Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Carlos Daniel Varela-Chinchilla and Version 2 by Catherine Yang.
Breast implant illness refers to a combination of different symptoms related to breast implant surgery, including fatigue, brain fog, and arthralgias. This malaise occurs after cosmetic and reconstructive breast surgeries, although it has not been proven to be a disease. Complications associated with breast implants include breast pain, capsular contracture, infections, as well as other manifestations specific to breast reconstruction.
- BII
- breast
- implant
- illness
- surgery
- autoimmunity
- plastic surgery
- silicone
1. Introduction
Outstanding advancements have been made in the medical field since the inception of synthetic prosthetics [1][2][1,2]. Presently, prosthetics have changed disease therapeutics and improved the quality of life for many patients [3]. Globally, a portion of the medical community has been skeptical about the use and safety of cosmetic silicone breast implants (SBI) [4]. This is mainly due to the absence of physiologic function and the immense popularity of breast surgery worldwide, with 287,085 interventions in 2019 and 193,073 in 2020 in the United States alone [5].
New concerns regarding the use of SBI have emerged apart from infection and immune rejection [6]. Asymmetry, breast pain, capsular contracture, implant rupture, infections, and breast implant-associated anaplastic large cell lymphoma have been reported to date [7][8][7,8]. Particularly, patients have reported symptoms of new-onset autoimmune disorder (18%), depression (19%), hair loss (21%), anxiety (24%), arthralgias (25%), brain fog (25%), and fatigue (49%) after SBI surgery, leading to a new term being coined for this syndrome: breast implant illness (BII) [9][10][9,10].
2. Surgical Implications
One standard type of SBI and surgical planning cannot be used for all, and the choice is usually based on the surgeon’s experience [11][16]. Correspondingly, SBI placement involves several incision sites that appear as axillary, inframammary, periareolar, and mastectomy scars [11][12][16,17] (Figure 1). Moreover, each incision site provides different degrees of tissue manipulation [13][18].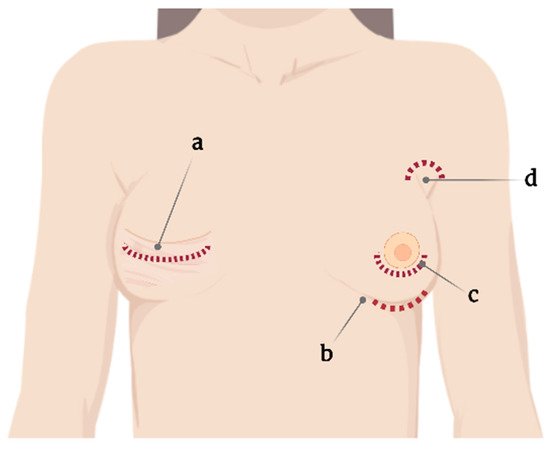
Figure 1.
Current incision sites for silicone breast implant placement. (
a
) Mastectomy scar, (
b
) submammary, (
c
) periareolar, and (
d
) axillary.
2.1. Capsular Contracture
Capsular contracture is one of the most common complications after breast implant surgery (Figure 2) [16][21]. Currently, according to Baker staging, capsular contracture can be of four degrees [17][22] and is believed to be caused by leukocytic infiltration and fibroblast proliferation around the implant [18][23]. Capsular contracture is observed in up to 20% of patients with SBI, with patients with a body mass index of >30 kg/m2 and undergoing complete breast reconstructions being at increased risk [19][20][24,25].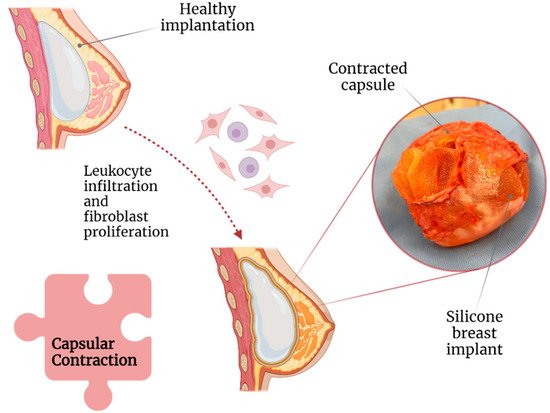
Figure 2.
Association of capsular contraction with breast implant illness.
2.2. Texture of SBI and Anaplastic Large Cell Lymphoma
Textured implants were introduced around 1970 in an attempt to reduce the incidence of capsular contracture [25][29]. Among the micropatterning techniques that were used, imprinted textured SBI has had the lowest rate of capsular contracture (3.8%) compared with foam (4.9%), salt-loss textured (5.27%), and smooth (15.5%) SBIs [27][35]. Nonetheless, compared with smooth SBI, a textured SBI has been highly associated with breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) [28][36] (Figure 3).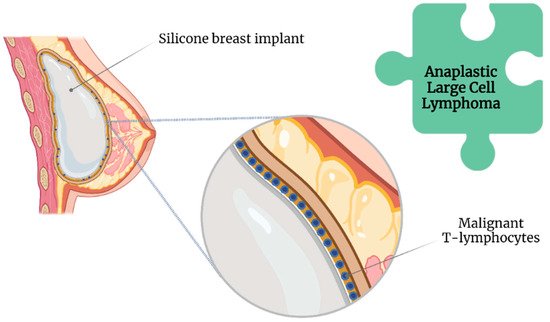
Figure 3.
Association of anaplastic large cell lymphoma with breast implant illness.
2.3. Biofilms
By definition, biofilms are colonies of one or more types of microorganisms living in symbiosis [35][36][34,43]. Unlike bacteremia, a biofilm does not present with the classic symptoms of infection as it induces a different immunological response [37][44]; this is more worrisome in the long term, as it involves chronic and significant immunological activation [38][45] unless the patient is immunosuppressed [39][46]. Biofilms further protect bacteria from host immune responses and antimicrobial therapy [40][47]. Extracellular insoluble polysaccharides secreted by microorganisms allow the adhesion of biofilms to the surface of prosthetic materials, such as SBI (Figure 4) [41][48]. However, biofilms are not exclusive to SBI [42][49].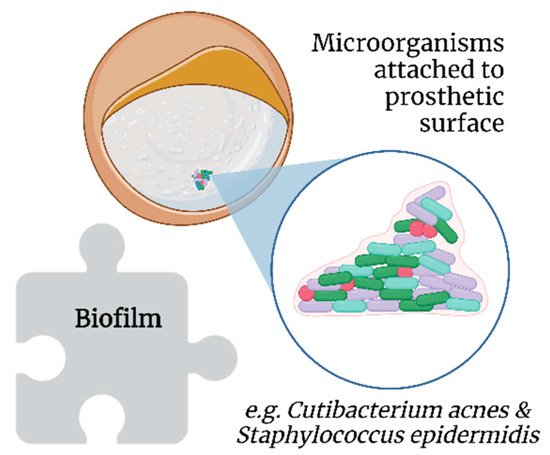
Figure 4.
Association of biofilms with breast implant illness.
2.4. Infections
As in many other circumstances, the introduction of foreign material into the body increases the risk of infection [42][49]. Specifically, infections are reported in 2.6% of SBI surgeries, predominantly because of inoculation during the surgical procedure, followed by hematogenous or contiguous spread [11][13][16,18]. Several authors have reported chronic infections in SBI capsules [16][35][48][21,34,55]. Such infections can cause capsule growth and further contraction [50][57]. Chronic infections have been posited to play a role in the genesis of breast implant-associated anaplastic large-cell lymphoma [24][51][28,58]. Patients with chronically infected capsules or synovial metaplasia reportedly have the best symptom resolution after explantation [50][57]. Notwithstanding, false-negative results account for 30% of cases in the field of SBI swab testing [52][59]. Thus, techniques such as extended culturing protocols and sonication have been suggested [53][60], which have shown 20% higher sensitivity (81% vs. 61%) and 99% specificity for bacterial detection in other prosthetic infections compared to simple culturing techniques [52][54][59,61].3. Autoimmune Responses
SBI surgery requires a specialized and highly detailed procedure that must consider certain biological aspects, including BII [19][24]. The role of autoimmune responses on the implant is a major concern associated with to BII [55][56][57][58][62,63,64,65]. Nevertheless, some authors are of the opinion that the term BII must be included with other autoimmune disorders or functional somatic syndromes [56][59][60][61][63,66,67,68].3.1. The Immune Response to SBI
Somatic syndromes are predominantly characterized by subjective symptoms rather than clinical signs by a physician, such as tissue abnormalities or specific physical findings [59][61][62][13,66,68]. Frequent patient-reported symptoms of brain fog, mood disturbances, xerophthalmia, fever, paresthesia, and arthralgia, among others, after SBI surgery have led authors to coin the term “siliconosis” or “silicone reactive disorder” [19][56][61][63][64][65][66][24,63,68,69,70,71,72]. However, other authors posit these symptoms represent a subtype of an adjuvant-induced autoimmune syndrome, a broad term that includes BII and other implant-associated diseases [56][65][63,71], termed silicone implant incompatibility syndrome (SIIS) [67][68][73,74]. SIIS is presumed to share pathophysiological features with fibromyalgia [69][75]. The nociceptive stimulus (silicone) combined with extensive worries about the safety of the SBI can lead to disturbances in pain signaling pathways, with excessive neurotransmitter stimulation resulting in systemic complaints [70][76]. Additionally, cytokines released during chronic inflammation may lead to persistent alterations in dopaminergic pathways and basal ganglia, leading to persistent anhedonia, fatigue, and psychomotor slowing [71][77]. Silicone particles can be shed from the textured implants, leading to a chronic immunological stimulus in the body [33][41] (Figure 5). This theory is supported by the findings in the lymphoid tissue and thymus related to silicone-activated inflammasomes, cytokine production, and neutrophil and macrophage recruitment, even leading to granulomas [58][72][65,78].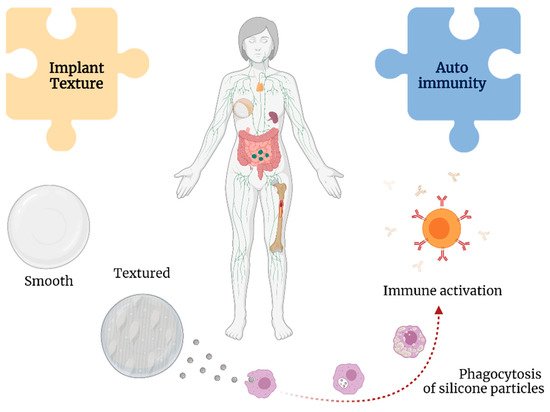
Figure 5.
Associations between implant texture and autoimmunity with breast implant illness.