Boswellia trees, found throughout the Middle East and parts of Africa and Asia, are the source of frankincense oil. Since antiquity, frankincense has been traded as a precious commodity, but it has also been used for the treatment of chronic disease, inflammation, oral health, and microbial infection.
- inflammation
- oral health
- frankincense
- infection
- microbiology
1. Introduction

2. Description of Frankincense Resins, Oils, and Boswellic Acids
The resin is available in yellowish, bluish, and greenish shades, and is composed of 3–8% volatile oils containing various terpenes and sesquiterpenes, 60–70% resin, and 27–35% gum [15][48]. In the mid-twentieth century, it was found that the gum contains two types of polysaccharides [16][49]. More recently, the composition showed that the monosaccharides present were predominantly galactose, arabinose, and glucuronic acid, along with small amounts of rhamnose and glucose [17][50]. However, recent scientific advancements allow reusearchers to identify the molecular content of diverse frankincense products such as incense mixtures, components of conventional medicines, and archaeological specimens. The concentrated volatile, aromatic liquid obtained from different parts of the plant such as roots, seeds, leaves, flowers, and resins is called an essential oil. Mostly, a distillation process is used to extract the essential oil from Boswellia plants [18][51]. The main chemical constituents of frankincense oil are pentacyclic triterpenoids [19][52], tetracyclic triterpenoids [20][53], and a variety of other oils [21][54]. The most common characteristic and intensely studied component in frankincense are the pentacyclic triterpenoids [7][22][7,55]. The major active components of frankincense are the boswellic acids (BA), which are extracted from the woody parts of different Boswellia trees. The representative phytochemicals are β-boswellic acid, acetyl-β-boswellic acid (ABA), 11-keto-β-boswellic acid (KBA), 3-acetyl-11-keto-β-boswellic acid (AKBA), α-boswellic acid, and acetyl-α-boswellic acid. Figure 2 shows the chemical structure of the main BA.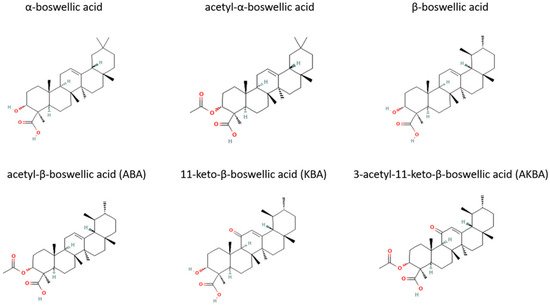
3. Modern Medicinal Uses of Frankincense
Many plant components from Boswellia are used to treat chronic diseases with comparatively few side effects [33][34][67,68]. Indian traditional medicine practice narrates that Boswellia decoctions were used to treat various gastrointestinal tract conditions such as diarrhea, flatulence, alimentary stoppage, and vomiting [35][36][37][38][69,70,71,72]. It was believed that the decoctions contain active ingredients from Boswellia, which are useful in treating the above-mentioned diseases. Furthermore, the extract was used to treat bronchitis, asthma, hoarseness, dyspnea, cough, and cold [39][40][73,74]. The gum extracts or resins from Boswellia sp. and their triterpenes, especially BA, have attracted the attention of pharmacologists, medicinal chemists, and biochemists as therapeutic agents due to their efficacy in treating rheumatoid arthritis and chronic inflammation without side effects and toxicity. The gum exudate obtained from the bark of the tree B. serrata, also called Indian olibanum, has been extensively used in the treatment of arthritis, asthma, ulcers, and skin diseases by practitioners of Indian traditional medicine [15][25][48,58]. It has also been widely used in various formulations for the treatment of inflammation related disorders in the past decade [15][41][48,75]. One study analyzed the effects of gum resins of B. serrata (900 mg daily divided in three doses for 6 weeks) on human patients suffering from chronic colitis [33][42][67,76]. The authors found that out of 20 patients treated with Boswellia gum resin, 18 patients showed an improvement in one or more parameters, including stool properties, histopathology and scanning electron microscopy characterization, hemoglobin, serum ion, calcium, phosphorus, proteins, total leukocytes, and eosinophils [33][42][67,76]. The control group (10 patients) was given sulfasalazine at a dose of 1 g three times a day for 6 weeks. The authors reported that 6 out of 10 patients in the control group showed similar improvements with the same parameters tested in the B. serrata group. ResearcThers is study demonstrates that a gum resin preparation from B. serrata might be effective in the treatment of chronic colitis, with minimal side effects [33][42][67,76]. The same research group evaluated the effects of B. serrata gum resin on the treatment of patients with bronchial asthma [40][74]. Their data demonstrated that 70% of patients treated with 300 mg thrice daily for 6 weeks showed improvement of disease, evident by the disappearance of physical symptoms and signs such as dyspnea, rhonchi, number of attacks, as well as a decrease in eosinophilic counts. The control group (treated with placebo) only showed 27% of improvements in symptoms [40][74]. These data imply that gum resin from B. serrata could serve as a pharmacological agent in the treatment of bronchial asthma. Gum resin from B. serrata was reported to be a potential remedy for inflammation, and it has been used as a folk medicine for topical and systemic inflammatory diseases for centuries [15][48]. The oleo gum resin of B. carterii has been used in folk medicine to treat cough and asthma and as an embalming fluid for human corpses. In addition, it has been used as an incense, respiratory antiseptic, and diuretic stimulant [25][58]. The oleo gum resin of B. serrata and B. carterii were also used in traditional medicine in different countries to treat rheumatic and other inflammatory diseases, including Crohn’s disease and ulcerative colitis [42][43][44][76,77,78]. However, B. serrata was reported to be the least effective in recurrent infections [45][79]. In addition, frankincense extracts and oils were used as antiseptic agents in mouthwash and also used to treat cough and asthma [43][77]. Furthermore, recent studies on animals and humans have demonstrated the efficacy of resin gum of B. serrata to treat inflammatory bowel disease, asthma, osteoarthritis, and rheumatoid arthritis [42][46][47][76,80,81]. Though frankincense has been known for its medicinal properties since antiquity, it is still widely used in modern medical treatment. In 2010, Moussaieff and Mechoulam reviewed Boswellia resin constituents in vitro, in vivo, and in clinical trials studies [48][82]. Indeed, in Ayurvedic medicine, different parts of the Boswellia tree and derived extracts are used for the treatment of respiratory, gastrointestinal, immune system, and skin conditions. Most of the published work focuses on the pharmacological activities of boswellic acids, specifically on their anti-inflammatory, analgesic, and anti-arthritic properties. As an example, there is growing evidence to support the clinical efficacy of Boswellia in osteoarthritis patients. However, there is inadequate evidence to demonstrate the clinical efficacy in rheumatoid arthritis patients [49][83]. The application of frankincense to treat different diseases of recent times is discussed below and summarized in Figure 3. Frankincense has been used to treat both infections and chronic diseases.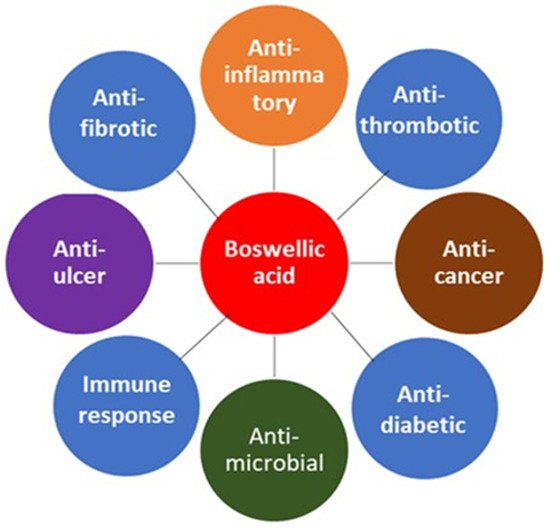
4. Antimicrobial Activity of Frankincense
The oleo gum resin essential oils from B. carterii (Somalia), B. papyrifera (Ethiopia), B. serrata (India), and B. rivae (Ethiopia) were individually tested against different fungi and Gram-positive and Gram-negative bacteria. The essential oils exhibited significant antifungal activity against both C. albicans and C. tropicalis, with the essential oils from B. carterii and B. papyrifera showing the best activity [50][97]. The MIC values for C. albicans and C. tropicalis were 12.86 and 12.86 μg/mL (B. serrata), 6.16 and 6.16 μg/mL (B. carterii), 6.09 and 6.09 μg/mL (B. papyrifera), and 2.65 and 27.38 μg/mL (B. rivae), respectively, compared with the MIC of 0.15 μg/mL for amphoterecin B. The essential oil of B. rivae resin exhibited the best activity against C. albicans [50][97]. Limonene present in the essential oils is thought to be responsible for the antifungal activity [51][98], since oleo gum resin essential oils without limonene lack antifungal activity. The oleo gum resins also showed significant antibacterial effects against Gram-positive S. aureus and S. epidermidis, with MIC values ranging from 3.52 to 107.20 μg/mL. These values can be compared with the MIC of 1 μg/mL for vancomycin and 2 μg/mL for amikacin used as controls in the experiments [50][97]. The frankincense compounds against Gram-negative E. coli and P. aeruginosa showed MIC ranging from 6.60 to 107.18 μg/mL, compared to the vancomycin MIC of 10 and 5 μg/mL for E. coli and P. aeruginosa, respectively. It is noteworthy that some of the frankincense compounds had antimicrobial effects at concentrations that were comparable or very close to concentrations of the standard antibiotics used in the in vitro experiments. Future studies might confirm and expand the results to in vivo and clinical models.
Dental caries and periodontitis remain two of the major oral diseases that affect more than half of the global population [52][108]. Periodontitis is often referred as a common inflammatory disease in humans. The etiology of these diseases has been linked to certain bacterial species, plaque and biofilm formation, and the resultant inflammatory states. Current therapies for treating periodontal disease place an emphasis on biofilm removal. This is exercised via a combination of mechanical (such as scaling and root planing) and antibiotic treatments. However, these treatment modalities are still unable to fully remove biofilms. This has led to an interest in incorporating herbal extracts into current treatment regimens.
Many studies have been performed using the resin of B. serrata. As noted above, this resin contains boswellic acid, which are the active components in its anti-inflammatory effects. In addition, both the boswellic acid and the essential oils of B. serrata exhibit antimicrobial properties. Of the four major boswellic acids, acetyl-11-keto-β-boswellic acid (AKBA), has consistently demonstrated the greatest antibacterial effects. In fact, several studies have determined that AKBA is the most active component in the resin of B. serrata and other Boswellia species [53][109].
In terms of antibacterial effectiveness, AKBA isolated from B. serrata demonstrated activity against Streptococcus mutans, Enterococcus faecalis, Enterococcus faecium, Actinomyces viscosus, Streptococcus sanguinis, Fusobacterium nucleatum, Prevotella intermedia, and Porphyromonas gingivalis. Furthermore, the post-antibiotic effects of AKBA were determined to be greater than those of ciprofloxacin, and AKBA was also shown to inhibit biofilms of the cariogenic bacteria S. mutans [53][109].
In a double-blinded, randomized clinical trial, the effectiveness of traditional scaling and root planing methods were compared to the use of B. serrata extract or powder [54][110]. The results indicated that the addition of B. serrata extract or powder to traditional scaling and root planing treatments leads to better gingival health as measured by gingival, plaque, and bleeding indices, as well as probed pocket depths [54][110]. The authors concluded that the anti-inflammatory properties of B. serrata extract had results comparable or even superior to traditional scaling and root planing treatments. Given its antibacterial, antifungal, and antioxidant properties, it is not surprising that frankincense also has promising beneficial effects on oral health.
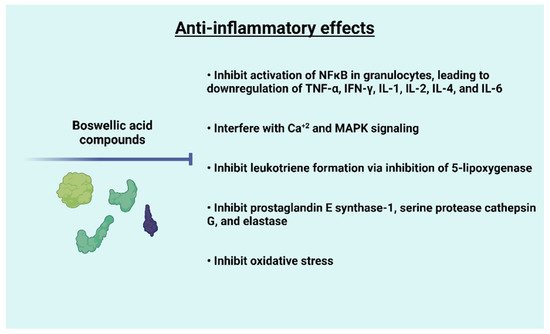
5. Anti-Inflammatory Effects of Frankincense