Phytosterols are important constituents of plant cells structural analogous of mammalian cholesterol, that have been shown to exert very important biological effects, such as hypocholesterolemic, antidiabetic, and antioxidant activities in the human body. The action mechanisms are yet poorly understood until now thus the aim of this contribution is to present the most current scientific information on phytosterols' biological effects and their mechanism of action.
- Phytosterol
- Dyslipidemia
- Cholesterol
1. Introduction
A high level of LDL cholesterol in the plasma, due to an incorrect diet, is connected to the onset of coronary diseases, which are one of the main causes of death and significantly also affects the health care cost. The reduction of cholesterol levels in plasma prevents many cardiovascular diseases. A way to achieve this objective, and avoid drugs’ use, could be the consumption of phytosterol-enriched/fortified foods.
2. Effects and Action Mechanisms
Although cholesterol and phytosterols have a similar structure, they are absorbed and metabolized by the human body with different efficiency. As a matter of fact, while the absorption of cholesterol is between 20% and 80%, the absorption of phytosterols is approximately 2–5%. As a consequence of this, the plasma levels of phytosterols are very low (0.10–0.14% of the cholesterol levels). Phytostanols are absorbed even less efficiently than the cholesterol and their blood levels are equal to one-tenth of those of phytosterols [12][1]. The phytosterols and cholesterol, which come through the diet or with the enterohepatic circulation in the small intestine, are incorporated into micelles, which, interacting with the apical membrane of the enterocytes, are incorporated into the intestinal cells [5][2]. The intestinal absorption of cholesterol and phytosterols/phytostanols occurs through a complex multistep process. Within the enterocyte, cholesterol is esterified by the enzyme AcilCoA:cholesterol acyl transferase-2 (ACAT2) and becomes part of the chylomicrons, lipoproteins rich in triglycerides that carry the dietary fats in the plasma. The low plasma concentrations of phytosterols could depend on their poor affinity for the ACAT2 enzyme, which would prevent their incorporation into the chylomicrons. The nonesterified cholesterol and phytosterols are transported back to the intestinal lumen and from there to the liver via the enterohepatic circulation. This step is extremely important since it counteracts the sterols’ accumulation into the enterocyte, preventing the formation of cytotoxic products of the lipid peroxidation. The leakage of cholesterol and phytosterols from the enterocyte is mediated by carriers of the “ATP-binding cassette transporters” or ABC transporters named ABCG5 and ABCG8 [13][3]. There are several mechanisms of action through which the phytosterols reduce the blood cholesterol level. The most important mechanism is the competition of phytosterols with cholesterol for incorporation into the mixed micelles in the intestinal chyme, because of the structural similarity of the two molecules. In this way, cholesterol remains not solubilized, its absorption is reduced, and it will be expelled through the feces [14][4]. Secondly, phytosterols interfere with the normal mechanisms responsible for maintaining intracellular cholesterol homeostasis. This effect depends on many factors, including the activity of the ABC transporters. In fact, phytosterols compete with cholesterol during its transport into enterocytes by means of the NPC1L1 (Niemann-Pick C1 Like 1) transport proteins. Once in the enterocytes, phytosterols are preferentially transported back out into the lumen by ABCG5 and G8 heterodimer complex. Phytosterols, which are incorporated into chylomicrons and enter into the circulatory system, are excreted from the liver into the bile by this ABCG5/G8 system (Figure 1) [14][4].
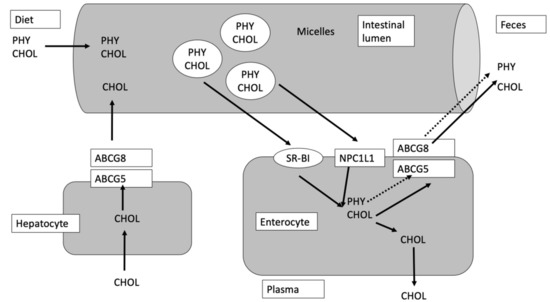
Figure 1. Transport mechanism of CHOL (cholesterol) and PHY (phytosterols), modified from Jesch and Carr [5][2]. SR-BI is the scavenger receptor class B type I, NPC1L1 is the Neiman-Pick C1 Like 1 and ABCG5 and ABCG8 are the transporters ATP binding cassette (ABC) G5 and G8, respectively.
The reduced intestinal absorption of cholesterol (consequent to the modification of mixed micelles induced by phytosterols) can lead to an increase in both the synthesis of endogenous cholesterol and the uptake of lipoproteins in the liver. In fact, when the cholesterol concentration inside the cell goes down, the sterol regulatory element-binding proteins (SREBPs) activate the transcription of both the enzyme 3-Hydroxy-3-methylglutaryl-CoA reductase (HMGCR) and the receptor for LDL, causing an increase of the endogenous biosynthesis of cholesterol and of the LDL cells’ uptake, respectively. Both effects lead to an overall reduction in circulating cholesterol [15][5]. In contrast to the favorable effects of plant sterols on cholesterol serum levels, in some cases they are considered atherogenic, but only where there is a rare genetic disease called sitosterolemia (or phytosterolemia). Sitosterolemia is a rare autosomal recessive inherited disorder, resulting from a mutation in either the ABCG5 or the ABCG8 gene, in which phytosterols are over-absorbed and accumulate in the tissues, causing xanthomatosis and premature atherosclerotic diseases [16,17][6][7]. Before the first description of sitosterolemia, it was believed that plant sterols were not absorbed by the human body. In 1974, for the first time, it was diagnosed a case of sitosterolemia in the United States and, with subsequent studies, the mechanisms by which this disease is generated were also explained. Afterwards, it was estimated that the mean consumption of plant sterols is about 400 mg/day; healthy subjects absorb less than 5% (while plant stanols are absorbed only for 0.5%). In sitosterolemic patients it was found a high concentration of phytosterols in the plasma, ranging from 10 to 65 mg/dL, and also an increase in the levels of cholestanol, 5α-campestanol, and 5α-sitostanol, starting from their unsaturated precursors. The symptoms of this disease can be confused with cases of hypercholesterolemia or xanthomatosis, but it can be discriminated from these disorders because the only clinical sign of sitosterolemia is an abnormal hematological parameter. In fact, a sitosterolemic patient exhibits normal or slightly increased cholesterol levels. Furthermore, it is believed that extremely high levels of plant sterols cause stiffness of the membrane, rupture of red blood cells, and changes in platelet size, number, and function, which occasionally causes bleeding episodes. The known therapy for sitosterolemia consists of a diet low in plant sterols. Fortunately, this is a rare disease [18,19][8][9]. Another negative effect linked to the consumption of phytosterols is the reduction of levels of fat-soluble vitamins. In fact, as phytosterols reduce the absorption of cholesterol by a mechanism of competition with it for the incorporation into mixed micelles, there is also a lower absorption of other lipophilic compounds, such as β-carotene, α-carotene, and vitamin E (tocopherols). The effect of phytosterols and phytostanols on the absorption of fat-soluble vitamins has been known since the year 2000 when the first phytosterols-enriched foods present in the market were deeply studied. The commercialization approval for these foods was issued with the condition that the labeling state that “the product may not be nutritionally appropriate for certain sections of the population (pregnant and breastfeeding women and children under the age of five years)” and “the product should be used as part of a healthy diet, including regular consumption of fruit and vegetables (to help to maintain carotenoid levels)”.
The different studies led to the conclusion that there is a reduction of the level of about 24% of β-carotene and a reduction of about 9% for α-carotene, while there are no significant changes for retinol (vitamin A) and vitamin D. However, this negative effect can easily be countered by eating more colored fruits and vegetables [20][10].
References
- A Berger; Peter J H Jones; Suhad S. AbuMweis; Plant sterols: factors affecting their efficacy and safety as functional food ingredients. Lipids in Health and Disease 2004, 3, 5-5, 10.1186/1476-511X-3-5.
- Rúbia C.G. Corrêa; Rosane M. Peralta; Adelar Bracht; Isabel C. F. R. Ferreira; The emerging use of mycosterols in food industry along with the current trend of extended use of bioactive phytosterols. Trends in Food Science & Technology 2017, 67, 19-35, 10.1016/j.tifs.2017.06.012.
- Richard E Ostlund; Phytosterols and cholesterol metabolism. Current Opinion in Lipidology 2004, 15, 37-41, 10.1097/00041433-200402000-00008.
- Dylan S. Mackay; Peter J. H. Jones; Phytosterols in human nutrition: Type, formulation, delivery, and physiological function. European Journal of Lipid Science and Technology 2011, 113, 1427-1432, 10.1002/ejlt.201100100.
- Ariënne De Jong; Jogchum Plat; Ronald P Mensink; Metabolic effects of plant sterols and stanols (Review). The Journal of Nutritional Biochemistry 2003, 14, 362-369, 10.1016/s0955-2863(03)00002-0.
- Izar, M.C.; Tegani, D.M.; Kasmas, S.H.; Fonseca, F.A. Phytosterols and phytosterolemia: Gene–diet interactions. Genes Nutr. 2011, 6, 17–26.
- Bain, B.J.; Chakravorty, S. Phytosterolemia. Am. J. Hematol. 2016, 91, 643.
- Tzavella, E.; Hatzimichael, E.; Kostara, C.; Bairaktari, E.; Elisaf, M.; Tsimihodimos, V. Sitosterolemia: A multifaceted metabolic disorder with important clinical consequences. J. Clin. Lipidol. 2017, 11, 1095–1100.
- Vergès, B.; Fumeron, F. Potential risks associated with increased plasma plant-sterol levels. Diabetes Metab. 2015, 41, 76–81.
- Anthony Fardet; Anne Morise; Esther Kalonji; Irène Margaritis; François Mariotti; Influence of Phytosterol and Phytostanol Food Supplementation on Plasma Liposoluble Vitamins and Provitamin A Carotenoid Levels in Humans: An Updated Review of the Evidence. Critical Reviews in Food Science and Nutrition 2015, 57, 1906–1921, 10.1080/10408398.2015.1033611.