Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Stefan Harsanyi and Version 2 by Conner Chen.
In modern society, there has been a rising trend of depression and anxiety. This trend heavily impacts the population’s mental health and thus contributes significantly to morbidity and, in the worst case, to suicides. Modern medicine, with many antidepressants and anxiolytics at hand, is still unable to achieve remission in many patients. The pathophysiology of depression and anxiety is still only marginally understood, which encouraged researchers to focus on neuropeptides, as they are a vast group of signaling molecules in the nervous system. Neuropeptides are involved in the regulation of many physiological functions
- anxiety
- depression
- neuropeptides
1. Neuropeptides in Anxiety and Depression
Neuropeptides are small polypeptides of size ranging from 3 to 100 amino acids. Secretion is localized in neurons and the effect, depending on receptors, is local or distant. Affected are both neurons and other somatic cells, indicating a wide array of effects [1][2][19,20]. Some are synthesized as precursors and later cleaved into mature forms, while some have no post-translational changes [3][21]. Stress, pain, or emotional distress often leads to anxiety and depression. Studies of neuropeptides and their related receptors pose a high potential for a better understanding of the etiology/etiopathogenesis of these disorders, leading to better, more targeted surveillance and treatment, especially as diagnostic markers. In Table 1 , we summarize the neuropeptides mentioned in theise contents article with their related receptors and encoding genes. Data were acquired using the OMIM® database accessed on 25 May 2022 [4][22].
Table 1. Anxiety and depression-related neuropeptides, encoding genes, and related receptors. (Receptors of neuropeptides without any relation to anxiety or depression are not mentioned in this table.)
| Neuropeptide | Gene (Symbol) | Cytogenetic Location | Related Receptors |
|---|---|---|---|
| Oxytocin | OXYTOCIN (OXT) | 20p13 | OXTR |
| Vasopressin | ARGININE VASOPRESSIN (AVP) | 20p13 | AVPR1A; AVPR1B; AVPR2 |
| Adrenocorticotropic hormone | PROOPIOMELANOCORTIN (POMC) | 2q23.3 | MCR1; MCR2; MCR3; MCR4; MCR5 |
| Corticotropin-releasing hormone | CORTICOTROPIN-RELEASING HORMONE (CRH) | 8q13.1 | CRHR1; CRHR2 |
| Urocortin 1 | UROCORTIN (UCN) | 2p23.3 | |
| Urocortin 2 | UROCORTIN II (UCN2) | 3p21.31 | |
| Urocortin 3 | UROCORTIN III (UCN3) | 10p15.1 | |
| Pituitary adenylate cyclase-activating polypeptide | ADENYLATE CYCLASE-ACTIVATING POLYPEPTIDE 1 (ADCYAP1) |
18p11.32 | ADCYAP1R1; VIPR1 |
| Melanocyte stimulating hormone | PROOPIOMELANOCORTIN (POMC) | 2p23.3 | MC3R; MC4R |
| Melanin-concentrating hormone | PRO-MELANIN-CONCENTRATING HORMONE (PMCH) |
12q23.2 | MCH-R1; MCH-R2 |
| Beta-endorphin | PROOPIOMELANOCORTIN (POMC) | 2q23.3 | OPRM1 other μ-opioid receptors |
| Neuropeptide Y | NEUROPEPTIDE Y (NPY) | 7p15.3 | NPY1R; NPY2R; NPY5R |
| Neuropeptide S | NEUROPEPTIDE S (NPS) | 10q26.2 | NPSR1 |
| Neuropeptide FF | NEUROPEPTIDE FF-AMIDE PEPTIDE (NPFF) | 12q13.13 | NPFFR1; NPFFR2 |
| Galanin | GALANIN (GAL) | 11q13.2 | GALR1; GALR2; GALR3; GPR151 |
| Galanin-like peptide | GALANIN-LIKE PEPTIDE (GALP) | 19q13.43 | GALR1; GALR2 |
| Spexin | SPEXIN HORMONE (SPX) | 12p12.1 | GALR2; GALR3 |
| Kisspeptin | KISS1 METASTASIS SUPPRESSOR (KISS1) |
1q32.1 | KISS1R |
| Substance P | TACHYKININ 1 (TAC1) | 7q21.3 | TACR1; TACR2; TACR3 |
| Neurotensin | NEUROTENSIN (NTS) | 12q21.31 | NTSR1; NTSR2 |
| Hypocretin | HYPOCRETIN (HCRT) | 17q21.2 | HCRTR1; HCRTR2 |
| Phoenixin | SMALL INTEGRAL MEMBRANE PROTEIN-20 (SMIM20) | 4p15.2 | GPR17 |
| Relaxin 3 | RELAXIN 3 (RLN3) | 19p13.12 | RXFP3 |
| Nesfatin-1 | NUCLEOBINDIN 2 (NUCB2) | 11p15.1 | Not discovered |
| Nociceptin | PREPRONOCICEPTIN (PNOC) | 8p21.1 | OPRL-1 |
| Cholecystokinin | CHOLECYSTOKININ (CCK) | 3p22.1 | CCKAR; CCKBR |
| Calcitonin gene-related peptide | CGRP RECEPTOR COMPONENT (CGRP) | 7q11.21 | CGRPR |
| Neurokinin A | TACHYKININ 1 (TAC1) | 7q21.3 | TACR1; TACR2; TACR3 |
Signaling axes (or pathways) studied in relation to anxiety and depression are the hypothalamic–pituitary–adrenal (HPA) axis, the hypothalamic–pituitary–gonadal (HPG) axis, and the gut–brain axis (GBA). The GBA is newer, and less thoroughly studied, although reports indicate that the microbiome and gut hormones may play a role in the etiology of depression [5][23]. More studied are the HPA and HPG axes. Interactions of these axes are presented in Figure 12.
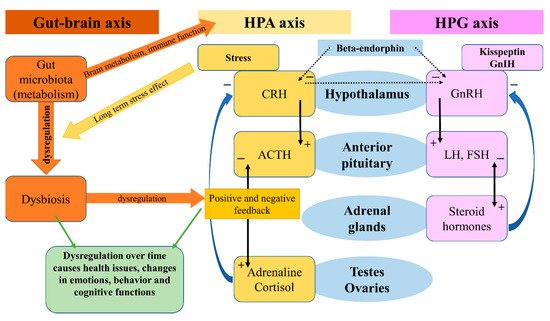
Figure 12.
Gut-brain axis, HPA axis, HPG axis and their interactions.
The HPA axis affects many different systems in the mammalian body, with a modern link to neuropeptides, psychiatry, and neurology, one reviewwhich we will focus oin this aspect [6]review [24]. The HPA axis is controlled by the limbic system depending on stimuli (stressors) received by the latter, and so inducing release of the CRH. CRH stimulates the release of ACTH (adrenocorticotropic hormone), which affects the adrenal glands and the production of glucocorticoids. Stress-adaptation responses are mediated by corticosterone in rodents and by cortisol in humans.
Circulating levels of gluco- and mineralo-corticoids are essential for negative feedback on the hypothalamus, which has been reported faulty in patients suffering from depression [7][25]. A systematic review and meta-analysis on the effects of aging and the HPA axis in patients with depression reported that older patients suffering from depression showed a higher degree of dysregulation in the HPA axis [8][26]. A bipolar disorder- (BD) focused systematic review and meta-analysis found a possible association of progressive HPA axis dysfunction with the cognitive deterioration of BD patients, which seemed rather a risk factor than a determinant, but nonetheless an important one [9][27]. In a recent review, an association between early-life stress in the HPA axis and anxiety has been found, followed by hyperactivity in the axis acting as a risk factor for relapses [10][28]. Effects of the microbiota on the HPA axis, stress response, anxiety-like behavior, endocrine abnormalities, and wider neuropsychiatric disorders have been observed, calling for further investigation [11][12][13][14][29,30,31,32]. In a systematic review, Juruena et al., based on the activity of the HPA axis, found a difference between melancholic and atypical depressive subtypes [15][33]. However, they attributed these findings to hypercortisolism in melancholia and rather normal, than decreased, function in atypical depression [15][33].
The HPG axis is represented by neurons of the gonadotropin-releasing hormone (GnRH), which in mammals is a 10-amino acid peptide. GnRH stimulates the synthesis and secretion of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), thus having an important role in the regulation of fertility and reproduction. GnRH is inhibited by the gonadotropin-inhibitory hormone (GnIH), which belongs to the RFRP family. The RFRPs (RF-amide-related peptides) act in regulatory regard to the HPG axis [16][34]. Studies on the GnIH have been associated with different behaviors in male rats [17][35]. Stress-induced increase in adrenal glucocorticoids increased the RFRPs, which contributed to the suppression of reproductive function through the HPG axis [18][36]. In birds, a small dose of interfering RNA targeted against the GnIH precursor mRNA caused elevation in aggressive and sexual behaviors [19][37]. Iwasa et al. reviewed the field of stress-induced reproductive dysfunction and found an association with the GnIH/RFRP-3 system [20][38]. These findings are important as stress, whether physical or emotional, is related to anxiety and depression in a reciprocal character, and one may affect or over time induce the other. The use of GnRH analogs caused upregulation in the expression of phoenixin in hypothalamic, hypophyseal, and ovarian regions, while the GPR173 expressions were downregulated in the hypothalamus and pituitary [21][39].
2. Oxytocin
Oxytocin (OXT) is composed of nine amino acids and was the first polypeptide hormone to be sequenced. OXT is synthesized in the supraoptic and paraventricular nuclei of the hypothalamus [22][40]. It became first known for its role in lactation, parturition, and maternal behavior, yet over the last several decades it has also been implicated in memory, regulation of anxiety, mood, and social behavior [23][41]. In reaction to acute stress, oxytocin is released from the nucleus centralis of the amygdala, which leads to the local activation of gamma-aminobutyric acid (GABA)-ergic interneurons [24][42]. While the amygdala is responsible for acute stress reactions, stria terminalis is the structure involved in the transition to chronic anxious states. A portion of oxytocinergic neurons from the periventricular nucleus projects directly into this structure [25][43]. The anterior cingulate cortex likely facilitates learning and social adaptation [26][27][44,45]. Oxytocin receptors (OXTR) are present across the whole brain, and it seems that the research of polymorphisms and epigenetic markers for OXTR is a promising area for future research [28][46]. Myers et al. reported two single nucleotide polymorphisms (SNP) in the OXTR gene in depressed patients [23][41]. Costa et al. described a relationship between separation anxiety in adulthood and SNP rs53576 of the third intron of the OXTR gene, which seems of substance for the epigenetic regulation of this gene [29][47]. An allele of rs53576 is also related to increased suicide risk, according to some authors [30][48]. Oxytocin interacts with various neurotransmitters and neuroendocrine systems [31][49]. The most prominent ones are the serotonergic and GABA-ergic systems and the HPA axis. Mottolese et al. have proven the interplay between oxytocin and serotonin using a 5-HT1A receptor antagonist 2’methoxyphenyl-fluorobenzamidoethylpiperazine (MPFF). Intranasal administration of oxytocin resulted in increased levels of MPPF in nucleus dorsalis raphes, the right amygdala-hippocampus-parahippocampus complex, insula, and right medioventral prefrontal cortex, measured using PET MRI [32][50]. The interplay between the oxytocinergic and serotoninergic systems is further supported by the fact that MDMA (3,4-methylenedioxymethamphetamine) causes oxytocin-mediated behavioral changes via serotoninergic 5HT1A receptors [33][51]. Furthermore, oxytocin is also connected to the HPA axis. Part of the neurons in the paraventricular nucleus co-expresses oxytocin and CRH, a portion of CRH-releasing neurons expresses mRNA for the OXTR, and clusters of OXTR express CRH receptor CRHR2. Centrally administered oxytocin reduces the excitability of CRH neurons, inhibits their spontaneous excitability, and lowers the expression of CRH mRNA and neuroendocrine response to stress [24][42]. In animals, the central administration of oxytocin reduces anxiety-like behaviors and lowers plasmatic cortisol levels [34][52]. Furthermore, the medial prefrontal cortex contains oxytocinergic interneurons synthetizing CRH binding protein (CRHBP) and GABA. In male rodents, the stimulation of these interneurons leads to the release of CRHBP and the reduction of CRH activity and anxiety, while in female rodents CRHBP was not able to effectively inhibit CRH activity, which may be due to higher levels of CRH in paraventricular nuclei (PVN) [35][53]. Antagonistic activity on GABAA receptors in the PVN blocks the suppression of stress-induced CRH release and the application of oxytocin into the PVN results in a significant increase in GABA release from the PVN [34][52]. Meisenberg was the first to describe the antidepressant-like effect of oxytocin when oxytocin application had an effect similar to the tricyclic antidepressant imipramine in rodents—it resulted in reduced immobility during the forced swim test [33][51]. Later, Scantamburlo et al. reported an inverse relationship between plasma oxytocin levels and the severity of symptoms of depression and anxiety in depressed patients [36][54]. Jobst et al. measured plasmatic levels of oxytocin in chronically depressed patients before and after psychotherapy. In their research, increased levels of oxytocin correlated with a reduction of subjectively reported depressive symptoms according to the Beck Depression Inventory-II [37][55]. Lancaster et al. found that higher endogenous oxytocin levels are associated with a reduced central amygdala volume and blood oxygen level-dependent activity in response to aversive stimuli [38][56]. However, the relationship between oxytocin and depressive and anxiety symptoms is not as straightforward as it may seem, and the literature is full of contradictory results. For example, Parker et al. found increased oxytocin levels in depressed subjects, and more recently Tabak et al., examining the role of oxytocin in social anxiety in humans, reported increased plasma concentrations of oxytocin following the Trier Social Stress Test (TSST), but this increase was specific to women, and that social anxiety moderated the OXT increase with more socially anxious participants showing greater increases than those with lower levels of social anxiety [39][57]. This can be the result of the so-called oxytocin paradox, which has been described as the context-dependent feedback loop of OXT signaling based on socio-psychological settings leading to positive or adverse psychological consequences [40][58]. The functioning of oxytocin varies according to contextual factors and individual differences, including gender, age, and psychosocial functioning [41][59]. In the past years, research allowed peopleus to better understand signaling ways affected by OXT and its complex regulation, and further multi-peptide-centered research will reveal this intricate web of regulation.
3. Vasopressin
Vasopressin, also known as the antidiuretic hormone (ADH) or arginine vasopressin (AVP), consists of 9 amino acids, belongs to nonapeptides, and is synthesized by magnocellular cells of the hypothalamic supraoptic nucleus and PVN whose axons project to the posterior pituitary [42][43][60,61]. After release into the bloodstream, it is transported predominantly to kidneys and blood vessels, where it regulates physiological functions (e.g., resorption of water, vasoconstriction, …). Vasopressin has amino acid sequences and tertiary structures similar to oxytocin, probably due to the shared origin of their encoding genes [44][62]. In addition, it is possible that an interplay between oxytocin and vasopressin is involved in mood and stress-response regulation [45][63]. It binds to four types of G-protein-coupled receptors: AVPR1A, AVPR1B, AVPR2 (for clarity reasons further as V1A, V1B, and V2, respectively), and oxytocin receptor [46][64]. V2 receptor binds to vasopressin in the kidney, where it participates in water homeostasis [47][65]. On the other hand, V1B and V1A receptor subtypes are promising sites of interest for psychiatry. The V1B subtype is highly expressed in the anterior pituitary gland, where it stimulates corticotropin release and is also localized in the amygdala, hippocampus, and hypothalamus [48][66]. Purba et al. already in 1996 reported increased numbers of V1B receptors in the postmortem analysis of brains of depressed patients compared to controls [49][67]. In depression and anxiety, vasopressin binds to V1 receptors in the brain. Hoghson et al. used V1B-30N-A potent V1B receptor antagonist in rat pups to examine the potential role of V1B in anxiety. They reported that V1B-30N had a dose-dependent anxiolytic effect in the separation-induced vocalization test in rat pups, moreover without causing sedation [46][64]. The interaction between vasopressin and oxytocin has already been mentioned, but vasopressin co-operates at least with one other neuromodulator system—the serotonergic. Ishizuka et al. used V1B knockout mice treated with a selective serotonin reuptake inhibitor (SSRI) and serotonin noradrenaline reuptake inhibitor (SNRI) to examine whether at least part of the SSRI´s effects might be mediated via the V1B receptor. The effects were evaluated in experiments using an elevated plus-maze (EPM) test and a hole-board (HB) test. Chronic treatment of V1bR KO mice with SSRI did not change the amount of time spent on the open arms, the number of head dips, or the number of readings, while chronic treatment with SNRI significantly increased the time spent on the open arms and the number of head dips. These results suggest that the anxiety action of 5-HT reuptake inhibitors might partly involve V1bR regulating the anxiety behaviors [48][66]. While the V1B receptor likely plays a role in depression and anxiety, the V1A subtype seems to be related to a different type of psychopathology. Vollegbregt et al. in their study reported an association between RS3 microsatellite repeats within the promoter region of the V1A gene and extreme childhood aggression, while no association was found between childhood aggression and RS1 repeats [50][68]. However, in addition to factors related to the V1 receptor, the levels of vasopressin also likely play a role in the pathophysiology of depression and anxiety. It was shown that chronically elevated plasma vasopressin levels may induce depressive symptomatology [51][69]. Another research project pointing to the positive correlation between vasopressin levels and depression was performed by Mlynarik et al., which showed reduced depression-like behavior in vasopressin-deficient Battleboro rats during the forced swim test [52][70]. The results of human studies agree with animal research. Goekoop et al. measured plasma levels of vasopressin in 89 patients with a highly anxious-retarded subtype of depression with a family history of depression. Depression with above-normal plasma AVP, as well as familial depression with above-normal plasma AVP, showed a high correlation between anxiety and retardation and this correlation was significantly higher than that found in the depressed patient control groups. The data support the delimitation of a largely familial depression with above-normal plasma AVP, vasopressinergic activation of the HPA axis, and a variable anxious-retarded phenotype [53][71]. As already mentioned above, the current situation regarding the efficient treatment of anxiety and depression is far from satisfactory despite the fact that there are multiple pharmacological agents on the market. The rate at which novel antidepressants are developed and introduced into clinical practice is very slow. This motivates research into different treatment modalities, of which V1B antagonists seem to be one promising option [54][55][72,73].
4. Melanocortins
Melanocortins are a group of peptide hormones derived from pro-opiomelanocortin (POMC). This group includes the adrenocorticotropic hormone (ACTH), alfa-, beta-, and gamma-melanocyte stimulating hormones (MSH), beta-endorphin, and corticotropin-like intermediate peptide (CLIP), the adrenocorticotropic hormone fragment [56][74]. Melanocortin receptors are associated with obesity, erectile dysfunction, cachexia, pain, depression, and anxiety [57][75]. Melanocortins work through the melanocortin receptors. The five melanocortin receptors are GPCRs identified as MC1 to five receptors. To date, only MC3R and MC4R with their ligand, the alfa-MSH (also gamma-MSH in the case of MC3R) were connected to anxiety and depression [58][76]. The main expression sites of melanocortin neurons are located in the brainstem and the hypothalamus, in the arcuate nucleus (ARC), closely communicating with AgRP- and Neuropeptide Y- (NPY) expressing neurons, thus indicating their participation in the system [59][60][77,78]. The alpha-MSH was reported to suppress the effects of NPY, thus reducing its antidepressant effect [61][79]. The administration of alpha-MSH antagonist with NPY shows a synergistic anxiolytic effect [62][80]. The inhibition of MC4 receptors in the dorsal raphe nucleus (DRN) using alpha-MSH induces anxiety and depression and reduces feeding in mice [63][81]. PVN, ARC, and DRN are predominant locations of the alpha-MSH effect [64][82]. The circle of regulation in the melanocortin system is closed by the receptor antagonist, the Agouti-related peptide (AgRP), with an orexigenic effect [65][83]. Chronic administration of a high-fat diet blunts AgRP response to anxiety and depression signals, as well as hunger by reducing GABA-ergic outputs from AgRP aimed at MC4R. However, GABA-ergic stimulation and suppression of the 5-HT3R within the MC4R neurons in the bed nucleus causes cessation of the effect of the high-fat diet-induced anxiety and depression [66][84]. The combined effect also reduces food intake and thus body weight. These findings indicate that initially AgRP regulates appetite, but later with a loss of effect, MC4Rs are a viable option for further research on anxiety and depression treatment [67][68][85,86]. Further associations are discussed in individual sections. A specific regulation protein, which affects the melanocortin system, is the melanocyte-stimulating hormone release-inhibiting factor-1 (MIF-1) with its analog Nemifitide. Both show low affinity to μ-opioid receptors and function as blockers of alpha-MSH release, thus reducing its inhibitory effect on NPY. Preclinical studies have shown effects in depressive disorder, but further research into this particular peptide is necessary to prove its efficacy.
5. Corticotropin-Releasing Hormone
Corticotropin-releasing hormone (CRH) is also known as the corticotropin-releasing factor (CRF); however, for precise nomenclature reasons, further on, the term CRH will be used. CRH is the central regulator of the hypothalamic–pituitary–adrenal (HPA) axis, which is the main organizer of the body’s response to stress. CRH consists of 41 amino acids and binds to CRHR1 and CRHR2, two GPCRs (not counting alpha and beta splicing variants), both in the central nervous system and the R2 also in peripheral tissues [69][87]. CHR receptors are expressed in the pituitary, amygdala, hippocampus, brain stem, and cingulate cortex (20). The CRH system consists of CRH itself, then Urocortin 1, 2, and 3, which all serve as ligands for the CRH receptors [70][88]. Effects of this system lie not only in the mediation of stress-related responses but also in the regulation of inflammation, with a close relationship with inflammation-related pain, as macrophages, monocytes, or mast cells do express both CRH receptors, thus serving as targets of this system [71][89]. CRH-induced stress-related responses through the HPA axis have a wide area of effect, recently measured in human hair follicles connected to hair loss interestingly antagonizable by caffeine [72][90]. ItHere we can be observed how deteriorative an effect the CRH-HPA system can have on the human body and how broad the effect is. It is not surprising that many human and animal studies report CRHs’ effect on the HPA axis regulation. Chronic stress activates the CRH-related signaling in the bed nucleus and induces maladaptive behavior in mice [73][91]. This goes in line with observed HPA axis dysfunction in patients with major depression or schizophrenia, where the continuous effect of CRH on the HPA axis causes disbalance (increased cortisol, increased ACTH, reduced feedback) and results in a pathology [74][75][92,93]. This disbalance is targeted by antidepressants, which after a period of time have the potential to revert changes in HPA axis hyperactivation. The CRH system is long associated with serotonergic mediation, emotional disbalance, behavioral changes, anxiety, and depression [76][77][78][94,95,96]. CRHR1 gene variants have been linked to a higher susceptibility to depression or panic disorder [79][80][97,98]. A sex-specific stress reaction in females has been observed in an animal model, with sex hormones affecting CRH regulation [81][99]. Transgenic mice with induced CRH expression show hyperactivation of the HPA axis and an increase in stress-mediated processes and behaviors, treatable with CRHR1 antagonists [82][100].
Further members of the CRH family are the urocortins. Urocortin 1, 2, and 3 are a group of three peptides (UCN1, UCN2, and UCN3). UCN1 is a 40-amino acid peptide, while UCN2 and 3 are paralogous 38-amino acid peptides that bind to CRHR2 [83][101]. UCN1 is produced by the hypothalamus, substantia nigra, and the pituitary gland and has a high affinity for both CRH receptors, suggesting its role in behavior and interestingly also regulation of food intake [84][102]. The intracerebrovascular injection of UCN1 has anxiogenic and “anti-social” effects antagonizable by CRHR1 antagonists [85][86][103,104]. However, the CRHR1 antagonist had no effects on social interaction on its own but antagonized the decreases in social interaction induced by stress or UCN1 [87][105]. Summarized by Tanaka et al., UCN2 and UCN3 show an association with depression-like behavior, where stimulation by UCN1 (CRHR1-2) is antagonized by UCN2 and UCN3 (CRHR2), thus resulting in no effect [88][106].
The latest members associated with the CRH family are four teneurins, or teneurin C-terminal associated peptides (TACPs), which share homology with the amino acid sequence of CRH and bind to latrophilins (a group of highly conserved GPCRs). Their effect is tissue-specific, and reports show an ability of TACP-1 to reduce anxiety, addiction, and depression in stress-induced behaviors [89][107].
On the other hand, studies and preclinical models also show mixed results [90][108]. In some cases, CRH or TACP receptor antagonists have different effects on anxiety, based on the animal test line, the baseline of depression, or perceived anxiety or the treatment regimen, but also depending on the test, as these therapeutics do not work under basal conditions. However, if depression- or anxiety-related symptoms or signaling are present, these therapeutics do have a significant effect [91][109]. In other words, a stressor (depression or anxiety) must be present for antidepressants and anxiolytics to work [92][110]. These conclusions are not surprising, as urocortins and their over-expression in CRH-deficient individuals are often induced as a compensatory mechanism in absence of CRH. The same result is for models with CRH over-expression antagonizable by CRHR1 antagonists, where some lines do exhibit higher anxiety and vulnerability to stress, but in other lines that do not exhibit these traits, a UCN1 downregulation was found [93][94][111,112].
6. Pituitary Adenylate Cyclase-Activating Peptide
Pituitary adenylate cyclase-activating peptide (PACAP) is a neuropeptide existing in two isoforms, either 27 or 38 amino acids long. PACAP is relatively well-conserved across many species [95][113]. Wide expression in central and peripheral tissues indicates a role in multiple physiological functions, such as the modulation of nociception, regulation of prolactin release, and food intake, along with stress, anxiety, and depression [96][97][114,115]. PACAP has the highest affinity for the ADCYAP1R1 receptor, known also as the PAC1 receptor [98][116]. Studies have associated this neuropeptide with stress-related mood disorders and adaptation [1][99][19,117]. PASAP is predominately expressed in the amygdala and the bed nucleus [100][101][118,119]. Dore et al. observed pro-depressive and anxiety-like effects on rats after intracerebroventricular PACAP administration [102][120]. Human studies show an association of PACAP/PAC1 receptor with behavioral and endocrine responses, also in neuropsychiatric disorders such as schizophrenia or post-traumatic stress disorder (PTSD) [103][104][105][121,122,123]. A recent animal model of PACAP-mutated mice under chronic variable mild stress exhibited viable results for future depression-targeted tests [106][124]. PACAP-KO mice exhibit decreased c-Fos expression, which shows a close connection not only with CRH and wider melanocortin signaling [107][108][125,126]. These results go in line with previous results on PACAP’s influence on CRH [109][127]. Additionally, a study on the consequences of chronic stress on PACAP expression in the bed nucleus goes in hand with CRH, indicating that synergic modulation exists in anxiety-like behavior [110][128]. The anxiety-associated effect of PACAP was further studied in mice, where the induction of PACAP-firing neurons aimed at the bed nucleus enhanced anxiety-like behavior [111][129].