Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Ioannis Ntafoulis and Version 2 by Conner Chen.
Glioblastoma (GBM) remains one of the most difficult tumors to treat. The one of major obstacle in GBM treatment is the blood–brain barrier (BBB), which prevents effective delivery of drugs to the central nervous system (CNS). Another key player impeding drug delivery into the CNS is the family of drug efflux pumps and more specifically the ATP-binding cassette (ABC) transporters.
- drug repurposing
- glioblastoma
- blood–brain barrier
- efflux pumps
1. Introduction
Glioblastoma (GBM) is the most aggressive form of diffuse gliomas and the most lethal among all types of brain tumors, comprising 12–15% of all adult intracranial tumors and 50–60% of astrocytic neoplasms [1]. According to the 2021 WHO classification of central nervous system (CNS) tumors, former (grade 4) GBM is now classified based on the presence or absence of mutations in the isocitrate dehydrogenase (IDH) gene: IDH wild-type (IDHwt) glioblastoma or IDH-mutant (IDHmut) grade 4 astrocytoma [2]. Molecularly, IDHwt glioblastomas are characterized by the presence of TERT promoter mutation, EGRF amplification, +7/−10 chromosome copy number changes or any combination of the above [2]. IDHmut grade 4 astrocytomas are characterized by mutations of IDH1/2, ATRX, TP53, CDKN2A/B homozygous deletion, PDGFRA amplification or any combination of the above [2]. These genomic alterations of IDHwt gliomas are associated with fast growth rates and poor prognosis [2].
The standard of care treatment following diagnosis comprises maximal safe surgical resection of the tumor (debulking), followed by radiation therapy (RT) and concurrent and adjuvant chemotherapy with the alkylating agent temozolomide (TMZ) [3][4][3,4]. However, the survival rates of the patients diagnosed with GBM and receiving first-line treatment remain very low. The median overall survival (OS) is 12–15 months, while only 3% of patients have a progression-free survival (PFS) of more than 5 years [5]. The MGMT (O6-methylguanine–DNA methyltransferase) promoter is a well-established predictive marker of response in GBM patients receiving TMZ. The epigenetic silencing of the MGMT gene by promoter methylation compromises DNA repair, improving response to TMZ and leading to longer survival of glioblastoma patients [6]. Inevitably, all GBM patients receiving RT + TMZ and/or adjuvant TMZ therapy relapse; the median PFS upon completing the first line of treatment varies between 1, 5 and 6 months [7]. Lomustine (CCNU), an alkylating agent, is sometimes administered as ultimate treatment option to recurrent GBM patients with minor therapeutic benefit [8][9][10][11][8,9,10,11].
In 2009, the U.S. food and drug administration (FDA) approved bevacizumab for the treatment of GBM with relapse after prior RT + chemotherapy [12]. Bevacizumab is a recombinant humanized monoclonal antibody, with anti-angiogenic properties by blocking vascular endothelial growth factor A (VEGF-A). However, its moderate clinical benefit and unproven OS advantage to date have withheld approval by the European medicine agency (EMA) [13][14][15][16][13,14,15,16]. The most recent therapeutic approach for recurrent GBM, which received FDA approval in 2011, is a device known as tumor-treating fields (TTF) [17]. In 2015, the device was also granted FDA approval for newly diagnosed GBM [17]. The device delivers low intensity, alternating electric fields to the tumor, therewith inhibiting glioma cell proliferation [18][19][18,19]. Moderate improvements in the survival of newly diagnosed GBM patients have been observed by adding TTF as an adjuvant treatment upon completing the standard of care treatment [20][21][20,21]. In Europe, the use of TTF is very limited to date, as the appropriate usage and implementation of the device in daily clinical practice presents many challenges [22][23][22,23].
Despite these limited additions to the arsenal of treatments, the prognosis of GBM patients remains dismal [24][25][24,25]. Two key players are involved in failure of conventional and targeted therapies: (1) the tremendous intra- and inter-tumoral heterogeneity of GBM and (2) the blood–brain barrier (BBB) [26][27][28][26,27,28]. GBM heterogeneity contributes to drug resistance and treatment escape and comprises a complex and arduous obstacle to overcome [29][30][31][29,30,31]. Extensive genetic and epigenetic profiling led to the classification of GBM tumors into three distinct molecular subgroups (classical, mesenchymal and proneural) as well as to the characterization of distinct DNA methylation profiles and/or expression patterns within these GBM subgroups [32][33][34][32,33,34]. Additionally, single-cell RNA sequencing analysis revealed different molecular subtypes within each tumor that can dynamically adapt to micro-environmental cues [34][35][36][37][34,35,36,37]. To date, these findings provide a better understanding of the heterogeneous nature of GBM; however, their clinical relevance, in particular in relation to drug treatment, is still limited [38].
The second major obstacle in GBM treatment is the BBB, which prevents effective delivery of drugs to the central nervous system (CNS). Therefore, to achieve any therapeutic response, it is of utmost importance that drugs cross the BBB and reach the tumor region in therapeutically effective concentrations. Drug discovery tools have been developed to identify optimal drug candidates for CNS penetration based on their physicochemical properties [39][40][39,40]. Moreover, efforts are being directed towards assessing CNS penetration and actual target delivery of new agents, as noted in the increasing number of phase 0 trials for GBM [41][42][43][41,42,43]. In addition, new delivery techniques, such as focused ultrasound sonication (FUS) and/or the use of nanoparticles to encapsulate therapeutic molecules, are being used to enhance systemic drug delivery into the CNS [44][45][46][44,45,46]. Examples include chemotherapeutic agents widely used in clinical practice, such as paclitaxel, cytarabine, carboplatin, etoposide and daunorubicin [47][48][49][50][51][52][53][47,48,49,50,51,52,53].
Based on these developments, a renewed interest in the available anticancer agents has arisen. With tools available to predict, enhance and assess drug delivery to CNS tumors as well as approaches to define markers of tumor sensitivity to specific compounds, the available arsenal of approved anticancer agents may be re-evaluated for potential GBM treatment. This approach, known as drug repurposing or drug repositioning, is a recognized strategy in drug discovery aiming to identify secondary indications for already approved drugs [54][55][56][54,55,56]. Given the unmet need for novel therapeutic options for GBM, drug repurposing may be a valuable tool, bypassing the delays and high costs of the novel drug development process and providing new drug candidates against GBM within a relatively short timeframe.
2. The Blood–Brain Barrier and Drug Efflux Pumps
The BBB is a neurovascular unit that, in physiological conditions, acts as a ‘gatekeeper’ [57]. The main task of the BBB is to maintain the brain homeostasis by controlling the passage of endogenous and exogenous molecules from the blood stream into the CNS [57][58][57,58]. Structurally, the BBB consists of endothelial cells interconnected with a complex network of proteins (tight junctions), while pericytes and astrocytic end-feet provide an additional structural support to the brain microvasculature (Figure 1) [57][59][57,59]. Tight junctions (TJs) are the key feature of the BBB and responsible for the impediment of polar solutes through intracellular and paracellular diffusion pathways [57]. TJs consist of claudins, occludins, junction adhesion molecules (JAMS) and various cytoplasmic accessory proteins, such as Zonula occludens-1, -2, -3 (ZO-1, ZO-2, ZO-3) (Figure 2) [60]. The transport of molecules across the BBB can be achieved by different routes, including passive diffusion, solute carriers (SLC), ATP-binding cassette (ABC) transporters, transcytosis and receptor-mediated transport [61][62][61,62]. Lipid soluble molecules can passively diffuse the BBB and reach the CNS at a rate that is linked to their physicochemical properties [40].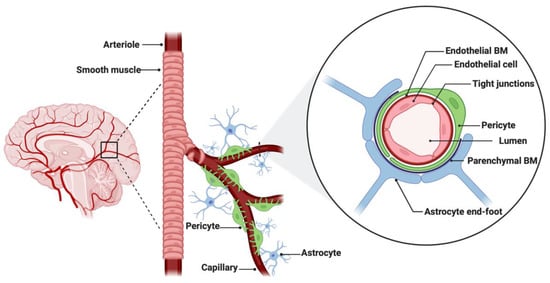
Figure 1. Anatomical features of the blood–brain barrier (BBB). The structure of the BBB in normal physiology consists of endothelial cells interconnected with a complex network of proteins (tight junctions), while mechanical support is provided by pericytes and astrocytic end-feet. The parenchymal and endothelial basal membranes (BM) provide additional strengthening to the cell attachments. Figure was created in BioRender.com (accessed on 5 July 2022).
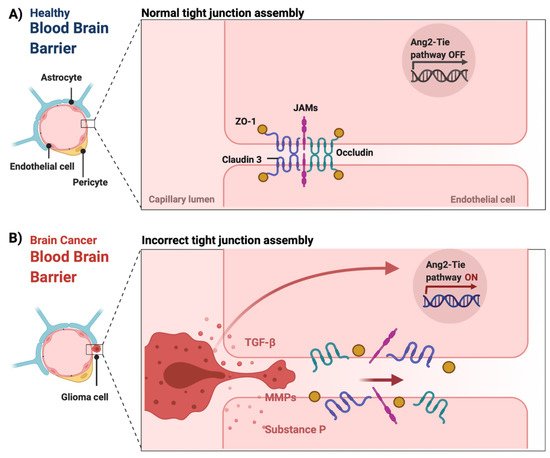
Figure 2. The integrity of the blood–brain barrier in physiological and malignant conditions. (A) In physiological conditions, tight junctions (claudin 3, occludin, junction adhesion molecules (JAMS) as well as cytoplasmic accessory proteins, such as Zonula occludens-1 (ZO-1)) of the endothelial cells remain intact maintaining the integrity of the BBB. (B) In CNS tumors, the release of chemical mediators by the tumor cells, such as substance P, matrix metalloproteinases (MMPs) and transforming growth factor beta (TGF-β), can cause the loss of tight junctions, which leads to the dysfunction and disruption of the BBB [60][63][64][65][60,69,70,72]. Additionally, the overexpression of angiopoietin-2 (ANG-2) is linked to vascular malformations and pericyte detachment through the hypoxic upregulation of VEGF, which subsequently promotes angiogenesis at the tumor margin [66][68]. Figure was created in BioRender.com (accessed on 20 May 2022).