1. Introduction
Coronavirus disease 2019 (COVID-19) is the clinical manifestation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
[1]. This infection started to spread across the world in 2019, increasing hospitalization rates in several countries, and rapidly turned into a global pandemic
[2]. Considering the high infection rate, which can affect an elevated percentage of individuals in each community in a short period, the mortality rate and the death risk estimation are related to the breakdown of the healthcare systems
[3][4][3,4]. Therefore, on March 2020, the World Health Organization (WHO) declared a pandemic, leading to the emergence of public health strategies to contain the outbreak, including social confinement and movement restriction
[2][5][2,5]. Reported illnesses have ranged from very mild (including some with no reported symptoms) to severe, including illness resulting in death
[4]. Despite the worldwide spread, the clinical and epidemiological patterns of COVID-19 remain unclear
[6]. The first epidemiological and clinical investigations showed that most COVID-19 cases were attributed to elder or middle- aged men, with a mean incubation period of 5.2 days
[7][8][7,8]. Aside from age and gender, there are also pre-existing conditions that are considered to be risk factors for SARS-CoV-2 infection, namely: hypertension, obesity, diabetes mellitus, asthma, chronic obstructive pulmonary disease, chronic kidney disease, smoking, and diseases that induce an immunosuppression state such as cancer
[9].
Cancer has a major impact on society, with more than 18 million new cases per year globally
[10]. Cancer patients are more susceptible to infection compared to healthy people and non-cancer patients
[11][12][11,12]. This predisposition has been historically related to the systemic malignancy-related immunosuppressive state and to active disease-oriented treatments, such as chemotherapy, immunotherapy, radiotherapy, and surgery
[13][14][13,14].
SARS-CoV-2 is a member of the Coronaviridae family and consists in an enveloped, single-stranded RNA virus with positive polarity and a genome of approximately 30 kilobases
[15]. Like an mRNA, the virus genome consists of a 5′ cap structure together with a 3′ poly (A) tail that translates its proteins. Coronaviridae viruses contain similar genomic RNA (gRNA) compositions, including two open reading frames (ORF1a and ORF1b), which encode for the RNA-dependent RNA polymerase (RdRp) and nonstructural proteins (nsps)
[16]. ORF1a contributes to the production of nsp1–nsp11, while the rest of the nsps (nsp12–nsp16) originate from ORF1b
[17]. In addition to this, one-third of the genome at the 3′ end encodes for the viral structural proteins’ surface (S), envelope (E), membrane (M), and nucleocapsid (N)
[17][18][17,18]. Moreover, the genomes of Coronaviridae viruses also contain multiple structurally conserved elements within the 5′ and 3′ untranslated regions (UTRs) that have been suggested to play roles in viral replication. These elements include three stem-loops (SL1, SL2 and SL3) within the 5′ UTR, as well as a bulged stem-loop (BSL), pseudoknot (PK) stem-loop, and hypervariable region (HVR) within the 3′ UTR. The spike glycoprotein of SARS-CoV-2 comprises the receptor binding domain (RBD) in the S1 subunit, which binds with the angiotensin-converting enzyme 2 (ACE2), allowing the penetration of the virus into the endothelial and epithelial cells and consequently activating infection
[19][20][19,20]. The S2 subunit improves the fusion of viral and host cell membranes that is activated by the transmembrane protease serine 2 (TMPRSS2)
[20]. Then, the virus affinity to infect certain cells may be related to the multiple organ distribution of ACE2, the functional receptor for SARS-CoV-2
[21]. Consequently, spike glycoprotein and its RBD are crucial targets for vaccination and therapeutic improvement
[22][23][22,23].
The global pandemic has caused an urgent necessity for vaccine development promoting the emergence of mRNA vaccines against SARS-CoV-2
[23][24][23,24]. These mRNA vaccines provide genetic information in the form of mRNA allowing the production of viral proteins by the host—more specifically the spike glycoproteins—to trigger an immune response
[23][25][23,25]. However, it is important to note that, in the same way that some subsets of the population are more prone to SARS-CoV-2 infection due to immunosuppression (either caused by cancer or other immune disorders), the same applies for their capacity of vaccination response. In fact, since cancer patients are not included in vaccination clinical trials, there is still a considerable uncertainty regarding the efficacy of the SARS-CoV-2 vaccines that are available, as well as the extent of the humoral and cellular immune responses and the impact of related side effects
[26]. In fact, cancer patients have a three-fold higher infection risk than the general population
[27]. Therefore, it is important to identify and study new potential biomarkers and therapeutic targets for this disease. Moreover, patients with lung or hematological cancers and those who receive active chemotherapy treatment are at a greater risk of SARS-CoV-2 infection, due to an increased immunosuppression state
[28]. In addition to an increased susceptibility to SARS-CoV-2 infection, the immunosuppressive state of cancer patients also makes them more prone to vaccination failure
[28]. However, due to the novelty of the mRNA vaccination field, the mechanisms behind vaccination responsiveness and immunity development are not fully understood. Therefore, it is important to identify and study new potential biomarkers that can predict and monitor these patients’ susceptibility to SARS-CoV-2 infection and responsiveness to vaccination.
Currently, there is a massive investment in circulating microRNAs (miRNAs) research, due to their potential use as biomarkers for innumerous conditions. The intensive research of the past few years has demonstrated that miRNAs are secreted in several of the body fluids (e.g., blood, plasma, serum, saliva, urine, etc.) that are routinely examined in patients; are stable and resistant to degradation; and are easy to quantify through molecular biology techniques such as real time PCR
[29][30][31][29,30,31]. This set of characteristics make miRNAs excellent biomarker candidates, with the advantage that they can be obtained through non-invasive or minimally invasive methods. MicroRNAs (miRNAs) are small non-coding RNAs of 18–25 nucleotides that play a key role in the regulation of gene expression through the post-transcriptional suppression of mRNAs
[32][33][32,33]. MiRNAs have been shown to regulate every aspect of cellular activity, including differentiation and development, metabolism, proliferation and apoptosis
[34]. In fact, they can regulate approximately 30–70% of human gene expression
[35]. These molecules can bind directly to mRNA targets by complementarity, causing their degradation or suppressing the translation process
[32]. Thousands of human protein coding genes are regulated by miRNAs, reinforcing the idea that miRNAs are master regulators of diverse biological processes with an impact in the body physiological responses
[34]. Over the past decade, it has been established that miRNAs expression is dysregulated in several human malignancies, consequently affecting the hallmarks of cancer and having either an oncogenic or tumour suppressor role
[36].
2. Evidence Synthesis
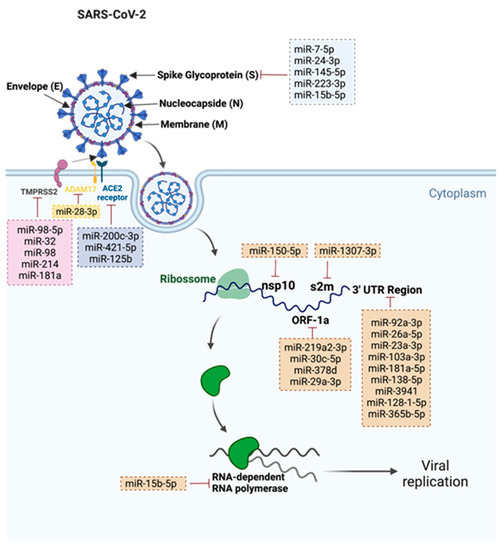
A total of 31 miRNAs were found. The gathered information is summarized in
Figure 1. The relevant miRNAs were divided into two categories: (1) miRNAs that target SARS-CoV-2 (2) miRNAs that target SARS-CoV-2 related proteins.
Figure 1. Representation of the 31 validated SARS-CoV-2 miRNAs and their respective targets. This figure was created at
BioRender.com (accessed on 12 July 2022).
2.1. miRNAs That Target SARS-CoV-2
3.1. miRNAs That Target SARS-CoV-2
RWe
searchers found a total of 22 human miRNAs that were involved in the targeting of several components of SARS-CoV-2, such as: 3′–untranslated regions (UTR); open reading frames (ORF); stem-loop II motif (s2m); and RNA template components of non-structural protein 10 (nsp10), spike protein, and RNA-dependent RNA polymerase (RdRp). Nine miRNAs were involved in the targeting conserved 3′–UTR of the viral genome. Park and colleagues observed that miR-92a-3p, miR-26a-5p, miR-23a-3p, miR-103a-3p and miR-181a-5p from placenta stem-cell-derived extracellular vesicles (EVs) were able to bind to 3′-UTR regions of SARS-CoV-2 and suppress RNA replication, consequently leading to the suppression of the virus-mediated pro-inflammatory response in human bronchial cells and lung fibroblasts
[37][45]. In addition to this, Barreda-Manso and co-workers described that miR-138-5p, miR-3941, miR-128-1-5p and miR-365b-5p were also able to bind to 3´-UTR regions of SARS-CoV-2
[38][46]. While some of the SARS-CoV-2 3′-UTR is variable in sequence, the virus contains a highly conserved 41-nucleotide (nt) stem-loop II motif (s2m) within the terminal portion of the HVR (hypervariable region)
[39][47]. Imperatore and colleagues highlighted the potential role of the s2m element in mediating the viral genome dimerization, suggesting its potential application as a drug target. Moreover, the authors observed that host miR-1307-3p was able to bind and inhibit s2m
[39][47]. Akula and co-workers observed that the decline in plasma levels of miR-150-5p in COVID-19 patients could enhance SARS-CoV-2 infection
[40][48]. In fact, these authors demonstrated that miR-150-5p was able to lower SARS-CoV-2 infection in vitro by targeting the coding strand of nsp10 and suggested that downregulation of this miRNA could be a mechanism to promote SARS-CoV-2 infection
[40][48]. Six miRNAs were involved in the targeting of the spike (S) protein. Wang and colleagues demonstrated that miR-7-5p, miR-24-3p, miR-145-5 and miR-223-3p were able to directly target the S protein and inhibit SARS-CoV-2 replication
[41][40]. Moreover, the authors also observed that these miRNAs were markedly decreased in elderly and diabetic patients when compared to young healthy volunteers
[41][40]. Siniscalchi and colleagues observed that endogenously expressed lung miRNAs were able to bind and inhibit viral targets. The authors observed that miR-219a2-3p, miR-30c-5p, miR-378d and miR-29a-3p were able to bind to ORF1a, and miR-15b-5p was able to bind to spike ORF and repress plasmid-driven spike expression
[42][49]. Moreover, these authors were also able to demonstrate that synthetic miRNA mimics of the miRNAs that were studied could be used to inhibit SARS-CoV-2, which highlights the potential of miRNAs as a therapeutic approach to fight the viral infection. In addition to spike ORF, miR-15b-5p was also described as being able to target the RNA template component of RdRp, further contributing to the suppression of viral infection and proliferation
[43][50].
3. MiRNAs Applications in Cancer Patients’ Management Regarding SARS-CoV-2
The use of circulating miRNAs as clinical biomarkers has been explored under a variety of conditions, including cancer and viral infections
[44][45][94,95]. MiRNAs are considered to be robust, sensitive, and cost-effective biomarkers that can add additional information to the clinical variables that are already used in the clinical practice
[46][47][58,96]. In fact, several miRNA-based diagnostic and therapeutic products are already in clinical trial phase and expected to enter the market in the next few years
[48][97]. Therefore, the study and use of miRNA profiles to stratify cancer patients according to their risk of SARS-CoV-2 infection and vaccination effectiveness seems a promising personalized approach to improve the current management of these patients (
Figure 23). Moreover, miRNAs can be obtained through minimally invasive methods, such as a blood sample, and their isolation and quantification protocols are simple and less time-consuming when compared with other type of molecules
[29][30][29,30]. In fact, the implementation of a stratification algorithm would allow the selection of patients that could benefit from the emerging SARS-CoV-2 therapeutic approaches, such as the Long-Acting Antibodies (LAAB) AZD7442, which are currently in phase III clinical trials (ClinicalTrials.Gov NCT04507256) and show promising results in reducing the risk of severe COVID-19 or death. LAABs mimic natural antibodies and can block the binding of the SARS-CoV-2 virus to host cells
[49][98]. Therefore, their potential is being tested to treat and prevent disease progression in patients that are already infected with the virus, as well as to be given as a preventative intervention prior to exposure to the virus.
Figure 23. Schematic representation of the applicability of using miRNA profiles to stratify cancer patients according to their prognostic in terms of SARS-CoV-2 infection risk and vaccination responsiveness. This figure was created at
BioRender.com. (accessed on 12 July 2022).