1. Available Perceived Exertion Definitions
Researchers have recently discussed the meaning of perceived exertion, which may have implications for defining and applying the construct in the practical context
[1][2][3][16,33,34]. Gunnar Borg proposed that sensory information from skeletal muscles, joints, the cardiorespiratory system, and any other organ would generate sensations such as pain, fatigue (weakness), strain, and breathlessness. Together, these sensations would form the perceived exertion, a kind of gestalt (i.e., a whole inexplicable by its parts individually) related to the exercise requirement
[4][5][6][3,4,7]. Past experiences, expectations about exercise performance, psychological features, environmental conditions, exercise characteristics, and emotions associated with the exercise-evoked sensations would also weigh on the reported perceived exertion
[5][7][4,35]. Based on these assumptions, Gunnar Borg defined perceived exertion as a “feeling of how heavy, strenuous, and laborious the exercise is” according to the sensation of strain and fatigue in the skeletal muscles and breathlessness or aches in the chest
[5][4].
Robert Robertson and Bruce Noble defined perceived exertion as a “subjective intensity of effort, strain, discomfort, and/or fatigue that is experienced during physical exercise”
[8][17]. This definition somewhat agrees with Gunnar Borg’s idea that somatic information from different organs would generate sensations that together would form the perceived exertion. However, people can differentiate several bodily sensations arising during exercise
[1][9][10][11][12][13][14][15][16][16,36,37,38,39,40,41,42,43]. For example, if clear instructions are given, it is possible to discriminate the sense of effort to command skeletal muscles from the sensations of force, pain, or discomfort evoked by muscle contractions
[1][9][10][12][16][16,36,37,39,43]. It is also possible to differentiate the sensations of respiratory effort from the feelings of “air hunger” (insufficient inspiration), breathlessness, and chest tightness
[11][13][14][38,40,41]. Such differentiations possibly occur because different neurophysiological mechanisms are involved in the genesis of each of these sensations
[1][9][10][17][18][2,16,36,37,44]. Thus, considering all exercise-evoked somatic sensations together could hinder the rating accuracy of the perceived exertion
[1][19][16,30].
Samuele Marcora suggested defining perceived exertion as a “conscious sensation of how hard, heavy, and strenuous a physical task is”
[19][20][21][8,30,45]. This sensation, however, would depend mainly on the sense of effort to command the involved limbs during the physical task and the feeling of heavy breathing
[21][45]. Given that people can accurately differentiate the sense of effort to command skeletal muscles (locomotor and respiratory) from other exercise-evoked somatic sensations, such as tension, force, pain, discomfort, and breathlessness
[1][9][10][11][12][13][14][15][16][16,36,37,38,39,40,41,42,43], it seems that the definition proposed by Samuele Marcora is more accurate for classifying the perceived exertion. It is also worth noting that Marcora’s definition enables quantifying perceived exertion according to the RPE and CR10 scales descriptors, and several studies have shown that perceived exertion is sensitive to different physiological and psychological manipulations using Marcora’s definition
[1][19][16,30].
2. Neurophysiological Mechanisms Associated with Perceived Exertion
Two theories are frequently used to describe the origin of the neural signals responsible for the genesis of the perceived exertion during exercise
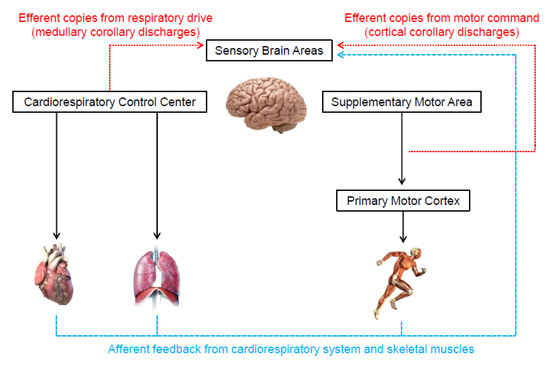
[1][19][20][21][22][8,15,16,30,45]. One of them, known as the afferent feedback theory (
Figure 13), holds that sensory brain areas produce the perceived exertion proportionally to mechanical and metabolic signals detected by receptors in the skeletal muscles and cardiorespiratory system
[1][5][23][24][4,11,13,16]. The same neural signals are also crucial for cardiorespiratory responses to exercise
[25][26][46,47]. Thus, presumably, perceived exertion and cardiorespiratory responses should be tightly associated. Indeed, several studies have shown high correlations between perceived exertion, heart rate, and pulmonary ventilation responses to exercise
[27][28][48,49].
Figure 13.
Illustration of the neurophysiological mechanisms underlying the genesis of perceived exertion during exercise.
Some researchers, however, argue that available evidence does not support the afferent feedback theory
[1][19][22][15,16,30]. For instance, beta-blockers or mental fatigue can dissociate perceived exertion and heart rate responses to exercise
[22][29][30][15,50,51]. Moreover, information from mechano- and chemo-receptors in the respiratory system (airways, lungs, and chest wall) do not seem to be involved in generating the respiratory effort sensation (i.e., heavy breathing), which is an essential component of perceived exertion during whole-body exercise
[11][19][22][31][15,30,38,52]. Finally, experimental studies that partially blocked group III and IV muscle afferents typically do not show changes in perceived exertion during exercise compared to a control condition
[19][22][32][33][34][15,30,53,54,55]. Nevertheless, a cautious interpretation is required, considering that some of the mentioned studies were not specifically designed to investigate the neurophysiological mechanisms behind the perceived exertion during exercise
[32][33][34][53,54,55].
In contrast to the afferent feedback theory, the corollary discharges theory (
Figure 13) proposes that the signals that generate the perceived exertion come from efferent copies associated with the motor command to locomotor muscles and the central drive to respiratory muscle
[2][19][22][15,30,33]. Specifically, outputs from the supplementary motor area and medullary respiratory center are sent directly to sensory areas. These signals are parallel (i.e., corollary discharges) and somewhat independent of the signals sent to locomotor and respiratory muscles
[1][2][19][20][21][22][35][36][37][38][39][8,15,16,30,33,45,56,57,58,59,60]. In support, experimental findings have shown that perceived exertion accompanies the changes in motor-related cortical potential (a proxy to central motor command) induced by manipulations that do not alter afferent signals (e.g., use of caffeine or eccentric exercise-induced force reduction)
[35][36][56,57]. Therefore, these findings indicate that corollary discharges, rather than afferent signals, are vital to the generation and modulation of perceived exertion. However, researchers opposed to the afferent feedback theory have not considered that the redundancy and interaction between neurophysiological mechanisms are crucial for cardiovascular and respiratory adjustments to exercise
[25][26][40][46,47,61]. Such a phenomenon likely contributes to the formation of perceived exertion as well. Thus, next,
it w
ase propose
d how both theories might physiologically operate together, which should be taken into account by future studies.
Recent evidence has suggested that the genesis of perceived exertion during high-intensity exercise can indirectly involve the afferent feedback from the skeletal muscle and cardiorespiratory system. For example, the activation of group III and IV afferents receptors in the locomotor muscles by metabolite accumulation reduces the excitability of the primary motor cortex, hindering muscle recruitment
[41][42][43][44][45][62,63,64,65,66].
HIn this case
rein, the supplementary motor area has to increase the signals to the primary motor cortex to preserve the muscle power output, which provides additional corollary discharges for the genesis of the perceived exertion
[1][35][36][37][39][46][16,56,57,58,60,67]. In addition, the elevated respiratory work may generate metabolite accumulation in the respiratory muscles, which also activates underlying group III and IV afferent fibers
[47][48][49][68,69,70]. The activation of respiratory muscle afferents leads to sympathetically-mediated vasoconstriction that impairs the oxygen supply to the locomotor muscles, exacerbating metabolite accumulation in both locomotor and respiratory and ultimately inducing primary motor cortex inhibition
[41][42][43][44][45][47][48][49][62,63,64,65,66,68,69,70]. Again, enhanced activation of the supplementary motor area would be required to sustain the muscle power output, potentially increasing corollary discharges. Supporting evidence is the increase in diaphragmatic muscle activation (i.e., EMG response) associated with a decline in evoked transdiaphragmatic twitch pressure during an incremental exercise
[50][71]. In this scenario, an increase in medullary corollary discharges would also contribute to the rise in the perceived exertion.
3. Methodological Issues to Quantify Perceived Exertion
Some methodological issues are fundamental to quantifying the perceived exertion during exercise accurately. One of these issues is using the original versions of the scales, regardless of whether it is Borg’s scale or not. The previous section showed that the psychophysics properties of the RPE and CR10 scales were carefully verified and validated over several years. It is, therefore, inappropriate altering the RPE and CR10 scales by using figures, colors, other non-tested verbal descriptors, or verbal descriptors for all scale numbers
[1][51][16,26]. Considering that the scales were developed in English, if using the scales in another language, it is also strongly recommended to verify if the translated version has passed a thorough transcultural validation process
[52][72]. Translated versions of the RPE and CR10 in various languages are available from the Swedish company website licensed to distribute Borg’s scales (
https://borgperception.se, accessed on 1 November 2022). Moreover, practitioners should ideally obtain perceived exertion during exercise
[1][5][4,16]. If not possible, an option is obtaining values immediately after exercise. However, practitioners should remind the tested individual to report values referring to the exercise performed
[1][16].
Providing written instructions when obtaining perceived exertion was a methodological procedure originally recommended by Gunn
aer Borg
[5][4], which a review article recently reinforced
[1][16]. Given that these instructions were developed in English, transcultural adaptation to other languages should also be considered
[52][72]. Similar to Borg’s scales, translated versions of the instructions are also available (
https://borgperception.se, accessed on 1 November 2022). However, practitioners should be aware that the instructions were developed using Borg’s definition of perceived exertion
[5][52][4,72]. As
it w
ase pointed out in the previous paragraphs, contemporary studies support that it is essential to distinguish effort sensation to command skeletal muscles (locomotor and respiratory) from other exercise-evoked somatic sensations (e.g., pain or breathlessness). Clear instructions differentiating the sensations can be critical for accurate perceived exertion quantification
[1][16].
In the written instructions, individuals should be oriented first to read the descriptors and then to quantify the perceived exertion
[1][5][4,16]. In the case of the CR10 scale, individuals should be encouraged to report decimal values (e.g., 0.5), thus grading more finely the perceived exertion magnitude
[1][5][19][51][4,16,26,30]. Providing an example of maximal perceived exertion to the individuals is strongly recommended. This anchoring process can be done based on the individual’s memory or the individual’s experience with a performed exercise
[1][5][30][4,16,51]. In the case of the CR10 scale, values above 10 are possible if the current perception is more intense than previous experiences. The anchoring process and the clear construct definition are essential procedures for a valid measure of perceived exertion
[8][17]. Lastly, it is worth reminding the individuals to be as honest as possible and avoid comparing with others. It is also encouraged to avoid judgments about exercise intensity that can result in the tested individual underestimating or overestimating the reported perceived exertion
[5][4].
4. Practical Applications of Perceived Exertion Measurement
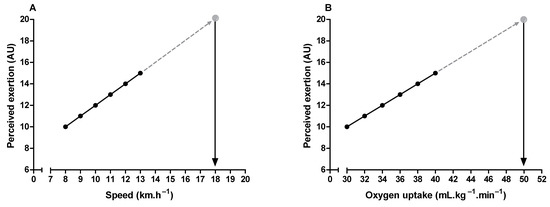
Maximal oxygen uptake and peak exercise intensity are frequently used to assess cardiorespiratory fitness and individualize exercise prescription, respectively
[53][54][73,74]. It is possible to estimate these parameters through the perceived exertion when it is undesirable to push the incremental exercise testing until the subject’s voluntary exhaustion
[55][56][57][58][6,75,76,77]. It is only necessary to extrapolate the submaximal relationship between perceived exertion and oxygen uptake or exercise intensity to a theoretical endpoint (i.e., 19 or 20) on the RPE scale (
Figure 24). It is also possible to estimate the time to exhaustion during constant-load exercise tests, given the linear relationship between perceived exertion and exercise time
[59][60][9,78]. Additionally, the product between perceived exertion and remaining distance fraction (i.e., hazard score) can predict the subsequent running speed change during time-trials tests (e.g., completing 5 km in the shortest time). Hazard scores below 1.5 and above 3 arbitrary units are associated with a reduction and an increase in the running speed, respectively
[61][79].
Figure 24. Illustration of peak exercise intensity (A) and maximum oxygen uptake (B) estimation through perceived exertion measurement during submaximal incremental exercise testing.
Critical power delimits the transition between heavy and severe exercise intensity domains
[62][63][80,81]. In the exercise above the critical power (i.e., severe-intensity domain), fatigue-related metabolites accumulate (e.g., inorganic phosphate and hydrogen ions) over time in the skeletal muscle
[63][64][65][81,82,83], limiting the capacity to sustain the exercise for a prolonged time
[63][81]. Therefore, critical power is a valuable tool for continuous or interval endurance training prescription, and it is considered an important indicator of performance in endurance sports
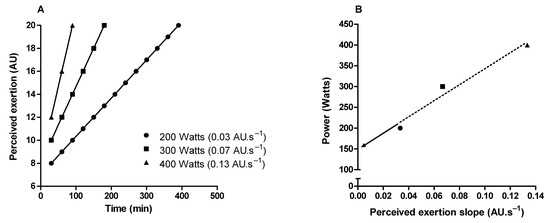
[62][63][66][80,81,84]. It is possible to approximate the critical power through perceived exertion slopes obtained from three or more constant-load exercise tests in the severe-intensity domain
[67][68][69][85,86,87]. The intercept between exercise intensity and perceived exertion slopes approximates the critical power (
Figure 35). Importantly, this method of critical power approximation does not require exercise until exhaustion, as the perceived exertion slopes can be obtained from intermediate levels (11–14 on the RPE scale) of perceived exertion
[69][87].
Figure 35. Illustration of critical power determination by obtaining the perception of exertion throughout constant load tests in the severe-intensity domain. (A) Shows perceived exertion over time in three constant-load exercise tests. (B) Shows the linear relationship between the power used in the constant-load exercises tests and the rate of perceived exertion increase over time (perceived exertion slope). Critical power is the intercept (arrow) of the linear regression.
Monitoring athletes’ responses to training (i.e., training effect) can provide valuable information to refine the training process, maximizing the chances of improving sports performance and minimizing the risk of injury, illness, nonfunctional overreaching, or overtraining
[70][71][88,89]. It is possible to track physical fitness changes by quantifying the workload during incremental exercise testing corresponding to a specific level of perceived exertion (e.g., 15 or 17 on the RPE scale)
[8][29][17,50]. For example, an increased workload to the same level of perceived exertion represents an improvement in physical fitness—i.e., a positive training effect
[8][29][17,50]. In addition, when athletes are in a state of accumulated fatigue due to an imbalance between training loads and recovery periods, a lower heart rate accompanies a higher perceived exertion for a given workload
[72][73][90,91]. Heart rate reduction for the same exercise intensity most often indicates positive training adaptations
[74][75][92,93]. Therefore, measuring perceived exertion simultaneously with heart rate during constant-load exercise tests seems to permit more accurate monitoring of the athletes’ responses to training.
The aforementioned practical applications are based on measuring perceived exertion during an externally imposed-exercise intensity (estimation approach). An alternative approach would be self-regulating exercise intensity while maintaining a given perceived exertion over time (production approach). For example, evidence suggests that incremental exercise testing self-regulated by perceived exertion can produce similar values of maximal oxygen uptake and ventilatory threshold compared with traditional protocols, but it seems unfeasible to determine the respiratory compensation point
[76][77][78][94,95,96]. Moreover, several studies have also shown that self-regulation of exercise intensity by perceived exertion produces similar cardiorespiratory and metabolic responses to those obtained during incremental exercise testing for the same perceived exertion
[8][79][80][81][17,19,20,97]. It is, therefore, possible to use the perceived exertion corresponding to percentages of maximal oxygen uptake or maximal heart rate obtained in incremental testing (e.g., 60% and 80%) to control exercise intensity during training sessions
[8][80][17,20], which has important practical implications when prescribing exercise for health or throughout rehabilitation programs.