There is a growing interest among people in western countries for adoption of healthier lifestyle habits and diet behaviors with one of the most known ones to be Mediterranean diet (Med-D). Med-D is linked with daily consumption of food products such as vegetables, fruits, whole grains, seafood, beans, nuts, olive oil, low-fat food derivatives and limited consumption of meat or full fat food products. Med-D is well-known to promote well-being and lower the risk of chronic conditions such as cardiovascular diseases, diabetes, and metabolic syndrome. On the other hand, bioactive constituents in foods may interfere with drugs’ pharmacological mechanisms, modulating the clinical outcome leading to drug-food interactions (DFIs). This textreview discusses current evidence for food products that are included within the Med-D and available scientific data suggest a potential contribution in DFIs with impact on therapeutic outcome. Proper patient education and consultation from healthcare providers is important to avoid any conflicts and side effects due to clinically significant DFIs.
1. Introduction
Mediterranean diet (Med-D) represents one of the most famous and well received diet food habits, particularly in the western countries
[1]. Med-D originates from the eating patterns that people around Mediterranean basin have been following since the ancient years, along with the adoption of food products that were cultivated later in the area (i.e., potatoes)
[2][3][2,3]. Med-D promotes the consumption of all food types but focuses on vegetables, fruits, the nearly exclusive use of olive oil in food preparation, routine consumption of marine food, low fat white meat (chicken, turkey) along with cereals, grains, nuts, wine and lesser consumption of high-fat meat products
[3]. UNESCO states regarding Med-D:
“The Mediterranean diet is characterized by a nutritional model that has remained constant over time and space, consisting mainly of olive oil, cereals, fresh or dried fruit and vegetables, a moderate amount of fish, dairy and meat, and many condiments and spices, all accompanied by wine or infusions, always respecting beliefs of each community” [4]. Since the first observations in 1960s
[5], Med-D has shown undisputable, longitudinal, and high-quality evidence to support its health benefits against specific diseases for people that remain adherent to Med-D dietary patterns
[6][7][8][9][6,7,8,9]. A reduced risk of overall mortality related with metabolic syndrome, cardiovascular diseases, coronary heart disease, myocardial infarction, cancer incidence, diabetes, neurodegenerative diseases, kidney disease and arthritis are mostly identified regarding clinical data availability
[10][11][12][13][14][15][16][17][18][19][20][21][10,11,12,13,14,15,16,17,18,19,20,21]. Moreover, for Med-D food products we can recognize specific active constituents (i.e., oleuropein, resveratrol, retinoids, flavonoids, terpenes, catechins, ω-3-fatty acids etc.) with pharmacological effects (i.e., anti-oxidant and anti-inflammatory) that are related with the health benefits from adherence in Med-D
[22][23][24][25][26][27][28][29][30][31][22,23,24,25,26,27,28,29,30,31]. In this respect, the question that arises is whether there could be cases in which pharmacologically active compounds that are present in Med-D foods could potentially interfere with the pharmacological action of drugs and lead in clinically significant DFIs.
Drug interactions are an important clinical issue for optimum healthcare provision. The proper drug administration and drug combinations ensures the minimization of risks for adverse drug reactions (ADRs) due to drug-drug interactions
[32][33][34][32,33,34]. Moreover, drug interactions can emerge due to co-administration of several complementary and alternative medicine (CAM) products such as herbal medicinal products (HMPs) as well as dietary supplements (DS) and food products
[35][36][37][38][35,36,37,38]. A DFI describes the physical, biochemical or physiological modulation of a pharmacological process that a drug is following due to the presence of one or more constituents within a food product or other nutraceuticals
[39][40][39,40]. These bioactive constituents that are present in dietary products may interfere with drugs’ biological pathways and alter drugs’ pharmacological action or levels in the body. Especially for food products there are well-established clinical examples of drug-food interaction (DFI) such as foods containing tyramine and monoamine-oxidase inhibitors (MAOIs), alcoholic beverages or spirits with central nervous system (CNS) drugs as well as grapefruit and its impact in systemic concentration of several drugs
[38][41][42][43][38,41,42,43]. Overall, DFIs can occur during the habitual use of certain foods whose components can modify pharmacological processes and pathways that take place in the body for drugs. These pathways can be related with the absorption, distribution, metabolism, and elimination processes (pharmacokinetic drug-food interactions, PK-DFIs) or with biological pathways related with the main—or secondary—pharmacological action of a drug (pharmacodynamic drug-food interactions, PD-DFIs)
[44][45][44,45].
2. Mediterranean Food Products and Potential DFIs
2.1. Med-D Food Products
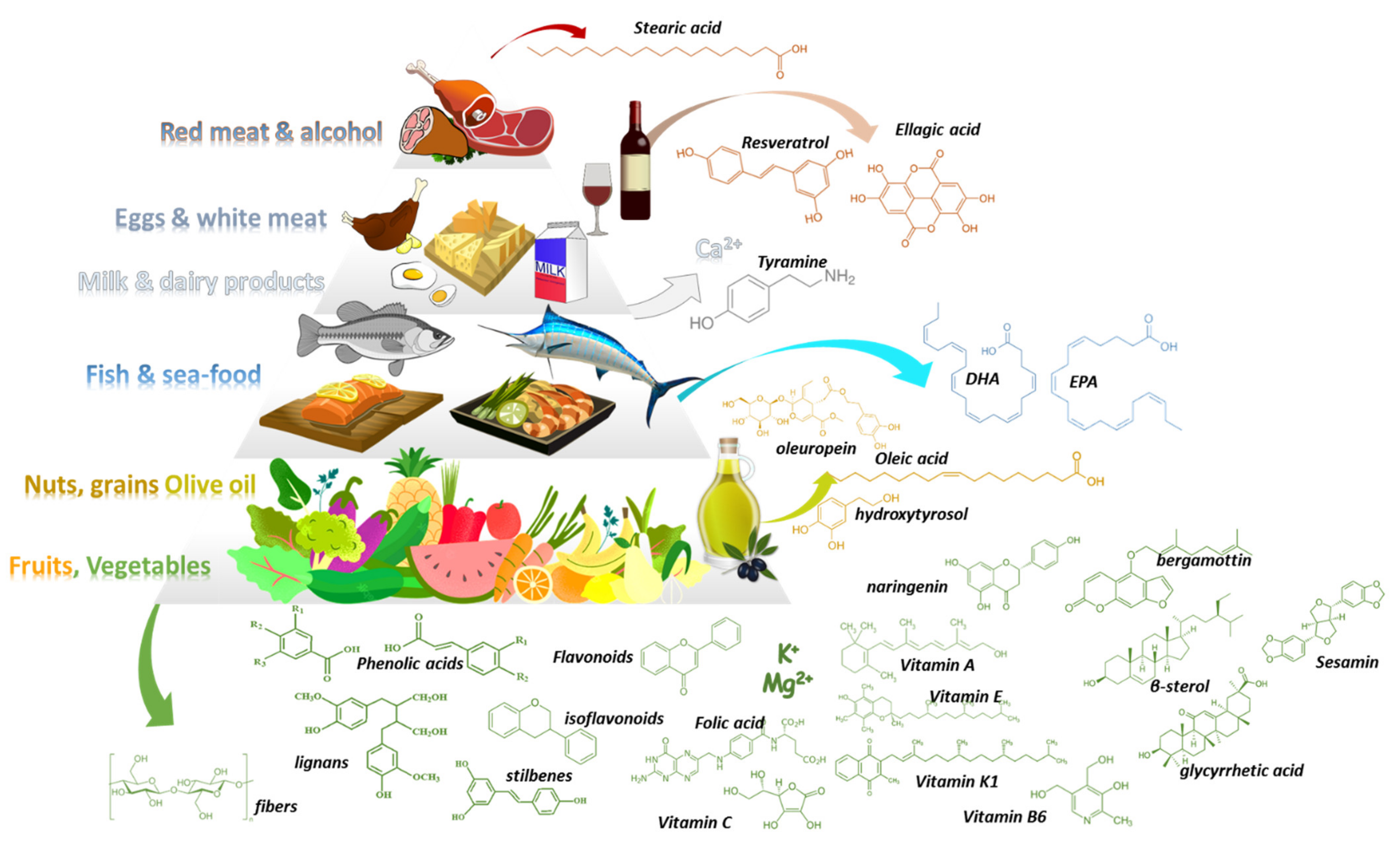
Med-D allows the intake of all types of foods following a general food guidance pyramid (
Figure 1)
[2][3][2,3]. In its base (level 1) are vegetables, fruits, nuts, and cereals that should be consumed in greater amounts and at daily frequency. Above them (level-2), sea food proteins and omega-3-fatty acids (n-3 FAs) are suggested to be consumed biweekly. Animal food products (level3) such as dairy, cheese, and eggs can be consumed in moderate portions during the week. Red meat (level 4) should be consumed in less proportions during the week along with saturated fat products and sweets. Regarding alcohol, a moderate consumption of wine and other fermented beverages is recommended (one to two glasses with meals). The pyramid is complete considering daily activities and physical exercise.
Table 1,
Table 2 and
Table 3 summarize available data regarding potential DFIs for food products of level1 in the Med-D pyramid.
Figure 1.
The Mediterranean diet pyramid along with examples of characteristic constituents that can be found in Med-D’s food products.
Table 1. DFIs, pharmacological mechanism, significance, and level of evidence for vegetables and herbs that are contained in the base of Med-D pyramid (PK: pharmacokinetic, PD: Pharmacodynamic, DFI: drug-food interaction).