Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Irena Baranowska-Bosiacka and Version 3 by Jessie Wu.
CXCL1 is a chemokine crucial in inflammation as a chemoattractant for neutrophils in physiology and in selected major non-cancer diseases.
- CXCL1
- chemokine
- cytokine
1. Cartilage and Bone Tissue
1.1. Bone, Fracture Healing, Osteoporosis
CXC motif chemokine ligand 1 (CXCL1) is involved in the physiology and pathology of bone tissue. Most data are based on studies of KC, a mouse paralog for human CXCL1, and for this reason require confirmation in research on humans.
The expression of ligands for CXCR2, such as KC and MIP-2, has been shown to be elevated in murine osteocytes under shear stress [1][2][51,52] and by parathormone (PTH) and parathyroid hormone-related protein (PTHrP) [3][53]. This increase in KC expression causes osteoclast precursors to migrate [1][51], and the subsequent activation of CXCR2 on these cells enhances osteoclast maturation [4][54]. This is followed by either bone remodeling or bone resorption under the influence of factors that stimulate KC expression. Human osteoclast precursors exhibit CXCR2 expression [5][55] but it is reduced during differentiation of these cells into osteoclasts. It appears that CXCL1 may have the same properties in bone as KC, and so may participate in bone modelling in humans, although this should be confirmed by further studies.
Due to the induction of osteoclast maturation by CXCR2 ligands, CXCL1 levels are positively correlated with osteoporosis in humans [6][56]. Also, bone marrow adipocytes produce ligands for CXCR2 [4][54], which leads to the weakened bone structure in mice with advanced age or obesity [4][54]. If a similar mechanism occurs in humans, then this could account for the frequent bone fractures in older people or those with obesity. CXCL1 is also important in fractures—a condition associated with an increase in KC expression in mice [7][57]. This chemokine is indirectly important in fracture healing, via neutrophils recruited by this chemokine [7][57].
The expression of ligands for CXCR2 by bone marrow adipocytes may support the formation of cancer bone metastasis in elderly or obese people [4][54]. Also, the increased expression of ligands for CXCR2 in osteocytes under shear stress and PTHrP may support bone metastasis of some cancers, including breast cancer [2][8][52,58]. Not less important is CXCL1 production by cancer cells in bone metastasis [9][59], as CXCL1 stimulates cancer cell proliferation [10][11][12][35,37,60], as well as participating in bone remodeling during bone metastasis formation [4][9][54,59]. If a tumor cell from the blood stops in bone tissue, it causes bone remodeling by secreting CXCL1 and hence bone metastasis.
1.2. Bone Marrow
Ligands for CXCR2, including CXCL1, are important in the self-renewal capacity of hematopoietic stem cells [13][61]. Human CD34+CD38- express CXCL1 as well as other ligands for CXCR2 such as CXCL2, CXCL6 and CXCL8/IL-8—chemokines crucial for hematopoietic stem cell maintenance.
CXCL1 is also significant in the regulation of whole body immunity via neutrophil egress from the bone marrow [14][15][62,63]. Two axes are responsible for the regulation of neutrophil release from the bone marrow. CXCL12/SDF-1→CXCR4 is responsible for the retention of neutrophils and homing of senescent neutrophils to the bone marrow [14][62], while CXCR2 ligands are responsible for neutrophil egress from the bone marrow [14][15][62,63]. Also, pro-inflammatory factors in the blood, such as LPS, increase CXCL1 expression in endothelial cells in the bone marrow—an effect dependent on β-adrenergic signaling [15][63] The release of neutrophils under the influence of pro-inflammatory factors in the blood is important in the fight against pathogens. Acute inflammation increases the levels of pro-inflammatory cytokines in the blood leading to the mobilization of neutrophils and subsequent accumulation of these cells at sites of intense inflammatory responses.
Chronic inflammation is associated with elevated levels of ligands for CXCR2, including CXCL1, which cause the expansion of monocytic myeloid-derived suppressor cell (MDSC) in the bone marrow as shown in mice [16][64]. This is associated with CXCR2 activation on granulocyte and macrophage progenitor cells (GMPs) [17][65], which reduces the expression of Sin3-associated 18 kDa polypeptide (SAP18). This, in turn, results in the activation of extracellular signal-regulated kinase (ERK) mitogen-activated protein kinase (MAPK) and signal transducer and activator of transcription 3 (STAT3), which increases granulocyte monocyte progenitor (GMP) differentiation into macrophages and dendritic cell progenitor cells (MDP) [17][65]. Subsequently, in the bone marrow, MDP differentiate into monocytic MDSC, resulting in an increase in the number of these cells. This effect is important in diseases with chronic inflammation. Expansion of monocytic MDSC in the bone marrow results in an increase in the number of these cells in the blood, which leads to an overall weakening of the immune system.
1.3. Rheumatoid Arthritis
Rheumatoid arthritis, estimated to affect less than 1% of the human population, is an autoimmune disease that is characterized by chronic inflammation which results in the destruction of joints [18][66]. One component of the pathophysiology of rheumatoid arthritis is an increase in CXCL1 expression in rheumatoid arthritis patients in the blood [19][67] and synovial fluid [20][21][68,69]. At the same time, CXCL1 expression in synovial fluid is higher in patients with rheumatoid arthritis than in those with osteoarthritis [19][21][22][67,69,70].
CXCL1 in the synovial fluid comes from fibroblast-like synoviocytes (FLS), chondrocytes and neutrophils (Figure 1). In particular, increased CXCL1 expression occurs in the lining layer [23][71]. FLS increases the expression of CXCL1 under the influence of pro-inflammatory cytokines such as TNF-α and IL-1β [20][24][68,72], whose expression is also increased in rheumatoid arthritis patients [25][26][73,74]. That means that chronic inflammation in joints increases the expression of TNF-α and IL-1β, which increases the expression of CXCL1. The synovial fluid in patients with rheumatoid arthritis also show increased levels of IL-17 [27][75], a cytokine that increases CXCL1 expression, particularly in FLS [28][76]. In FLS, the expression of CXCL1 is also increased by resistin, an adipokine produced by macrophages located in the synovium in patients with rheumatoid arthritis [29][77].
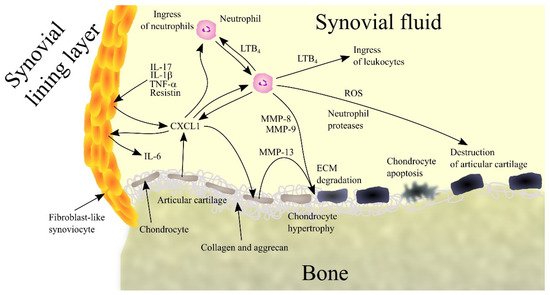
Figure 1. Importance of CXC motif chemokine ligand 1 (CXCL1) and neutrophils in rheumatoid arthritis. Patients with rheumatoid arthritis have elevated levels of interleukin-1β (IL-1β), tumor necrosis factor α (TNF-α), interleukin-17 (IL-17) and resistin in synovial fluid. These factors induce CXCL1 expression in fibroblast-like synoviocytes (FLS), chondrocytes and neutrophils, which leads to an increase in CXCL1 levels in synovial fluid. CXCL1 causes an increase in interleukin-6 (IL-6) expression in FLS. This chemokine causes leukotriene B4 (LTB4) synthesis in neutrophils and thus an ingress of more neutrophils and leukocytes into the joints. CXCL1 also causes an increase in matrix metalloproteinase-13 (MMP-13) expression in chondrocytes, which leads to extracellular matrix (ECM) articular cartilage degradation. Also responsible for this process are matrix metalloproteinase-8 (MMP-8) and matrix metalloproteinase-9 (MMP-9) produced by neutrophils. CXCL1 also causes chondrocyte hypertrophy and apoptosis. Finally, neutrophils secrete reactive oxygen species (ROS) and neutrophil proteases into synovial fluid. All these processes and factors lead to the destruction of articular cartilage and symptoms of rheumatoid arthritis. Abbreviations: CXCL1—CXC motif chemokine ligand 1; ECM—extracellular matrix; IL-1β—interleukin-1β; IL-6—interleukin-6; IL-17—interleukin-17; LTB4—leukotriene B4; MMP—matrix metalloproteinase; ROS - reactive oxygen species; TNF-α - tumor necrosis factor α; Source: own elaboration.
CXCL1 participates in rheumatoid arthritis by acting on various cells in the joints. It causes hypertrophy of chondrocytes [30][78] resulting in an elevated expression of MMP-13, an enzyme that degrades collagen and aggrecan. This results in degradation of ECM in articular cartilage followed by apoptosis of chondrocytes and degradation of cartilage in the joints.
CXCL1 also acts on FLS. Although it does not cause the proliferation of FLS [31][79], it does reduce collagen production in these cells, which interferes with the normal function of these cells in the joints. CXCL1 also increases the production of IL-6 in FLS [21][69], one of the factors causing an increase in IL-6 in synovial fluid in patients with rheumatoid arthritis; such a response does not occur in healthy individuals [21][24][69,72]. IL-6 is a cytokine that is involved in rheumatoid arthritis by causing bone resorption and by participating in inflammatory reactions [32][80].
CXCL1 causes an ingress of neutrophils into the joints [33][34][81,82], a process that also appears to require LTB4 [34][82]. CXCL1 has also been shown to act on neutrophils in the joints by increasing the production and secretion of LTB4 in these cells [34][82]. This bioactive lipid causes an ingress of leukocytes into joints, where they act destructively on joint tissue and thus contribute to the pathogenesis of rheumatoid arthritis. Neutrophils also produce MMP-8 and MMP-9 which degrade collagen [35][83]. Neutrophils also produce ROS, which have a destructive effect on joint tissue, and various proteases such as elastase, cathepsin G and proteinase-3, which are involved in joint tissue destruction and inflammatory reactions.
CXCL1 can also increase osteoclast activity, which leads to bone erosion [4][5][6][54,55,56]. However, the importance of CXCL1 in the destruction of bone tissue in the joints of patients with rheumatoid arthritis is yet to be thoroughly investigated.
2. Muscles
CXCL1 may play an important physiological role, particularly in muscle function. However, due to the lack of an appropriate research model, these are assumptions drawn from a mouse model for changes in KC chemokine expression. Therefore, this physiological aspect requires further studies on humans.
2.1. Muscle Physiology
Exercise is associated with an increase in the expression of IL-6 and CXC chemokines that are ligands for CXCR2, such as KC and lipopolysaccharide-induced CXC chemokine (LIX) in the muscle and blood of mice [36][37][38][39][40][84,85,86,87,88]. Significantly, the increase in KC expression in the muscle is independent of IL-6 [40][88]. IL-6 from the muscle travels via the blood to the liver, where the expression of KC increases, which then is responsible for the increase in blood KC levels [38][86]. KC also acts in an autocrine manner on muscle via CXCR2, which induces an increase in muscle insulin responsiveness, specifically an increase in glucose transporter 4 (GLUT4) recycling [36][84]. However, the same authors in a later study question the effect of KC and LIX on GLUT4 recycling in muscle [37][85]. KC also increases fatty acid oxidation [39][87] and muscle angiogenesis (Figure 2) [39][87].
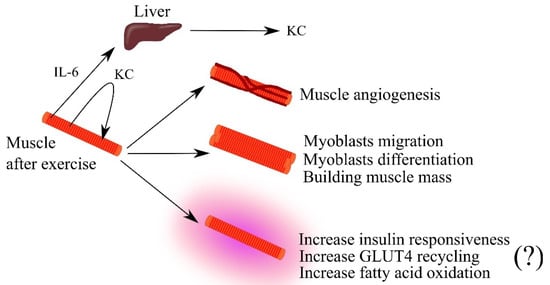
Figure 2. The importance of keratinocyte-derived chemokine (KC) in skeletal muscle physiology. Intense effort induces an increase in the expression of interleukin-6 (IL-6) and KC in muscle. IL-6 travels through the bloodstream to the liver where it increases KC expression. This leads to an increase in blood levels of this chemokine. KC secreted by muscle acts in an autocrine manner, causing muscle angiogenesis, the growth of muscle mass by acting on myoblasts, and increasing muscle efficiency by increasing insulin responsiveness and fatty acid oxidation in the muscle. Abbreviations: (?)—mechanism in question; GLUT4—glucose transporter 4; IL-6—interleukin-6; KC—keratinocyte-derived chemokine; Source: own elaboration.
KC is also considered a myokine as it causes proliferation, self-renewal of satellite cells and myogenesis from satellite cells—stem cells present in muscles that participate in regeneration [41][89]. KC is also a chemotactic factor for myoblasts and causes myogenic differentiation of these cells [37][85]. As a consequence of the action of KC, there is an expansion of the muscle and an increase in muscle efficiency. Also of note is the exercise-induced increase in blood levels of KC in mice, and most likely also CXCL1 in humans [38][86]. KC and CXCL1 cause the mobilization of neutrophils from the bone marrow, whose function is to destroy pathogens [14][62]. It can be speculated that exercise in the described mechanism may enhance immunity.
The expression of ligands for CXCR2 is also subject to upregulation in muscle regeneration, as shown by studies in cattle [42][90]. Their role in muscle regeneration is additionally indicated by the fact that their expression is tightly regulated by myostatin [42][90]. Further research in this area is required to determine the exact mechanism of muscle regeneration.
2.2. Muscle, CXC Motif Chemokine Ligand 1 (CXCL1)L1 and Obesity
CXCL1 participates in muscle disease mechanisms. Saturated fatty acids, particularly palmitate, cause myotube loss [43][91] which is associated with a decrease in the expression of certain myokines. At the same time, palmitate also increases the expressions of CXCL1 in human muscle and KC in mouse muscle [41][89]. In mice, KC stimulates proliferation and self-renewal of satellite cells [41][89] and thus it counteracts the negative effects of palmitate on muscle. A similar mechanism may occur in humans—palmitate may increase the expression of CXCL1 in muscle which then inhibits the adverse effect of this acid. This process is of importance as ~60% of the North American and European populations are overweight [44][92].
2.3. Tumor-Induced Muscle Wasting
CXCL1 may also participate in tumor-induced muscle atrophy, one of the components of cancer cachexia [45][46][93,94]. This section shows the effect that chronic inflammation has on muscle, as in advanced cancer. Patients with breast cancer [47][95], esophageal squamous cell carcinoma [48][96], ovarian cancer [49][97] and renal cell carcinoma [50][98] have elevated levels of CXCL1 in the blood. In addition, studies in mouse models have shown that factors from tumorigenesis increase KC expression in muscle [45][93]. KC, produced in muscle as well as secreted from a tumor, impairs myoblast differentiation, leading to muscle atrophy. This effect is also enhanced by other factors from the tumor such as insulin like growth factor binding protein 3 (IGFBP3) and CC motif chemokine ligand 2 (CCL2) [45][93]. Another mechanism by which KC causes tumor-induced muscle atrophy is the infiltration of skeletal muscle by immune cells, including neutrophils and macrophages [45][93]. These cells suppress myogenic differentiation, leading to tumor-induced muscle atrophy.