Dipeptidyl peptidase 4 (DPP4) enzyme is a type II transmembrane glycoprotein, expressed ubiquitously in many tissues, including the immune cells, kidney, liver, pancreas, fat cells, and presents as a soluble form in the circulation. Dipeptidyl peptidase 4 is a serine protease, can cleave and inactivate incretin hormones, glucagon-like peptide 1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), neuropeptides, and chemokines. In addition, DPP4 has been shown to have a direct pro-inflammatory role in lymphocytes, macrophages, and smooth muscle cell.
- DPP4i
- T2DM
- GLP1
- GIP
1. Introduction
2. DPP4 and DPP4 Inhibitions in Diabetes
2.1. Mechanisms of Effect of DPP4i
Diabetes mellitus (DM) is a worldwide health problem, which is a major cause of blindness, chronic kidney disease (CKD), stroke, lower extremity amputations, coronary heart disease and heart failure (HF) [13]. T2DM has changed from a chronic disease of the elderly in the traditional concept to a chronic disease of middle-aged and even children and adolescents [14,15][14][15]. Excess body fat along with age constitute the two most important risk factors for the premature development of T2DM [15,16][15][16]. Early onset T2DM relative to late-onset disease is associated with a more rapid deterioration of β-cell function, emphasizing the importance for early diagnosis and treatment initiation [17]. Obesity-related mechanisms that are potentially linked to the severity of the disease include adipocyte lipid spillover, ectopic fat accumulation and tissue inflammation [18]. Therapies aiming to decrease body weight are consequently a valuable strategy to delay the onset and decrease the risk of T2DM, as well as managing established disease [19]. In the past few decades, drug therapy for T2DM has developed greatly and involves several new strategies [20,21,22][20][21][22]. These new strategies include more patient-friendly ways to use the drug, such as improving weight loss. However, animal studies have demonstrated that a key barrier to the development of anti-obesity drugs is the large inability to predict human cardiovascular safety [23,24,25][23][24][25]. In tolerable doses, they rarely achieve 10% weight loss. Although the clinical success of these agents has laid the foundation for a new era of anti-obesity drugs, there is considerable debate as to how GLP1/GIP regulates metabolism and whether its receptor agonists or antagonists can be the drugs of choice for treating obesity and T2DM. At present, DPP4 inhibitors are widely used for the treatment of T2DM [26,27,28,29][26][27][28][29]. The basis for this approach lies with the finding that DPP4 has a key role in determining the clearance of the incretin hormone, GLP1 [5]. GLP1 is an intestinal peptide, which was known to have a role in glucose homeostasis via actions that include the potentiation of glucose-induced insulin secretion and the suppression of glucagon secretion [30]. Dipeptidyl peptidase 4 inhibitor (DPP4i) itself has no hypoglycemic activity. Instead, their anti-hyperglycemia effect is achieved primarily by altering levels of endogenous substrates. Once the catalytic activity of DPP4 is inhibited, the levels of these substrates change. To date, GLP1 has been considered to play a major role in the therapeutic effect of DPP4i [23]. GLP1 has been shown to be a physiological DPP4 substrate [23,25][23][25]. In vivo, endogenous levels of intact, biologically active peptides increase with DPP4 inhibition and are associated with improved glucose homeostasis [31,32][31][32]. Some studies found that GLP1 receptor antagonist inhibited GLP1 signaling pathway, and the hypoglycemic effect of DPP4i decreased [33[33][34],34], thus confirming the role of GLP1 in the mechanism of action of DPP4i. It also indicates that GLP1 is not the only regulatory factor, and even in the absence of GLP1 receptor activation, the hypoglycemic activity of DPP4i is still significant [33,34][33][34]. Another physiological substrate of DPP4 is glucose-dependent insulin polypeptide (GIP), also known as incretin, and the level of GIP increases with inhibition of DPP4 activity [35,36][35][36]. Similar to GLP-1, GIP enhances insulin secretion in pancreatic beta cells in a glucose-dependent manner but appears to act in a different way on glucagon secretion [37,38][37][38]. The response to GIP was also impaired in T2DM patients. In the past, views on the possible role of GIP in the treatment of T2DM have been largely ignored, because early studies have shown that GIP′s ability to stimulate insulin secretion is severely impaired. However, in T2DM patients, further studies to explore this problem were unable to be carried out due to the lack of appropriate GIP receptor antagonists. Recent studies have shown that GIP can improve glycemic control in patients with T2DM [39,40][39][40] and have revived studies on the development of novel antagonists [41,42][41][42]. These studies have led to a re-evaluation of the role of GIP in the anti-hyperglycemia of DPP4i. In addition, GLP1′s ability to inhibit glucagon secretion is weakened when blood glucose levels drop below normal fasting levels, while GIP enhances glucagon response to hypoglycemic levels. Thus, during insulin-induced hypoglycemia, glucagon secretion is increased due to GIP use [43]. Therefore, the increase in intact GIP levels observed after inhibition of DPP4 may help maintain the counter-regulatory response of glucagon when glucose levels are controlled at hypoglycemia [44,45][44][45]. Thus, GIP′s role in improving glucagon counter-regulation may further contribute to reducing the risk of hypoglycemia associated with DPP4i. Recent studies found the direct or indirect role of soluble DPP4 in brain, gastric, liver, kidney, adipose tissue, pancreas (with islet), cardiovascular system and muscle through GLP1/GIP signaling (Figure 1). However, whether other DPP4 substrates also contribute to the therapeutic effect of DPP4i remains to be determined. In vitro, many peptide hormones and chemokines are susceptible to DPP4 cleavage when incubated with DPP4 at high concentrations [25,45][25][45]. However, there is not much evidence that they are altered in vivo by DPP4i and there have been no adverse reactions or safety issues caused by off-target effects of DPP4i on other endogenous substrates [46,47][46][47].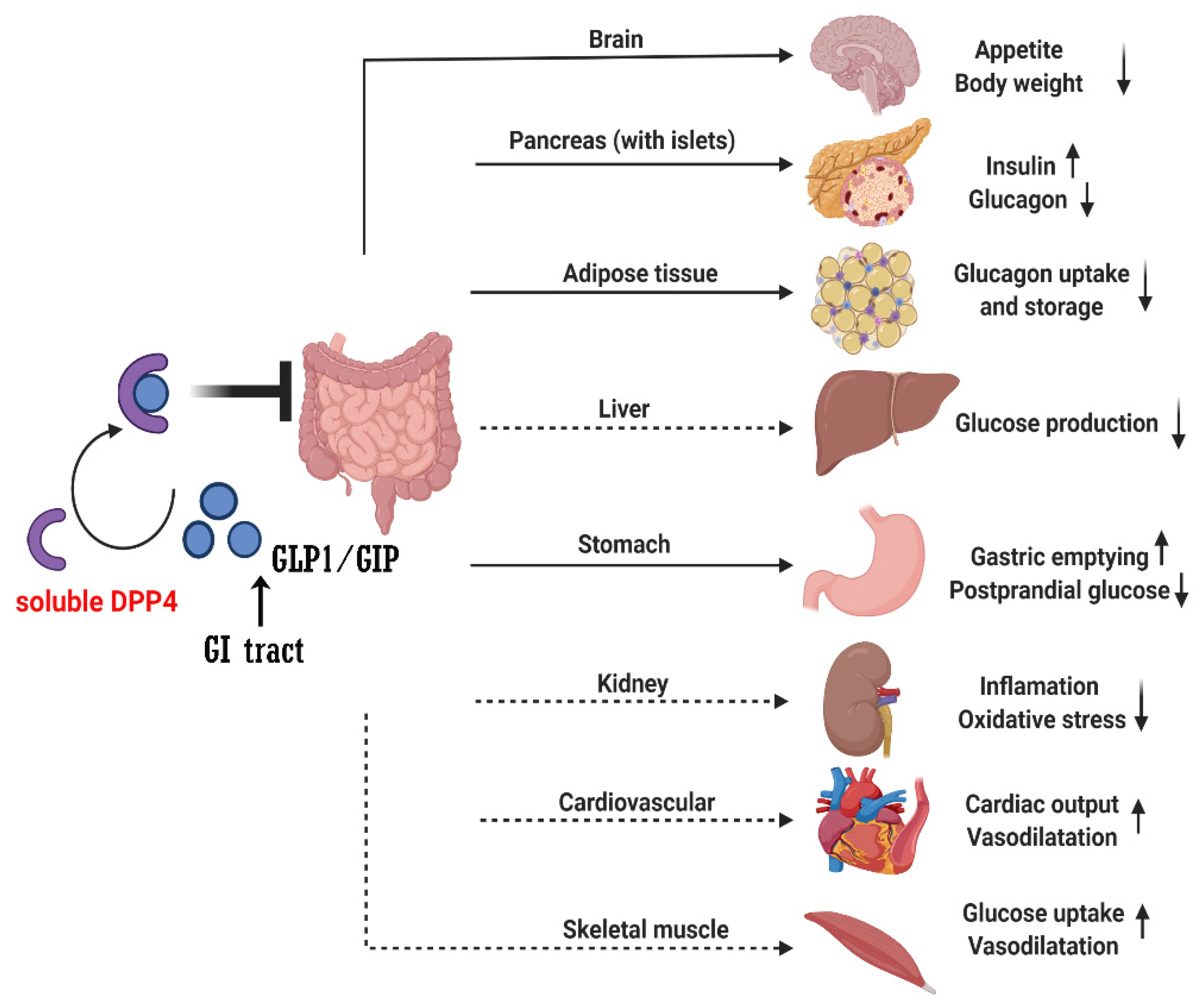
2.2. DPP4 Inhibitors
When DPP4 was identified as a therapeutic target, the search began for compounds suitable for clinical use, namely the progressive development of DPP4 inhibitors such as sitagliptin [48] and saxagliptin [49]. Currently, several structures oriented to target-specific interaction with DPP-4 are already known and officially approved by the United States Food & Drug Administration (FDA), including sitagliptin [50], saxagliptin [51], alogliptin [52], and linagliptin [53], and vildagliptin 12801240 is authorized in Europe (Table 1).|
DPP4i |
Chemistry |
Metabolism |
Half-Life |
Elimination Method |
|---|
|
DPP4i |
Trial (Year) |
Median Follow-Up, Years |
Mean/Median Age, Years |
Female (Total) |
BMI, kg/m2 * |
HbA1c, mmol/mol (%) * |
Baseline Metformin, % |
Baseline eGFR, mL/min/ [1.73 m]2 * |
Prior ASCVD, % |
Prior CHF, % |
|---|---|---|---|---|---|---|---|---|---|---|
|
Sitagliptin |
β-amino acid based |
Minimal |
||||||||
|
Sitagliptin |
|
DPP4i |
Dose (mg/Day) |
HbA1c Reduction |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
TECOS (2015) | 12.5 h |
3.0 |
Predominantly |
65 | (>80%) renal |
|||||||||
4212 | 30.2 |
55 (7.2) |
81 |
75 |
100 |
18 |
Vildagliptin |
Cyanopyrrolidine |
Hydrolysis (cytochromeindependent) to form an inactive metabolite |
~2 h | ||||
|
Sitagliptin |
100 |
0.5–1.0 | ||||||||||||
|
(14,523) | Metabolism |
(parent) and renal (metabolite) |
||||||||||||
|
Saxagliptin |
5 |
0.5–1.0 |
Saxagliptin |
Saxagliptin |
Cyanopyrrolidine |
Hydrolysis (cytochrome P450 3A4 or P450 3A5) to form an activemetabolite |
SAVOR-TIMI (2013) |
2.5 h (parent), |
2.1 |
3 h (metabolite) |
65 | |||
|
Alogliptin | Metabolism | 5590 |
31.2 |
25 (parent) and renal |
64 (8.0) |
69 |
0.6 (mean value) (metabolite) |
|||||||
73 | 78 | 13 |
Alogliptin |
Modified pyrimidinedione |
Minimal |
|||||||||
|
(16,492) | 20 h | |||||||||||||
|
Linagliptin |
5 |
0.5–0.7 | Predominantly (>70%) renal |
|||||||||||
|
Linagliptin |
Alogliptin |
Xanthine based |
EXAMINE (2013) |
Minimal |
1.5 |
~12 h (effective), >100 h (terminal) |
61 | Predominantly biliary (<6% renal) |
2.3. Benefits of DPP4i
1722 | ||||||||||
28.7 | 64 (8.0) | NA |
71 |
100 |
28 |
|||||
|
(5380) |
||||||||||
|
Linagliptin |
CARMEL (2019) |
2.2 |
66 |
2582 |
31.4 |
64 (8.0) |
54 |
55 |
57 |
27 |
NA, not available; * These are expressed as mean values.
2.4. Anti-Inflammation Effects of DPP4i
2.5. Adverse Effects
References
- Kos, K.; Baker, A.R.; Jernas, M.; Harte, A.L.; Clapham, J.C.; O’Hare, J.P.; Carlsson, L.; Kumar, S.; McTernan, P.G. DPP-IV inhibition enhances the antilipolytic action of NPY in human adipose tissue. Diabetes Obes. Metab. 2009, 11, 285–292.
- Mentlein, R. Dipeptidyl-peptidase IV (CD26)—Role in the inactivation of regulatory peptides. Regul. Pept. 1999, 85, 9–24.
- Wronkowitz, N.; Gorgens, S.W.; Romacho, T.; Villalobos, L.A.; Sanchez-Ferrer, C.F.; Peiro, C.; Sell, H.; Eckel, J. Soluble DPP4 induces inflammation and proliferation of human smooth muscle cells via protease-activated receptor 2. Biochim. Biophys. Acta 2014, 1842, 1613–1621.
- Ghorpade, D.S.; Ozcan, L.; Zheng, Z.; Nicoloro, S.M.; Shen, Y.; Chen, E.; Bluher, M.; Czech, M.P.; Tabas, I. Hepatocyte-secreted DPP4 in obesity promotes adipose inflammation and insulin resistance. Nature 2018, 555, 673–677.
- Holst, J.J.; Deacon, C.F. Inhibition of the activity of dipeptidyl-peptidase IV as a treatment for type 2 diabetes. Diabetes 1998, 47, 1663–1670.
- Ahren, B. Dipeptidyl peptidase-4 inhibitors: Clinical data and clinical implications. Diabetes Care 2007, 30, 1344–1350.
- Fan, L.; Zhou, W.; Zhang, L.; Jiang, D.; Zhao, Q.; Liu, L. Sitagliptin protects against hypoxia/reoxygenation (H/R)-induced cardiac microvascular endothelial cell injury. Am. J. Transl. Res. 2019, 11, 2099–2107.
- Kirino, Y.; Sato, Y.; Kamimoto, T.; Kawazoe, K.; Minakuchi, K.; Nakahori, Y. Interrelationship of dipeptidyl peptidase IV (DPP4) with the development of diabetes, dyslipidaemia and nephropathy: A streptozotocin-induced model using wild-type and DPP4-deficient rats. J. Endocrinol. 2009, 200, 53–61.
- Kirino, Y.; Sato, Y.; Kamimoto, T.; Kawazoe, K.; Minakuchi, K. Altered dipeptidyl peptidase-4 activity during the progression of hyperinsulinemic obesity and islet atrophy in spontaneously late-stage type 2 diabetic rats. Am. J. Physiol. Endocrinol. Metab. 2011, 300, E372–E379.
- Wang, X.; Xiang, J.; Huang, G.; Kang, L.; Yang, G.; Wu, H.; Jiang, K.; Liang, Z.; Yang, S. Inhibition of Podocytes DPP4 Activity Is a Potential Mechanism of Lobeliae Chinensis Herba in Treating Diabetic Kidney Disease. Front. Pharmacol. 2021, 12, 779652.
- Zheng, T.P.; Liu, Y.H.; Yang, L.X.; Qin, S.H.; Liu, H.B. Increased plasma dipeptidyl peptidase-4 activities are associated with high prevalence of subclinical atherosclerosis in Chinese patients with newly diagnosed type 2 diabetes: A cross-sectional study. Atherosclerosis 2015, 242, 580–588.
- Varin, E.M.; Mulvihill, E.E.; Beaudry, J.L.; Pujadas, G.; Fuchs, S.; Tanti, J.F.; Fazio, S.; Kaur, K.; Cao, X.; Baggio, L.L.; et al. Circulating Levels of Soluble Dipeptidyl Peptidase-4 Are Dissociated from Inflammation and Induced by Enzymatic DPP4 Inhibition. Cell Metab. 2019, 29, 320–334.e5.
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414.
- Chen, L.; Magliano, D.J.; Zimmet, P.Z. The worldwide epidemiology of type 2 diabetes mellitus—Present and future perspectives. Nat. Rev. Endocrinol. 2011, 8, 228–236.
- Candler, T.P.; Mahmoud, O.; Lynn, R.M.; Majbar, A.A.; Barrett, T.G.; Shield, J.P.H. Continuing rise of Type 2 diabetes incidence in children and young people in the UK. Diabet. Med. 2018, 35, 737–744.
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A.H.; Bailey, C.J.; Bellary, S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. 2018, 6, 69–80.
- Magliano, D.J.; Sacre, J.W.; Harding, J.L.; Gregg, E.W.; Zimmet, P.Z.; Shaw, J.E. Young-onset type 2 diabetes mellitus—Implications for morbidity and mortality. Nat. Rev. Endocrinol. 2020, 16, 321–331.
- Goossens, G.H.; Blaak, E.E. Adipose tissue dysfunction and impaired metabolic health in human obesity: A matter of oxygen? Front. Endocrinol. 2015, 6, 55.
- Muller, T.D.; Bluher, M.; Tschop, M.H.; DiMarchi, R.D. Anti-obesity drug discovery: Advances and challenges. Nat. Rev. Drug Discov. 2022, 21, 201–223.
- Hauser, A.S.; Attwood, M.M.; Rask-Andersen, M.; Schioth, H.B.; Gloriam, D.E. Trends in GPCR drug discovery: New agents, targets and indications. Nat. Rev. Drug Discov. 2017, 16, 829–842.
- Rask-Andersen, M.; Almen, M.S.; Schioth, H.B. Trends in the exploitation of novel drug targets. Nat. Rev. Drug Discov. 2011, 10, 579–590.
- Kaur, P.; Mittal, A.; Nayak, S.K.; Vyas, M.; Mishra, V.; Khatik, G.L. Current Strategies and Drug Targets in the Management of Type 2 Diabetes Mellitus. Curr. Drug Targets 2018, 19, 1738–1766.
- Deacon, C.F.; Hughes, T.E.; Holst, J.J. Dipeptidyl peptidase IV inhibition potentiates the insulinotropic effect of glucagon-like peptide 1 in the anesthetized pig. Diabetes 1998, 47, 764–769.
- Xiang, X.; Lang, M.; Li, Y.; Zhao, X.; Sun, H.; Jiang, W.; Ni, L.; Song, Y. Purification, identification and molecular mechanism of dipeptidyl peptidase IV inhibitory peptides from discarded shrimp (Penaeus vannamei) head. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2021, 1186, 122990.
- Mulvihill, E.E.; Drucker, D.J. Pharmacology, physiology, and mechanisms of action of dipeptidyl peptidase-4 inhibitors. Endocr. Rev. 2014, 35, 992–1019.
- Rohrborn, D.; Wronkowitz, N.; Eckel, J. DPP4 in Diabetes. Front. Immunol. 2015, 6, 386.
- Ahren, B. DPP-4 Inhibition and the Path to Clinical Proof. Front. Endocrinol. 2019, 10, 376.
- De, S.; Banerjee, S.; Kumar, S.K.A.; Paira, P. Critical Role of Dipeptidyl Peptidase IV: A Therapeutic Target for Diabetes and Cancer. Mini-Rev. Med. Chem. 2019, 19, 88–97.
- Shimizu, S.; Hosooka, T.; Matsuda, T.; Asahara, S.; Koyanagi-Kimura, M.; Kanno, A.; Bartolome, A.; Etoh, H.; Fuchita, M.; Teruyama, K.; et al. DPP4 inhibitor vildagliptin preserves beta-cell mass through amelioration of endoplasmic reticulum stress in C/EBPB transgenic mice. J. Mol. Endocrinol. 2012, 49, 125–135.
- Jonik, S.; Marchel, M.; Grabowski, M.; Opolski, G.; Mazurek, T. Gastrointestinal Incretins-Glucose-Dependent Insulinotropic Polypeptide (GIP) and Glucagon-like Peptide-1 (GLP-1) beyond Pleiotropic Physiological Effects Are Involved in Pathophysiology of Atherosclerosis and Coronary Artery Disease-State of the Art. Biology 2022, 11, 288.
- Bekiari, E.; Rizava, C.; Athanasiadou, E.; Papatheodorou, K.; Liakos, A.; Karagiannis, T.; Mainou, M.; Rika, M.; Boura, P.; Tsapas, A. Systematic review and meta-analysis of vildagliptin for treatment of type 2 diabetes. Endocrine 2016, 52, 458–480.
- Scott, L.J. Sitagliptin: A Review in Type 2 Diabetes. Drugs 2017, 77, 209–224.
- Aulinger, B.A.; Bedorf, A.; Kutscherauer, G.; de Heer, J.; Holst, J.J.; Goke, B.; Schirra, J. Defining the role of GLP-1 in the enteroinsulinar axis in type 2 diabetes using DPP-4 inhibition and GLP-1 receptor blockade. Diabetes 2014, 63, 1079–1092.
- Nauck, M.A.; Kind, J.; Kothe, L.D.; Holst, J.J.; Deacon, C.F.; Broschag, M.; He, Y.L.; Kjems, L.; Foley, J. Quantification of the Contribution of GLP-1 to Mediating Insulinotropic Effects of DPP-4 Inhibition With Vildagliptin in Healthy Subjects and Patients With Type 2 Diabetes Using Exendin as a GLP-1 Receptor Antagonist. Diabetes 2016, 65, 2440–2447.
- Sharma, A.; Paliwal, G.; Upadhyay, N.; Tiwari, A. Retraction Note: Therapeutic stimulation of GLP-1 and GIP protein with DPP-4 inhibitors for type-2 diabetes treatment. J. Diabetes Metab. Disord. 2015, 15, 34.
- Sharma, A.; Paliwal, G.; Upadhyay, N.; Tiwari, A. Therapeutic stimulation of GLP-1 and GIP protein with DPP-4 inhibitors for type-2 diabetes treatment. J. Diabetes Metab. Disord. 2015, 14, 15.
- Vilsboll, T.; Krarup, T.; Madsbad, S.; Holst, J.J. Defective amplification of the late phase insulin response to glucose by GIP in obese Type II diabetic patients. Diabetologia 2002, 45, 1111–1119.
- Mentis, N.; Vardarli, I.; Kothe, L.D.; Holst, J.J.; Deacon, C.F.; Theodorakis, M.; Meier, J.J.; Nauck, M.A. GIP does not potentiate the antidiabetic effects of GLP-1 in hyperglycemic patients with type 2 diabetes. Diabetes 2011, 60, 1270–1276.
- Hojberg, P.V.; Vilsboll, T.; Rabol, R.; Knop, F.K.; Bache, M.; Krarup, T.; Holst, J.J.; Madsbad, S. Four weeks of near-normalisation of blood glucose improves the insulin response to glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide in patients with type 2 diabetes. Diabetologia 2009, 52, 199–207.
- Aaboe, K.; Akram, S.; Deacon, C.F.; Holst, J.J.; Madsbad, S.; Krarup, T. Restoration of the insulinotropic effect of glucose-dependent insulinotropic polypeptide contributes to the antidiabetic effect of dipeptidyl peptidase-4 inhibitors. Diabetes Obes. Metab. 2015, 17, 74–81.
- Nakamura, T.; Tanimoto, H.; Okamoto, M.; Takeuchi, M.; Tsubamoto, Y.; Noda, H. GIP Receptor Antagonist, SKL-14959 Indicated Alteration of the Lipids Metabolism to Catabolism by the Inhibition of Plasma LPL Activity, Resulting in the Suppression of Weight Gain on Diets-Induced Obesity Mice. Diabetes Metab. Syndr. Obes. 2021, 14, 1095–1105.
- Gasbjerg, L.S.; Bari, E.J.; Stensen, S.; Hoe, B.; Lanng, A.R.; Mathiesen, D.S.; Christensen, M.B.; Hartmann, B.; Holst, J.J.; Rosenkilde, M.M.; et al. Dose-dependent efficacy of the glucose-dependent insulinotropic polypeptide (GIP) receptor antagonist GIP(3–30)NH2 on GIP actions in humans. Diabetes Obes. Metab. 2021, 23, 68–74.
- Christensen, M.B. Glucose-dependent insulinotropic polypeptide: Effects on insulin and glucagon secretion in humans. Dan. Med. J. 2016, 63, B5230.
- Ahren, B.; Schweizer, A.; Dejager, S.; Dunning, B.E.; Nilsson, P.M.; Persson, M.; Foley, J.E. Vildagliptin enhances islet responsiveness to both hyper- and hypoglycemia in patients with type 2 diabetes. J. Clin. Endocrinol. Metab. 2009, 94, 1236–1243.
- Farngren, J.; Persson, M.; Schweizer, A.; Foley, J.E.; Ahren, B. Glucagon dynamics during hypoglycaemia and food-re-challenge following treatment with vildagliptin in insulin-treated patients with type 2 diabetes. Diabetes Obes. Metab. 2014, 16, 812–818.
- Mannucci, E.; Nreu, B.; Montereggi, C.; Ragghianti, B.; Gallo, M.; Giaccari, A.; Monami, M.; SID-AMD Joint Panel for Italian Guidelines on Treatment of Type 2 Diabetes. Cardiovascular events and all-cause mortality in patients with type 2 diabetes treated with dipeptidyl peptidase-4 inhibitors: An extensive meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2745–2755.
- Molina-Vega, M.; Munoz-Garach, A.; Fernandez-Garcia, J.C.; Tinahones, F.J. The safety of DPP-4 inhibitor and SGLT2 inhibitor combination therapies. Expert Opin. Drug Saf. 2018, 17, 815–824.
- Biftu, T.; Feng, D.; Qian, X.; Liang, G.B.; Kieczykowski, G.; Eiermann, G.; He, H.; Leiting, B.; Lyons, K.; Petrov, A.; et al. (3R)-4--3-(2,2,2-trifluoroethyl)-1,4-diazepan-2-one, a selective dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. Bioorg. Med. Chem. Lett. 2007, 17, 49–52.
- Augeri, D.J.; Robl, J.A.; Betebenner, D.A.; Magnin, D.R.; Khanna, A.; Robertson, J.G.; Wang, A.; Simpkins, L.M.; Taunk, P.; Huang, Q.; et al. Discovery and preclinical profile of Saxagliptin (BMS-477118): A highly potent, long-acting, orally active dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. J. Med. Chem. 2005, 48, 5025–5037.
- Choy, M.; Lam, S. Sitagliptin: A novel drug for the treatment of type 2 diabetes. Cardiol. Rev. 2007, 15, 264–271.
- Thareja, S.; Aggarwal, S.; Malla, P.; Haksar, D.; Bhardwaj, T.R.; Kumar, M. Saxagliptin: A new drug for the treatment of type 2 diabetes. Mini-Rev. Med. Chem. 2010, 10, 759–765.
- White, J.R. Alogliptin for the treatment of type 2 diabetes. Drugs Today 2011, 47, 99–107.
- Aletti, R.; Cheng-Lai, A. Linagliptin: The newest dipeptidyl peptidase-4 inhibitor for type 2 diabetes mellitus. Cardiol. Rev. 2012, 20, 45–51.
- Rosenstock, J.; Perkovic, V.; Johansen, O.E.; Cooper, M.E.; Kahn, S.E.; Marx, N.; Alexander, J.H.; Pencina, M.; Toto, R.D.; Wanner, C.; et al. Effect of Linagliptin vs Placebo on Major Cardiovascular Events in Adults With Type 2 Diabetes and High Cardiovascular and Renal Risk: The CARMELINA Randomized Clinical Trial. JAMA 2019, 321, 69–79.
- Biessels, G.J.; Verhagen, C.; Janssen, J.; van den Berg, E.; Zinman, B.; Rosenstock, J.; George, J.T.; Passera, A.; Schnaidt, S.; Johansen, O.E.; et al. Effect of Linagliptin on Cognitive Performance in Patients With Type 2 Diabetes and Cardiorenal Comorbidities: The CARMELINA Randomized Trial. Diabetes Care 2019, 42, 1930–1938.
- Chikata, Y.; Iwata, H.; Miyosawa, K.; Koike, T.; Yasuda, H.; Funamizu, T.; Doi, S.; Endo, H.; Wada, H.; Naito, R.; et al. Dipeptidyl peptidase-4 inhibitors reduced long-term cardiovascular risk in diabetic patients after percutaneous coronary intervention via insulin-like growth factor-1 axis. Sci. Rep. 2022, 12, 5129.
- Carr, R.D.; Katzeff, H.L.; Alexander, C.M.; Berger, J.P.; Xu, S.S.; Thornberry, N. Reply to: Ahren, B.; Schweizer, A.; Dejager, S.; Villhauer, E.B.; Dunning, B.E.; Foley, J.E. Mechanisms of action of the dipeptidyl peptidase-4 inhibitor vildagliptin in humans. Diabetes Obes. Metab. 2011, 13, 775–783 and Ahren, B.; Schweizer, A.; Dejager, S.; Villhauer, E.B.; Dunning, B.E.; Foley, J.E. Clinical evidence and mechanistic basis for vildagliptin’s action when added to metformin. Diabetes Obes. Metab. 2011, 13, 193–203, Diabetes Obes. Metab.2012, 14, 383–384.
- Nabeno, M.; Akahoshi, F.; Kishida, H.; Miyaguchi, I.; Tanaka, Y.; Ishii, S.; Kadowaki, T. A comparative study of the binding modes of recently launched dipeptidyl peptidase IV inhibitors in the active site. Biochem. Biophys. Res. Commun. 2013, 434, 191–196.
- Tatosian, D.A.; Guo, Y.; Schaeffer, A.K.; Gaibu, N.; Popa, S.; Stoch, A.; Langdon, R.B.; Kauh, E.A. Dipeptidyl peptidase-4 inhibition in patients with type 2 diabetes treated with saxagliptin, sitagliptin, or vildagliptin. Diabetes Ther. 2013, 4, 431–442.
- Baranov, O.; Kahle, M.; Deacon, C.F.; Holst, J.J.; Nauck, M.A. Feedback suppression of meal-induced glucagon-like peptide-1 (GLP-1) secretion mediated through elevations in intact GLP-1 caused by dipeptidyl peptidase-4 inhibition: A randomized, prospective comparison of sitagliptin and vildagliptin treatment. Diabetes Obes. Metab. 2016, 18, 1100–1109.
- Alsalim, W.; Goransson, O.; Tura, A.; Pacini, G.; Mari, A.; Ahren, B. Persistent whole day meal effects of three dipeptidyl peptidase-4 inhibitors on glycaemia and hormonal responses in metformin-treated type 2 diabetes. Diabetes Obes. Metab. 2020, 22, 590–598.
- Scheen, A.J.; Charpentier, G.; Ostgren, C.J.; Hellqvist, A.; Gause-Nilsson, I. Efficacy and safety of saxagliptin in combination with metformin compared with sitagliptin in combination with metformin in adult patients with type 2 diabetes mellitus. Diabetes Metab. Res. Rev. 2010, 26, 540–549.
- Addy, C.; Tatosian, D.; Glasgow, X.S.; Gendrano, I.N., 3rd; Kauh, E.; Martucci, A.; Johnson-Levonas, A.O.; Selverian, D.; Matthews, C.Z.; Gutierrez, M.; et al. Pharmacokinetic and Pharmacodynamic Effects of Multiple-dose Administration of Omarigliptin, a Once-weekly Dipeptidyl Peptidase-4 Inhibitor, in Obese Participants With and Without Type 2 Diabetes Mellitus. Clin. Ther. 2016, 38, 516–530.
- Kim, Y.G.; Hahn, S.; Oh, T.J.; Kwak, S.H.; Park, K.S.; Cho, Y.M. Differences in the glucose-lowering efficacy of dipeptidyl peptidase-4 inhibitors between Asians and non-Asians: A systematic review and meta-analysis. Diabetologia 2013, 56, 696–708.
- Cai, X.; Han, X.; Luo, Y.; Ji, L. Efficacy of dipeptidyl-peptidase-4 inhibitors and impact on beta-cell function in Asian and Caucasian type 2 diabetes mellitus patients: A meta-analysis. J. Diabetes 2015, 7, 347–359.
- Gao, W.; Wang, Q.; Yu, S. Efficacy, safety and impact on beta-cell function of dipeptidyl peptidase-4 inhibitors plus metformin combination therapy in patients with type 2 diabetes and the difference between Asians and Caucasians: A meta-analysis. J. Endocrinol. Investig. 2016, 39, 1061–1074.
- Kozlovski, P.; Fonseca, M.; Mohan, V.; Lukashevich, V.; Odawara, M.; Paldanius, P.M.; Kothny, W. Effect of race and ethnicity on vildagliptin efficacy: A pooled analysis of phase II and III studies. Diabetes Obes. Metab. 2017, 19, 429–435.
- Klemann, C.; Wagner, L.; Stephan, M.; von Horsten, S. Cut to the chase: A review of CD26/dipeptidyl peptidase-4’s (DPP4) entanglement in the immune system. Clin. Exp. Immunol. 2016, 185, 1–21.
- Zhong, J.; Rao, X.; Deiuliis, J.; Braunstein, Z.; Narula, V.; Hazey, J.; Mikami, D.; Needleman, B.; Satoskar, A.R.; Rajagopalan, S. A potential role for dendritic cell/macrophage-expressing DPP4 in obesity-induced visceral inflammation. Diabetes 2013, 62, 149–157.
- Sitagliptin: Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/januvia-eparproduct-information_en.pdf (accessed on 1 August 2020).
- He, Y.L.; Wang, Y.; Bullock, J.M.; Deacon, C.F.; Holst, J.J.; Dunning, B.E.; Ligueros-Saylan, M.; Foley, J.E. Pharmacodynamics of vildagliptin in patients with type 2 diabetes during OGTT. J. Clin. Pharmacol. 2007, 47, 633–641.
- Christopher, R.; Covington, P.; Davenport, M.; Fleck, P.; Mekki, Q.A.; Wann, E.R.; Karim, A. Pharmacokinetics, pharmacodynamics, and tolerability of single increasing doses of the dipeptidyl peptidase-4 inhibitor alogliptin in healthy male subjects. Clin. Ther. 2008, 30, 513–527.
- Jedlowski, P.M.; Jedlowski, M.F.; Fazel, M.T. DPP-4 Inhibitors and Increased Reporting Odds of Bullous Pemphigoid: A Pharmacovigilance Study of the FDA Adverse Event Reporting System (FAERS) from 2006 to 2020. Am. J. Clin. Dermatol. 2021, 22, 891–900.
- Huang, J.; Jia, Y.; Sun, S.; Meng, L. Adverse event profiles of dipeptidyl peptidase-4 inhibitors: Data mining of the public version of the FDA adverse event reporting system. BMC Pharmacol. Toxicol. 2020, 21, 68.