1. Introduction
Glutathione is a tripeptide (cysteine, glycine, and glutamic acid) found in relatively high concentrations in many bodily tissues
[1]. It plays a pivotal role in reducing oxidative stress, maintaining redox balance, enhancing metabolic detoxification, and regulating the immune system
[1]. Various chronic, age-related diseases such as those related to neurodegeneration, mitochondrial dysfunction, and even cancer, have been related to suboptimal or deficient glutathione levels
[1][2][3][1,2,3]. There is increasing awareness of its utility in mitigating body toxin load through its ability to enhance hepatic conversion and excretion of compounds such as mercury and persistent organic pollutants (POPs)
[1][4][5][1,4,5].
As a result, it is possible that supporting the body’s endogenous levels of glutathione would be important for maintaining health and mitigating disease, although clear causal relationships between low glutathione and disease risk remain to be determined. One confounding factor is the complexity of antioxidants, referred to by Halliwell
[6] as the “antioxidant paradox”, or the situation in which antioxidants such as glutathione can possess prooxidant activity causing a hormetic effect enabling the body to bolster its endogenous antioxidant defenses. Indeed, redox balance can be the cause or consequence of a disease, and in some cases, it is difficult to know the level at which an antioxidant becomes a prooxidant. Therefore, there is much to understand about the role of glutathione levels in health.
A factor influencing glutathione status is the degree of variability in an individual’s capacity to produce glutathione, mainly due to genetic variability in enzymes involved in its production and/or regeneration. The enzymes that have received increased attention in the scientific literature and within clinical medicine include glutathione-S-transferase and gamma-glutamyl transferase. Some of these enzymes require nutrient cofactors
[1] (
Figure 1). With upregulated oxidative stress, malnutrition or increased toxic burden due to exposure to environmental contaminants, there can be even greater need for glutathione
[7][8][9][7,8,9]. A list of some proposed disease states related to inadequate glutathione status are listed in
Table 1.
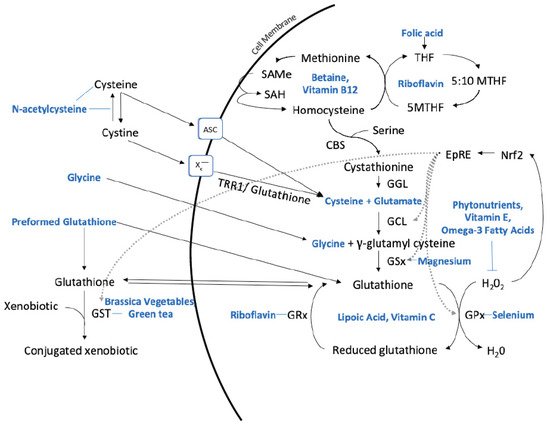
Figure 1. Hepatic synthesis of glutathione and nutritional substrates, co-factors, and other nutrients that influence metabolism. Key: 5-Methyl-tetrahydrofolate (5MTHF), system alanine–serine–cysteine (ASC), cystathionine-β-synthase (CBS), cystathionine gamma-lyase (CGL), electrophile response element (EpRE), glutathione-S-transferase (GST), glutamate cysteine ligase (GCL), glutathione reductase (GRx), glutathione peroxidase (GPx), glutathione synthetase (GSx), hydrogen peroxide (H
2O
2), Nuclear factor erythroid factor-2-related factor 2 (Nrf2), S-adenosylmethionine (SAMe), S-adenosylhomocysteine (SAH), tetrahydrofolate (THF), thioredoxin reductase 1 (TRR1), water (H
2O), cystine/glutamate antiporter system (x
c−). Description: Folic acid is reduced to THF and converted to 5MTHF which can subsequently be transferred to homocysteine and generate methionine. Methionine forms SAMe, which produces SAH from methylation reactions. SAH is hydrolyzed to homocysteine. Homocysteine can either regenerate methionine or be directed to the trans-sulfuration pathway forming cystathionine via the catalytic activity of CBS and serine. CGL cleaves the sulfur–gamma carbon bond of cystathionine, resulting in the release of cysteine which can be used by GCL and GSx to form glutathione. Extracellular cysteine can be either taken up by the cysteine transporter ASC or oxidized to cystine and taken up by system x
c−. N-acetylcysteine can donate cysteine or reduce plasma cystine to cysteine. Intracellular cystine is reduced to cysteine via TRR1 or glutathione. The synthesis of γ-glutamyl cysteine is catalyzed by GCL from cysteine and glutamate, and the addition of glycine to γ-glutamyl cysteine via GSx generates glutathione. GPx catalyzes the reduction of H
2O
2 by glutathione and forms reduced glutathione which is then recycled to glutathione by GRx. Glutathione can also form adducts and conjugate xenobiotics via GST. Oxidative stress activates the Nrf2 pathway which induces EpRE-dependent gene expression of enzymes involved in glutathione metabolism, including GCL, GSx, GPx, and GST, to re-establish cellular redox homeostasis. Modified and developed from
[10][11][12][13][14][10,11,12,13,14].
Table 1.
Clinical conditions and diseases associated with glutathione.
|
Research has found that many chronic diseases are associated with a reduction in glutathione levels, leading to the hypothesis that increasing glutathione levels can help prevent and/or mitigate the progression of these diseases. Below is a list of some of the diseases [2] and issues associated with glutathione dysregulation or deficiency [3]:
|
|
• aging [15] and related disorders [3]
|
|
• Alzheimer’s disease [16]
|
|
• cancer [17]
|
|
• chronic liver disease [18]
|
|
• cognitive impairment [19]
|
|
• cystic fibrosis [20]
|
|
• diabetes [21], especially uncontrolled diabetes [22]
|
|
• human immunodeficiency virus (HIV)/ acquired immune deficiency syndrome (AIDS) [23]
|
|
• hypertension [24]
|
|
• infertility in both men and women [25]
|
|
• lupus [26]
|
|
• mental health disorders [27]
|
|
• multiple sclerosis [28]
|
|
• neurodegenerative disorders [29]
|
|
• Parkinson’s disease [30]
|
While there may be a need to repair low levels of glutathione, proper balance, rather than excess, is required. For example, glutathione may need monitoring in patients undergoing chemotherapy due to the potential to support chemoresistance
[17]. There are challenges in the use of glutathione as a diagnostic biomarker and therapeutic target. Red blood cell (RBC) glutathione is readily available as a clinical assessment but has been found to have wide intra-individual variation
[31]. However, this intra-individual variation is relatively stable over time which is a phenomenon likely due to variation in genes regulating glutathione levels in RBCs
[32].
2. The Role of Gene Deletions and Single Nucleotide Polymorphisms (SNPs)
There are some common single nucleotide polymorphisms (SNPs) that impact glutathione and associated processes and may subsequently influence disease risk. These code for the enzyme glutathione S-transferase (GST), which conjugate the reduced glutathione to substrates during the detoxification process
[33][34].
GSTP1 and
GSTM1 do have multiple SNPs (for example,
GSTP1 rs1695, A105G results in an amino acid substitution in codon 105 from valine to isoleucine associated with increased cancer risk), however, the null alleles described and focused on
in th
ere is review result from gene deletion between the H3 and H5 regions flanking the gene
[34][35]. During times of oxidative stress, GST genes are upregulated. One of the most common polymorphisms, affecting 20% to 50% of certain populations, is an absence of the
GSTM1 gene (
GSTM1-null), which decreases detoxification ability among other possible outcomes
[35][36].
GSTT1 (null) and
GSTP1 (AB/BB) are additional polymorphisms related to a reduction in GST activity
[36][37]. Having one or more of these polymorphisms is associated with an increased risk of certain diseases
[36][37], especially when impacted by environmental triggers such as pollution, smoking, heavy metals, and other toxins.
3. Optimizing Glutathione Production with Nutrients
Whether due to the presence of SNPs, gene deletions or heightened physiological need due to exogenous reasons like toxic load, to some extent, glutathione levels may be supported by dietary and/or supplemental nutrients. This review article will attempt to review the salient human clinical literature to support the use of specific foods and nutrients that may increase or maintain optimal glutathione levels.
4. Preformed Glutathione
It would seem to be most efficient to administer oral glutathione as a preformed compound to override the effects of potentially inefficient SNPs and related enzymes. However, there has been some debate regarding whether glutathione given orally would be degraded by digestive peptidases
[36][37][37,38]. In further support of this theory, some studies
[38][39][40][39,40,41] have shown no change in glutathione levels or in parameters of oxidative stress despite acute
[39][40][40,41] or chronic (four weeks)
[38][39] oral glutathione supplementation.
There is also some evidence to the contrary. One six-month, randomized, double-blinded, placebo-controlled trial
[41][42] found that taking oral glutathione at either 250 or 1000 mg/day led to significant increases in the body stores of glutathione in 54 non-smoking adults in a dose-dependent manner. There was also a decrease in the markers for oxidative stress at six months as indicated through an improvement in the oxidized (GSSG) to reduced (GSH) glutathione ratio in whole blood, in conjunction with favorable increases in natural killer cell cytotoxicity.
5. N-Acetylcysteine (NAC)
Three conditionally essential amino acids, glycine, cysteine, and glutamic acid combine to form glutathione in a two-step biochemical reaction. First, cysteine is conjoined with glutamate through the action of glutamate cysteine ligase to produce gamma-glutamylcysteine, which proceeds to link with glycine via glutathione synthase
[42][48]. Therefore, the human body requires all three amino acids and adequate enzymatic function to make sufficient quantities of glutathione
[43][44][49,50]. Cysteine is a sulfur amino acid, which might imply that consuming sulfur-rich foods, especially those containing the sulfur amino acids, may also support glutathione synthesis
[45][46][51,52].
Cysteine is frequently identified as rate-limiting, which provides the rationale of why N-acetylcysteine (NAC) is frequently studied and suggested as a supplement for glutathione support
[44][50], yet a review of the data indicates its use may be inconclusive or equivocal. A systematic review
[47][53] that included twelve clinical trials utilizing NAC supplementation with a specific focus on cognitive markers indicated that there may be some benefit to using NAC in certain populations; however, the studies were too variable in design and outcome to make any definitive conclusion. As a suggestion in future studies, including a genotype segmentation for participants for glutathione-related enzymes such as GST may lead to different findings and assist in investigating who is more primed for an effect.
6. Dietary Protein Considerations
Theoretically, impaired protein digestion may also be a limiting factor in ensuring healthy glutathione levels. A lack of or reduced hydrochloric acid production in the gastric mucosa and/or pancreatic enzyme insufficiency would be important to assess in a patient with low plasma albumin and low glutathione levels and/or symptoms of impaired glutathione activity (e.g., fatigue). Hypochlorhydria may, in fact, be more common in the aging population as the gut physiology changes
[48][64], and the use of certain medications can also impact hydrochloric acid levels
[49][65]. Further, oxidative stress (such as seen with low physiological glutathione levels)
[50][51][66,67] and certain nutrient deficiencies
[52][68] may also contribute to low stomach acid levels.
Since the precursors and foundation of glutathione are amino acids, intake of dietary protein may influence the amino acid pool from which to draw to synthesize glutathione. Changes in protein consumption
[53][69], including reducing protein levels but remaining within safe levels, may alter plasma glutathione synthesis levels contributing to a reduction in antioxidant capacity.
In Herethis study, the researchers found that while individuals were able to recover from a reduction in protein (that remained above the lowest amount considered safe) in terms of nitrogen balance, it took longer for the functional changes in glutathione levels to equilibrate. Urinary excretion of 5-L-oxoproline was suggested as a marker to track glutathione kinetics, particularly the availability of glycine.
7. Omega-3 Fatty Acids
Chronic inflammation can contribute to oxidative stress and deplete glutathione supply
[54][75]. Due to their involvement in the production of inflammatory and anti-inflammatory prostaglandins, omega-3 fatty acids have been studied for their effects on glutathione levels. In one study
[55][76] taking 4000 mg of omega-3 supplements daily for 12 weeks led to a better GSH–creatine ratio and reduced depressive symptoms in older adults who had a higher risk of developing depression compared with the control group taking a placebo. Another study in patients with Parkinson’s disease found that taking 1000 mg omega-3 fatty acids from flaxseed oil in conjunction with 400 IU of vitamin E for 12 weeks led to an increase in glutathione concentrations as well as total antioxidant capacity and a reduction in the inflammatory marker, high-sensitivity C-reactive protein, and markers of insulin metabolism
[56][77].
8. Vitamins
8.1. B Vitamins
Riboflavin is a necessary coenzyme for the activity of glutathione reductase, which converts the oxidized glutathione into its reduced form, the compound required for antioxidant function
[57][82]. While there is a paucity of studies to confirm that riboflavin deficiency negatively impacts glutathione levels, there is indication that homocysteine production and methylation processes require riboflavin
[58][59][83,84]. Since the methylation cycle is closely linked to that of the trans-sulfuration pathways and glutathione metabolism, riboflavin levels could be important. Thus, it is likely that a riboflavin deficiency would impact glutathione function and may even impact the levels in the body. From a biochemical perspective, pantothenic acid (vitamin B5) may also help support glutathione synthesis through its role in ATP production
[60][85]. B12 deficiency
[61][86] is associated with lower glutathione levels.
8.2. Vitamin C
In 48 individuals with ascorbate deficiency
[62][87], taking 500 or 1000 mg per day of vitamin C for 13 weeks led to an 18% increase in lymphocyte glutathione levels compared with placebo. Similarly, in healthy adults following a self-selected vitamin C-restricted diet
[63][88] and an initial week of placebo supplementation, taking 500 mg L-ascorbate per day for weeks two and three and 2000 mg per day for weeks four and five in a six-week trial led to an increased level of glutathione in red blood cells. The lower dose of 500 mg daily led to the most pronounced rise in glutathione levels.
8.3. Vitamin E
Vitamin E supplementation has been studied to a limited extent in diabetic populations subject to higher endogenous oxidative stress levels
[64][65][89,90]. In type 1 diabetic children
[66][91], vitamin E supplementation (DL-alpha-tocopherol, 100 IU oral daily dose) significantly increased glutathione by 9% and lowered lipid peroxidation (malondialdehyde) by 23% and HbA1c concentrations by 16% in erythrocytes. A similar study
[67][92] in 20 children with type 1 diabetes and 20 healthy controls found that 600 mg/day of vitamin E for three months improved oxidative stress markers and glutathione levels in the diabetic children. In adults (
n = 54) with diabetic neuropathy
[68][93], the group provided with a vitamin E supplement (800 IU/day) for 12 weeks had significant improvements in cardiometabolic parameters and plasma glutathione levels compared to the group given the placebo.
9. Other Nutrients
9.1. Alpha-Lipoic Acid
Alpha-lipoic acid is a multifunctional compound in its ability to serve as a direct scavenger of free radical species and to also help in the regeneration of endogenous antioxidants such as glutathione. A variety of clinical trials in diverse populations
[69][70][71][72][73][74][94,95,96,97,98,99] would suggest that alpha-lipoic acid could be important for restoring antioxidant capacity. Children with oxidative stress due to protein malnutrition where given either 600 mg reduced glutathione twice daily, 50 mg alpha-lipoic acid twice daily, or 100 mg NAC twice daily for 20 days
[75][100]. Glutathione and alpha-lipoic acid improved survival rates in these children, compared with the control group. HIV-infected adults (
n = 33) assigned to either 300 mg alpha-lipoic acid three times daily or placebo for six months resulted in elevated blood total glutathione and lymphocyte response in the therapeutic group relative to the control group
[76][101].
9.2. Selenium
Selenium is a known antioxidant and cofactor of glutathione peroxidase. In a mouse study
[77][102], selenium supplementation increased the expression and activity of certain glutathione-related enzymes. Another study
[78][103] in 336 healthy adults, (161 blacks, 175 whites) found a positive relationship between selenium levels and selenium supplementation. Despite similar selenium supplementation levels, glutathione levels increased to a greater extent in whites than blacks. It is worthwhile to note that excess selenium may contribute to oxidative stress rather than relieve it and this effect may be related to certain genotypes
[79][104].
9.3. Phytonutrients
There can be potentially mixed clinical results from supplementation with supraphysiological doses of antioxidant vitamins and minerals in isolation, separate from their phytonutrient counterparts. One disadvantage may involve disturbing the redox state of a cell towards a predominantly prooxidant status
[80][105]. Therefore, it might seem that one of the safer approaches to fortifying the innate defense against oxidative stress and improving glutathione levels may be best implemented through the diversity and pleiotropism of multiple phytonutrients. In support of this theory, fruit and vegetable intake has been shown to reduce oxidative stress
[81][106], even in intervention studies
[82][83][84][85][86][107,108,109,110,111]. There needs to be sustainable, creative ways for people to get their daily intake of fruits and vegetables as this quota is not being met by the vast majority
[87][112].
9.4. Brassica Vegetables
There is a plethora of research to suggest the detoxification and cancer preventative qualities of cruciferous vegetable intake
[88][89][122,123], especially for cancers related to the gastrointestinal tract
[90][124]. Studies
[91][92][125,126] have shown that administration of cruciferous-derived compounds, such as sulforaphane, may increase glutathione, glutathione-related enzymes, and even endogenous antioxidant enzymes and inflammatory markers, although results are not always consistent
[93][115]. These compounds may be especially important for individuals with GST polymorphisms.
9.5. Green Tea
Green tea consumption is associated with reduced rates of certain cancers such as leukemia
[94][134]. In a multicenter case–control study
[94][134] in China with 442 confirmed adult leukemia cases and 442 controls, green tea intake and GST genotypes were assessed. Researchers found not only an inverse association between drinking green tea and adult leukemia risk compared with those who did not drink tea, but that cancer risk reduction was more pronounced in those with the
GSTT1-null genotype than the
GSTT1-present carriers.
9.6. Juice Studies
For those for whom eating fruits and vegetables is challenging, drinking juice derived from these foods may provide another healthful option, although some health professionals might be concerned with their simple sugar content. Generally, clinical studies would suggest that drinking fruit and/or vegetable juices confer health benefits, such as improving antioxidant status
[95][96][97][98][136,137,138,139].
9.7. Herbs and Roots
While there is a lack in human clinical trial data, there are several animal studies which would indicate that certain herbs and roots, such as rosemary
[99][100][101][144,145,146], turmeric/curcumin
[102][147], milk thistle
[103][148], and
Gingko biloba [104][149], may influence glutathione levels. Rosemary extract in the diet of female rats at concentrations of 0.25% to 1.0% by weight resulted in a 3.5- to 4.5-fold increase in hepatic GST. An increase was seen when injected intraperitoneally but to a lesser extent
[100][145]. In an animal study, a turmeric extract and curcumin were shown to increase hepatic glutathione content
[105][150].
9.8. Plant Foods that Contain Glutathione
While the focus of this resviearchw has been on foods and dietary-derived nutrients for the purpose of supporting antioxidant defenses, primarily by increasing glutathione levels and enzymes related to glutathione’s activity, it is worthwhile to note that there are several foods that contain the thiol-rich compounds, glutathione, NAC, and cysteine. Eating a glutathione-supported diet could involve the inclusion of these foods daily, especially the green foods, asparagus, avocado, cucumber, green beans, and spinach.