidity and mortality in NAFLD, and considering its wide prevalence, many efforts are put into identifying patients at risk for disease progression to enable early intervention and to prevent the development of cirrhosis [82][33]. Several algorithms were developed to screen NAFLD patients, each relying on different parameters (Figure 1) [83][34]. The European Association for Liver/-Diabetes/-Obesity Guidelines (EASL-EASD-EASO) uses the NFS and FIB-4 scores, while the German National Guidelines use LSM to guide the management of NAFLD patients [82][33].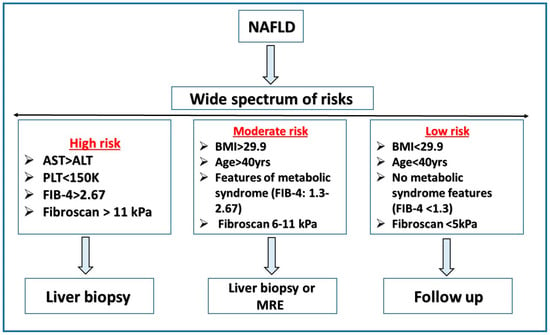
References
- Targher, G.; Corey, K.E.; Byrne, C.D.; Roden, M. The complex link between NAFLD and type 2 diabetes mellitus—Mechanisms and treatments. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 599–612.
- Juanola, O.; Martínez-López, S.; Francés, R.; Gómez-Hurtado, I. Non-alcoholic fatty liver disease: Metabolic, genetic, epigenetic and environmental risk factors. Int. J. Environ. Res. Public Health 2021, 18, 5227.
- Cardoso, A.C.; de Figueiredo-Mendes, C.; Villela-Nogueira, C.A. Current management of NAFLD/NASH. Liver Int. 2021, 41, 89–94.
- Armandi, A.; Bugianesi, E. Natural history of NASH. Liver Int. 2021, 41 (Suppl. 1), 78–82.
- Powell, E.E.; Wong, V.W.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224.
- Taylor, R.S.; Taylor, R.J.; Bayliss, S.; Hagström, H.; Nasr, P.; Schattenberg, J.M.; Ishigami, M.; Toyoda, H.; Wong, V.W.-S.; Peleg, N.; et al. Association Between Fibrosis Stage and Outcomes of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Gastroenterology 2020, 158, 1611–1625.e12.
- Ioannou, G.N. Epidemiology and risk-stratification of NAFLD-associated HCC. J. Hepatol. 2021, 75, 1476–1484.
- Calzadilla Bertot, L.; Adams, L.A. The Natural Course of Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2016, 17, 774.
- Zheng, Q.; Martin, R.C.; Shi, X.; Pandit, H.; Yu, Y.; Liu, X.; Guo, W.; Tan, M.; Bai, O.; Meng, X.; et al. Lack of FGF21 promotes NASH-HCC transition via hepatocyte-TLR4-IL-17A signaling. Theranostics 2020, 10, 9923–9936.
- Allen, A.M.; Hicks, S.B.; Mara, K.C.; Larson, J.J.; Therneau, T.M. The risk of incident extrahepatic cancers is higher in non-alcoholic fatty liver disease than obesity—A longitudinal cohort study. J. Hepatol. 2019, 71, 1229–1236.
- Lombardi, R.; Iuculano, F.; Pallini, G.; Fargion, S.; Fracanzani, A.L. Nutrients, Genetic Factors, and Their Interaction in Non-Alcoholic Fatty Liver Disease and Cardiovascular Disease. Int. J. Mol. Sci. 2020, 21, 8761.
- Sakurai, Y.; Kubota, N.; Yamauchi, T.; Kadowaki, T. Role of Insulin Resistance in MAFLD. Int. J. Mol. Sci. 2021, 22, 4156.
- Watt, M.J.; Miotto, P.M.; De Nardo, W.; Montgomery, M. The Liver as an Endocrine Organ—Linking NAFLD and Insulin Resistance. Endocr. Rev. 2019, 40, 1367–1393.
- Maurice, J.; Manousou, P. Non-alcoholic fatty liver disease. Clin. Med. 2018, 18, 245–250.
- Huang, R.; Zhu, L.; Wang, J.; Xue, L.; Liu, L.; Yan, X.; Huang, S.; Li, Y.; Yan, X.; Zhang, B.; et al. Clinical features of COVID-19 patients with non-alcoholic fatty liver disease. Hepatol. Commun. 2020, 4, 1758–1768.
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Non-alcoholic fatty liver diseases in patients with COVID-19: A retrospective study. J. Hepatol. 2020, 73, 451–453.
- Berlanga, A.; Guiu-Jurado, E.; Porras, J.A.; Auguet, T. Molecular Pathways in Non-Alcoholic Fatty Liver Disease. Clin. Exp. Gastroenterol. 2014, 7, 221–239.
- Abenavoli, L.; Milic, N.; Di Renzo, L.; Preveden, T.; Medić-Stojanoska, M.; De Lorenzo, A. Metabolic aspects of adult patients with nonalcoholic fatty liver disease. World J. Gastroenterol. 2016, 22, 7006–7016.
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 2016, 65, 1038–1048.
- Makri, E.; Goulas, A.; Polyzos, S.A. Epidemiology, Pathogenesis, Diagnosis and Emerging Treatment of Nonalcoholic Fatty Liver Disease. Arch. Med. Res. 2020, 52, 25–37.
- Milić, S.; Lulić, D.; Štimac, D. Non-alcoholic fatty liver disease and obesity: Biochemical, metabolic and clinical presentations. World J. Gastroenterol. 2014, 20, 9330–9337.
- Shabalala, S.C.; Dludla, P.V.; Mabasa, L.; Kappo, A.P.; Basson, A.K.; Pheiffer, C.; Johnson, R. The Effect of Adiponectin in the Pathogenesis of Non-Alcoholic Fatty Liver Disease (NAFLD] and the Potential Role of Polyphenols in the Modulation of Adiponectin Signaling. Biomed. Pharmacother. 2020, 131, 110785.
- Polyzos, S.A.; Aronis, K.; Kountouras, J.; Raptis, D.D.; Vasiloglou, M.; Mantzoros, C.S. Circulating leptin in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Diabetologia 2015, 59, 30–43.
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92, 82–97.
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Leptin in nonalcoholic fatty liver disease: A narrative review. Metabolism 2015, 64, 60–78.
- Stojsavljević, S.; Gomerčić Palčić, M.; Virović Jukić, L.; Smirčić Duvnjak, L.; Duvnjak, M. Adipokines and proinflammatory cytokines, the key mediators in the pathogenesis of nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 18070–18091.
- Svegliati-Baroni, G.; Pierantonelli, I.; Torquato, P.; Marinelli, R.; Ferreri, C.; Chatgilialoglu, C.; Bartolini, D.; Galli, F. Lipidomic biomarkers and mechanisms of lipotoxicity in non-alcoholic fatty liver disease. Free Radic. Biol. Med. 2019, 144, 293–309.
- Branković, M.; Jovanović, I.; Dukić, M.; Radonjić, T.; Oprić, S.; Klašnja, S.; Zdravković, M. Lipotoxicity as the Leading Cause of Non-Alcoholic Steatohepatitis. Int. J. Mol. Sci. 2022, 23, 5146.
- Basaranoglu, M.; Basaranoglu, G.; Bugianesi, E. Carbohydrate intake and nonalcoholic fatty liver disease: Fructose as a weapon of mass destruction. Hepatobiliary Surg. Nutr. 2015, 4, 109–116.
- Gjorgjieva, M.; Mithieux, G.; Rajas, F. Hepatic stress associated with pathologies characterized by disturbed glucose production. Cell Stress 2019, 3, 86–99.
- Xian, Y.X.; Weng, J.P.; Xu, F. MAFLD vs. NAFLD: Shared Features and Potential Changes in Epidemiology, Pathophysiology, Diagnosis, and Pharmacotherapy. Chin. Med. J. 2020, 134, 8–19.
- Dyson, J.K.; McPherson, S.; Anstee, Q.M. Republished: Non-alcoholic fatty liver disease: Non-invasive investigation and risk stratification. Postgrad. Med. J. 2014, 90, 254–266.
- Blank, V.; Petroff, D.; Beer, S.; Böhlig, A.; Heni, M.; Berg, T.; Bausback, Y.; Dietrich, A.; Tönjes, A.; Hollenbach, M.; et al. Current NAFLD guidelines for risk stratification in diabetic patients have poor diagnostic discrimination. Sci. Rep. 2020, 10, 18345.
- Rinella, M.E.; Sanyal, A.J. Management of NAFLD: A stage-based approach. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 196–205.