In percutaneous pedicle screw (PPS) fixation of the osteoporotic spine, rigid screw fixation obtaining strong stabilization is important for achieving successful treatment outcomes. However, in patients with severe osteoporosis, it is difficult to obtain PPS fixation with sufficient stability. PPS fixation has potential disadvantages with respect to maintaining secure stabilization in comparison to conventional pedicle screw fixation. In PPS fixation, bone grafting to achieve posterior spine fusion is generally not applicable and transverse connectors between the rods cannot be used to reinforce the fixation. Various augmentation methods, including additional hooks, sublaminar bands, and hydroxyapatite (HA) sticks, are available for conventional pedicle screw fixation.
1. Introduction
In the last decade, percutaneous pedicle screw (PPS) fixation has been widely used for minimally invasive spinal surgery. PPS fixation has been performed for various surgeries to treat spinal trauma, tumors, infection, deformity, and degenerative diseases in the thoraco-lumbar spine
[1]. PPS fixation can reduce the damage of the surrounding tissues, intraoperative blood loss, postoperative pain, and recovery time in comparison to conventional pedicle screw fixation
[2][3][4][2,3,4].
Osteoporosis is becoming more common as the population ages
[5][6][5,6]. In pedicle screw fixation for osteoporotic spine, rigid screw fixation and strong stabilization are essential for achieving successful treatment outcomes. However, in osteoporotic patients, it is difficult to obtain screw fixation with sufficient stability due to bone fragility. Therefore, there are certain risk factors for screw loosening and implant failure after surgery with instrumentation for osteoporotic spine
[7][8][7,8]. Various augmentation methods have been used for conventional pedicle screw fixation in spine surgery for patients with osteoporosis, including additional hooks
[9][10][11][9,10,11], sublaminar bands
[12][13][12,13], cement augmentation
[14][15][14,15], and hydroxyapatite (HA) sticks
[16][17][16,17].
PPS fixation has potential disadvantages with respect to maintaining strong stabilization in comparison to conventional pedicle screw fixation. In PPS fixation, bone grafting to achieve posterior spine fusion is generally not applicable
[18][19][18,19]. Because of the percutaneous technique involving a small incision, transverse connectors between the rods cannot be used to reinforce the PPS fixation
[20][21][20,21]. Conventional augmentation methods, including additional hooks and sublaminar bands, are not applicable in PPS fixation. However, there has been no standardized augmentation method for PPS fixation.
Recently,
rwe
searchers developed a novel augmentation technique for PPS fixation using hydroxyapatite (HA) granules
[22]. This technique allows for the percutaneous insertion of HA granules into the screw hole along the guidewire prior to insertion of the PPS
[22][23][22,23].
RWe
searchers have used this augmentation technique for PPS fixation in various spine surgeries
[23][24][23,24]. The biomechanical analyses of
theour previous studies demonstrated that PPS fixation was significantly enhanced by augmentation with HA granules in the osteoporotic lumbar spine
[22][23][22,23]. Furthermore, augmentation with HA granules was considered to reduce the incidence of screw loosening and implant failure following PPS fixation in patients with osteoporotic spine
[22][24][25][22,24,25].
2. Surgical Procedure of Augmentation of PPS Fixation Using HA Granules
In
theour augmentation technique for PPS fixation, HA granules can be inserted percutaneously into the screw hole along the guidewire using a dedicated inserter (
Figure 1). This method has the advantage that PPS fixation can be enhanced percutaneously without compromising the minimally invasive procedure.
ResWe
archers use commercially available HA granules (porosity, 50%; particle size, 1.0–2.0 mm; Apaceram, HOYA Technosurgical Corp., Tokyo, Japan) for the augmentation (
Figure 1A)
[22][23][22,23]. Based on the results of biomechanical analyses in
theour previous studies
[22][23][22,23], at least 0.25 g of HA granules are used for the augmentation for each PPS.
ThWe
y created a dedicated device to insert the HA granules percutaneously into the screw hole in order to achieve the augmentation (
Figure 1B)
[14].
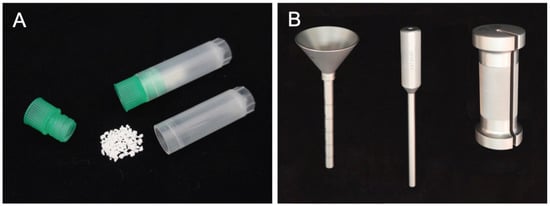
Figure 1. HA granules and the dedicated inserter for augmentation of PPS fixation. HA granules (porosity, 50%; particle size, 1–2 mm) are used for augmentation (
A). The inserter consists of a funnel-shaped external cylinder, internal cylinder, and slide hammer (
B).
The surgical procedures for the augmentation of PPS fixation are as follows (
Figure 2). First, according to the standard method of PPS insertion, the guidewire is inserted into the pedicle and posterior part of the vertebral body using a Jamshidi needle under fluoroscopic guidance. Then, the screw hole is prepared using a cannulated tap along the guidewire (
Figure 2A). Secondly, the funnel-shaped external cylinder of the insertion device is placed at the screw hole along the guidewire (
Figure 2B). Then, HA granules are inserted into the external cylinder. The tip of the inserter was set at the entry point of the screw hole so that the HA granules were mainly placed within the pedicle but not the vertebral body. Using the internal cylinder and slide hammer, the HA granules are pushed into the screw hole (
Figure 2C). The position of the tip of the guidewire must be carefully checked on a lateral fluoroscopic image in order to prevent the guidewire from penetrating the anterior wall of the vertebral body (
Figure 3). In addition, an assistant should securely grasp the proximal part of the guidewire with a Kocher forceps to prevent the guidewire from moving forward (
Figure 3). After removing the insertion device, the PPS can be inserted into the screw hole along the guidewire (
Figure 2D).
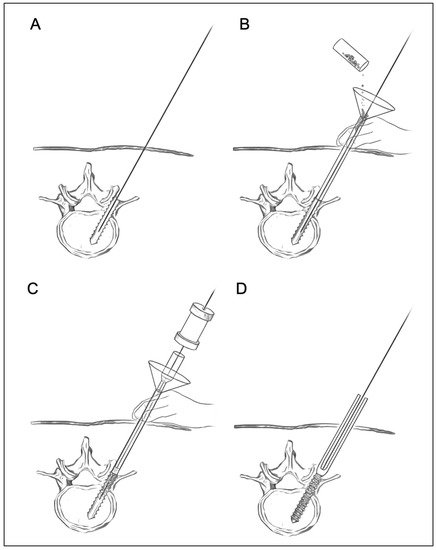
Figure 2. Surgical procedures for augmentation of PPS fixation using HA granules. A guidewire is inserted into the vertebra, and then tapping is performed (
A). The funnel-shaped external cylinder is placed at the screw hole along the guidewire. HA granules are put into the external cylinder (
B). Then, the HA granules are pushed into the screw hole using the internal cylinder and slide hammer (
C). Finally, screw insertion is performed (
D).
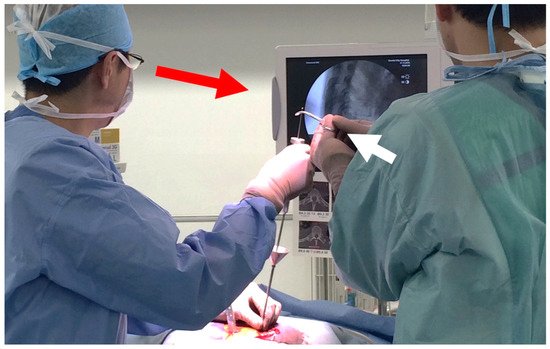
Figure 3. HA granules are pushed into the screw hole using the internal cylinder and slide hammer. The position of the tip of the guidewire must be carefully checked on a lateral fluoroscopic image in order to prevent the guidewire from penetrating the anterior wall of the vertebral body (red arrow). In addition, an assistant should grasp securely the proximal part of the guidewire with a Kocher forceps to prevent the guidewire from moving forward (white arrow).
3. Biomechanical Analysis of Augmentation of PPS Fixation Using HA Granules
Previous studies indicated that the placement of substances into the tapped screw hole increases the bone–metal interface friction force and enhances the mechanical strength of screw fixation
[16][26][27][28][29][30][31][16,26,27,28,29,30,31].
ResWe
archers previously performed a biomechanical analysis to evaluate the strength and stiffness of PPS fixation augmented with HA granules using a synthetic bone model
[22]. The results of that study demonstrated the biomechanical advantages of augmentation with HA granules for PPS fixation in the osteoporotic bone model. The study showed that the maximal insertion torque and the maximal pullout strength were significantly increased in screws with augmentation in comparison to without augmentation. Furthermore, the mechanical strength against cyclic loading was significantly greater in screws with augmentation in comparison to those without augmentation.
In another study,
reswe
archers performed a cadaveric biomechanical analysis of PPS fixation augmented with HA granules
[23]. The biomechanical performance in augmenting PPS fixation was evaluated using osteoporotic lumbar vertebrae obtained from cadavers.
TheOur results demonstrated that the augmentation using HA granules significantly increased the maximal pullout strength and maximal insertion torque of the screws placed in the osteoporotic lumbar spine. Moreover, a cyclic loading test revealed that the augmented screws achieved significantly higher mechanical strength.
These findings suggest that PPS fixation can be enhanced by augmentation with HA granules in the osteoporotic lumbar spine. PPS fixation augmented with HA granules may be helpful for decreasing the incidence of screw loosening and implant failure in patients with osteoporotic spine.