Mitral regurgitation is the second-most frequent valvular heart disease in Europe after degenerative aortic stenosis. The mitral valve is a complex anatomical structure whose physiological functioning relies on the biomechanical properties and structural integrity of its components. Their compromise can lead to mitral valve dysfunction [2]. Assessing its morphology can reveal various normal and abnormal features, which can be associated with deteriorating clinical outcomes [3]. Transthoracic echocardiography is the first diagnosis approach that should be performed to assess the valve disfunction, giving a complete morphological description of the structures, the regurgitant mechanism, and etiology [3].
- mitral regurgitation
- mitral valve
- echocardiography
1. Introduction
2. Etiology and Regurgitant Mechanisms
2.1. Primary Mitral Regurgitation
In this group, structural valvular damage is observed in the leaflets, chordae tendineae, annulus, or papillary muscles. The main cause of primary MR is the myxomatous degeneration of the leaflets resulting in valve prolapse. There is an important variability in the severity of myxomatous degeneration from fibroelastic deficiency to Barlow’s disease (commonly characterized by bileaflet prolapse). Other causes of primary MR are the leaflet perforation and cleft leaflets as well as connective tissue diseases, drugs, rheumatic diseases, or even radiation [7].2.2. Secondary Mitral Regurgitation
The main characteristic of this group is the absence of structural damage of the leaflets and subvalvular apparatus, such as the MR subsidiary to LV geometry alterations, ventricular remodeling, inferobasal segmental disorders, or atrium morphology alterations. Secondary MR due to alterations in the geometry of the LV should be differentiated into ischemic and non-ischemic etiology. The remodeling that occurs in both processes may have common characteristics; hence, both situations produce MR due to ventricular dilatation and lateral displacement of the papillary muscles, causing reduced valve closing forces and abnormally increased tethering forces of the leaflets to LV. This process is self-perpetuating, as MR leads to LV dilatation, which leads to more laterally papillary muscle displacement, annular dilatation, and then more MR. Apical displacement of the coaptation line within the LV is appreciated, conditioning an incomplete MV leaflet closure. It is essential to understand the global relationship between the LV, papillary muscle position, and leaflet motion and coaptation line to make an accurate etiological diagnosis [8,9]. The ischemic etiology should be suspected in the presence of inferior regional wall motion abnormalities (scars, dyskinesia, hypokinesia), which cause movement restriction in the posterior leaflet, generating the MR, whereas the non-ischemic is characterized for the restriction of both leaflets, LV dilatation, and displacement of both papillary muscles [10].2.3. Carpentier Classification
MR can be classified according to the Carpentier classification (Table 1), which facilitates the understanding of the etiology as well as therapeutic approach [13].
| Carpentier’s Classification |
Leaflets Motion | Anatomical Session | Etiologies |
|---|---|---|---|
| Type I | Normal. | Leaflet perforation. Annular dilatation. |
Degenerative (annular calcification), infectious endocarditis, inflammatory, congenital cleft defect. |
| Type II | Excesive. | Chordal rupture. Chordal elongation. Papillary muscle rupture. |
Degenerative (Barlow’s disease), congenital, infectious, ischemic. |
| Type IIIa | Restricted in both systole and diastole. | Commisural or chordal fussion. Leaflet thickening. Leaflet calcification. |
Rheumatic, inflammatory, radiation, drugs. |
| Type IIIb | Restricted in systole. | Ventricular dilatation. Chordal thickening or shortening. |
Ischemic and non-ischemic. |
3. Severity Assessment in Practice
MR severity assessment is a challenging process in which a multimodality evaluation, integrating quantitative, semiquantitative and qualitative methods, as well as a detailed evaluation of the morphology and function of both LV and LA is the key [6]. There is a strong correlation between the hemodynamic status of the patient and the quantification of the MR. Quantification variability due to the regurgitation dependence on the cardiac afterload and preload makes it important to choose the right clinical time to perform a systematic and accurate echocardiographic assessment in a dynamic scenario [15,16].
3.1. Quantitative Parameters
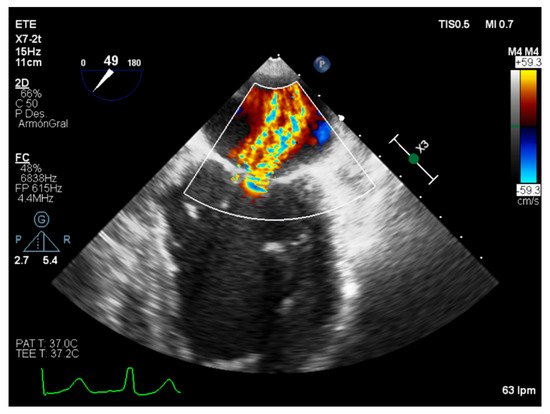
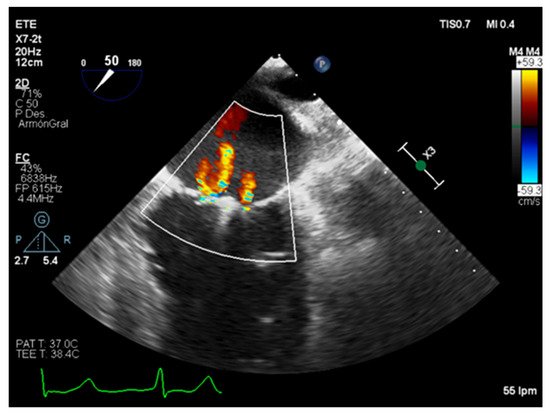
MR should be evaluated by quantitative parameters along a continuous scale if possible [7]. Severity quantification derived from the Doppler color regurgitant flow visual assessment evaluating LA occupation and size is incorrect. The Doppler flow visual assessment should only be used to detect the MR; hence, the flow jet size and the MR are not only dependent on the MR severity but technical factors (gain, color flow scale settings) and the hemodynamic scenario. In this sense, for a similar MR severity, patients with high LA pressures, eccentric jets, or dilated LA will show a smaller flow area in front of those with normal LA size and pressures [17]. Notwithstanding, the detection of a great eccentric flow directed towards the posterior atrial wall are favorable for a severe MR. On the contrary, small and thin flows reaching right above the mitral valves are suggestive of mild MR [16]. A first approach to quantify the severity of the MR is the vena contracta (VC) measurement (Figure 1). The VC is the narrowest portion of the regurgitant jet at the level or just distal to the regurgitant orifice area (EROA) and reflects the basic diameter of the regurgitant office [8,18]. The measure of the VC should be performed perpendicular to the coaptation line, and it is necessary to appreciate the jet convergence surface, the VC, and the jet expansion to the LA in the same place. Attention should be paid to ensure a high frame rate and spatial resolution [3]. A VC value smaller than 3 mm suggests mild regurgitation and when the width exceeds 6 mm indicates severity.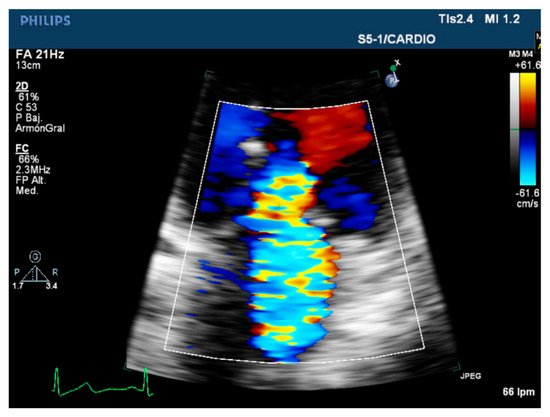
3.2. Semiquantitative and Qualitative Parameters
Given the limitation and pitfalls of the quantitative parameters, it is recommended to analyze them together with qualitative observations that can reflect the hemodynamic consequences of the MR in the LV, LA, and the pulmonary circulation [6]. The mitral valve morphology, beyond being suggestive of a possible etiology, can sustain the severity quantification of the regurgitation if a flail leaflet or a ruptured chordae is appreciated. The evolution of the color in the MR should be used at first to mainly detect the MR but not to quantify its severity. The color flow jet density, duration and direction, as well as the number of regurgitant jets observed can be useful, bearing in mind its tendency to overestimate or underestimate depending on the driving pressures and jet eccentricity. This parameter reflects the high systolic pressure gradient between the LV and LA [5]. Its continuous Doppler wave morphology, from faint and parabolic in mild regurgitation to dense and triangular when severe, can be useful as well [16]. Curiously, the velocity of the jet will not indicate the severity of the MR, but the intensity of the signal (a dense flow jet with a full envelope), which is considered a qualitative parameter of the MR, suggests severity [17].3.3. Role of Stress Echocardiography
Exercise intolerance and appearance of the symptoms, essentially dyspnea, with physical efforts constitute a Class I indication for intervention in patients with primary severe MR [35]. Stress echocardiography, which can be performed with exercise testing or dobutamine infusion, allows unmasking severe regurgitation as well as assessing LV and right ventricle performance and pulmonary pressure under stress conditions [36]. The appreciation of an MR severity increment, a lack of ventricular contractile reserve, and a systolic pulmonary pressure rise over 60 mmHg are predictive of worse prognosis, symptoms progression, and need for an intervention [37]. Particularly in the ischemic population, characterized by eccentric and variable regurgitant flows, stress echocardiography has a especial interest in patients with dyspnea out of proportion with the severity of their resting LV performance and MR severity, those whom have suffered acute pulmonary edema without a clear pathophysiological mechanism, and in the peri-surgical time, before assessing a need to mitral intervention when revascularization is planned and following surgery to identify persistence of pulmonary arterial hypertension [38]. On the other hand, secondary MR has also demonstrated a dynamic behavior during exercise and stress echocardiography, providing useful information to predict outcomes and plan further therapeutical options in these patients, such as cardiac resynchronization or transcatheter edge-to-edge repair [39].4. Assessment of Suitability of Valvular Repair
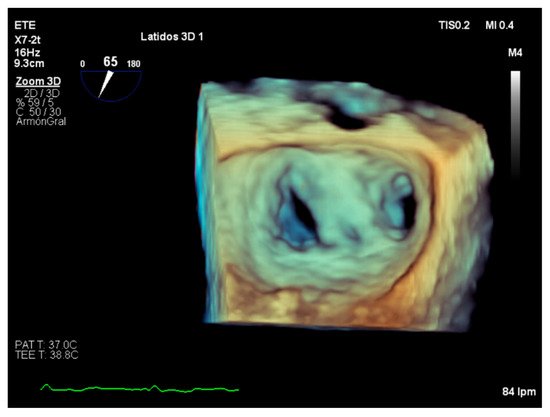
If there is an indication for surgery, mitral valve repair should be considered as a first choice if feasible since it has shown better survival rates [7,17]. A transesophageal echocardiography evaluation on morphology and etiology is necessary prior to every technique consideration. The paradigm of valve abnormality leading to a successful repair is the Carpentier type II, especially when involving one scallop of the posterior leaflet [7]. In primary MR, there are few echocardiographic findings that suggest a high probability of significant MR after a valve repair: the presence of a large central jet, annular diameter higher than 50 mm, involvement of three or more scallops, substantial valve and ring calcification, and lack of valve tissue, for instance, after suffering and infectious endocarditis [10]. Transcatheter edge-to-edge repair may be considered in those symptomatic patients with high surgical risk [39]. Findings of a perforated leaflet, lack of primary and secondary chordal support, severe calcification of the grasping area, significant mitral stenosis, short posterior leaflet (shorter than 7 mm), systolic and diastolic restriction typical of rheumatic valve disease, and the presence of a gap superior to 2 mm between leaflets makes the mitral valve unsuitable for edge-to-edge repair [40].5. Role of Intraoperative Echocardiography
Intraoperative transesophageal echocardiography is a basic component of contemporary cardiac surgery planning and results evaluation, allowing the detection of suboptimal results inside the operating room [41]. In addition, assessment of the results and follow-up evaluation is essential in the transcatheter edge-to-edge guiding procedure (Figure 5) [42].