Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Luca Di Pietrantonio and Version 2 by Camila Xu.
Somatic dysfunction (SD) is classified by the ICD 11 as a “Biomechanical lesion, not elsewhere classified”; however, the definitions are not equally shared and codified by osteopathic professionals.
- exclusion zone water
- interstitial fluid pressure
- water
- somatic dysfunction
1. Introduction
The main means available to osteopathic medicine is to assess tissues by palpating, in particular tissues of the musculoskeletal system, with the aim of diagnosing a possible somatic dysfunction (SD).
By underscoring some contradictory aspects, several researcheuthors have called into question SD, by defining it as a nosological entity detectable on palpation [1][2][3][1,2,3].
SD is classified by the ICD 11 [4] as a “Biomechanical lesion, not elsewhere classified”; however, the definitions are not equally shared and codified by osteopathic professionals [1][5][6][7][1,5,6,7].
SD presents the characteristics of impaired or altered function of components related to the somatic system, involving skeletal, arthrodial, and myofascial structures, and osteopathic manipulative treatment (OMT) is aimed at the treatment of SD [8][9][10][8,9,10].
The osteopathic literature describes the relationship between SD and OMT in many studies [10][11][12][13][10,11,12,13].
OMT is a drug-free manual medicine, a patient-centered, whole-body intervention. OMT has shown positive effects in different fields such as gynecology and obstetrics, neonatology, chronic inflammatory disease management, and musculoskeletal disorders [14][15][16][17][18][19][14,15,16,17,18,19].
There are many aspects to consider regarding the etiology and diagnosis of SD, and the osteopathic literature provides details on the signs that characterize it, including tissue texture changes [8][20][21][22][8,20,21,22].
Over the last few years, some researcheuthors have proposed a variety of interpretation models in order to clarify the mechanisms of onset and the inherent characteristics of tissue alterations concerning SD. Among such models, there are also clinical reasoning and decision-making procedures suitable to establish a treatment routine [23][24][25][26][27][23,24,25,26,27].
Recent knowledge suggests that tissue, and, in particular, connective tissue, may react by modulating the inflammation degree. This issue should also be extended to any response to OMT, and several studies show the efficacy of OMT on inflammatory tissue levels [28][29][30][31][32][33][34][35][28,29,30,31,32,33,34,35].
LGI would act on the ECM, and alter its structure, such as in fibrosis, which is defined as a lesion of the connective component in an organ or tissue [36].
These alterations occur through mechanisms mediated by the environment in which the tissues are placed, namely water [37][38][39][40][41][37,38,39,40,41].
The water under consideration is water present in living matter. It has particular biophysical characteristics, which could exemplify the functioning of both healthy and injured tissues [39][42][43][39,42,43].
2. New Model Regarding the Characteristics of Somatic Dysfunction
With the acronym TART (tenderness, asymmetry, range of motion abnormality, and tissue texture changes), osteopathic literature accurately provides the characteristic elements of SD, at which OMT is aimed [7][8][21][7,8,21]. However, some researcheuthors disagree on the relevance to be attributed to different clinical signs: some indicate the range of motion abnormality as fundamental for a diagnosis of SD, but there is no univocal evidence on the reproducibility in the evaluation [44][114]. Other researcheuthors suggest the need for the presence of at least 2 of these 4 signs; still, others do not consider the sign of hypersensitivity or tenderness [1][5][6][7][45][1,5,6,7,115]. Regarding the asymmetries of the musculoskeletal structures, these can occur for a variety of causes, and are, therefore, difficult to attribute solely to SD [46][47][48][116,117,118]. In light of the results of this resviearch, researchersw, we believe that among the 4 clinical signs considered, tissue texture changes are the most significant to define an SD, thus proposing the hypothesis that SD can be compared to a condition of LGI. The mechanisms underlying SD are still widely discussed in the literature, but it is reasonable to think that without first having tissue texture changes, caused by inflammatory phenomena, the presence of the other three clinical signs is not possible. ThWe researchers ssuggest that an inflammatory phenomenon could determine an alteration of the tissue as described in the chapters above, and only subsequently tenderness, altered movement, and asymmetry of the musculoskeletal structures can occur (Figure 12D).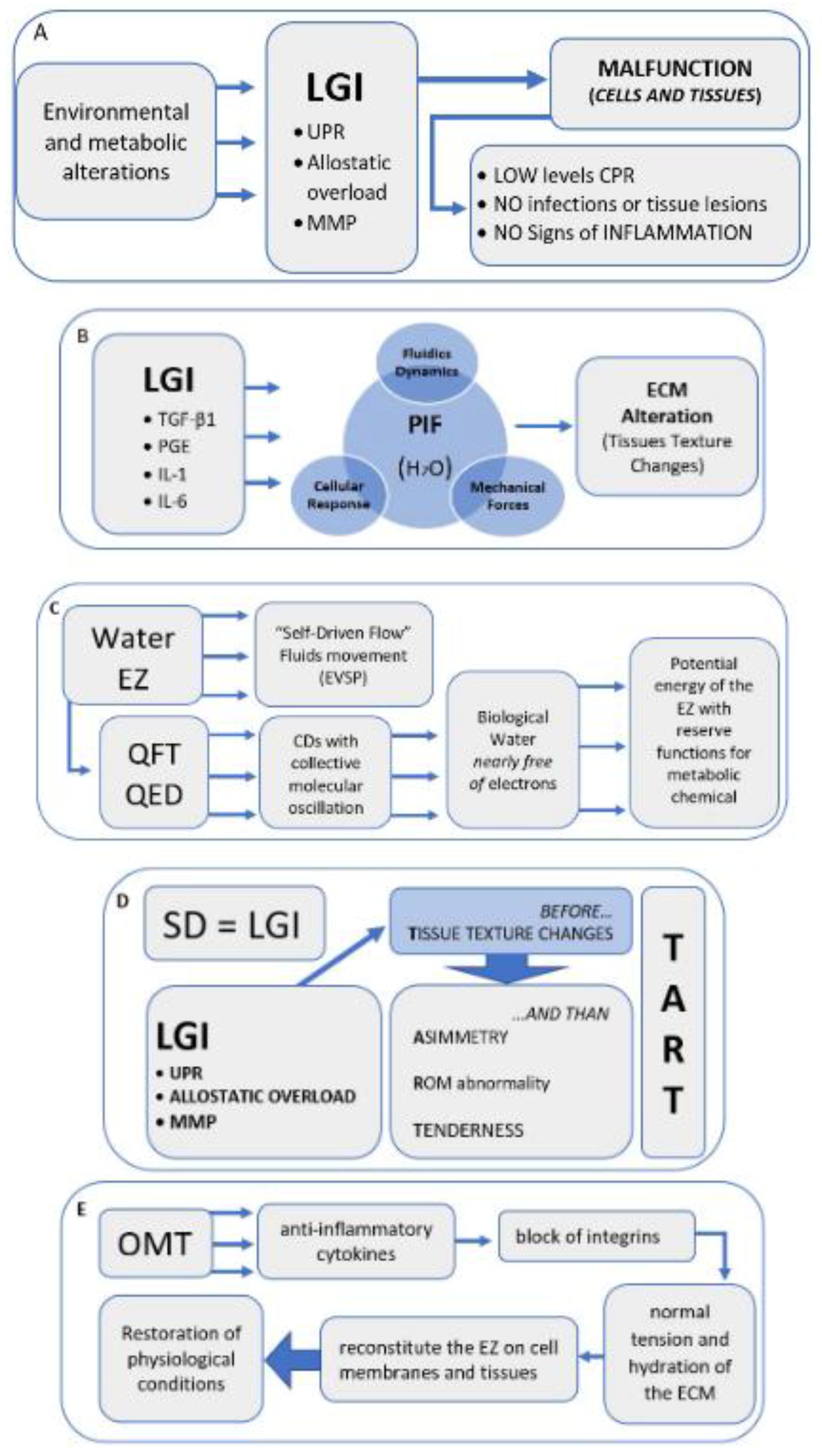
Figure 12. Narrative flow charts.
Narrative flow charts.