1. Piperazines
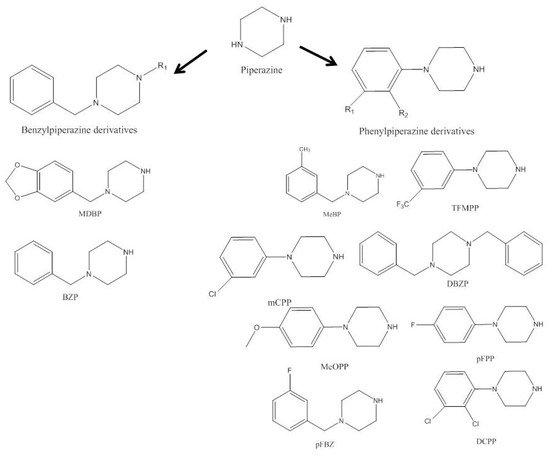
Piperazines were the first drugs of abuse deriving from phenylethylamine-based compounds. They are completely synthetic and have been widely sold as legal party pills, powder of pure substances, and adulterants due to their stimulant pharmacological properties. Piperazine (
Figure 1) is an
N-heterocyclic bioactive natural product extensively present in biologically active compounds
[1][2][3][4][13,31,32,33], and was used as anti-helminthic
[5][34].
Figure 1.
Represents the chemical structure of some of piperazines.
In the second half of the 1990s, piperazine designer drugs emerged in the illicit market, but the United States and Scandinavia were the only regions reporting high consumption rates
[2][7][13][31,35,41].
N-benzylpiperazine (BZP) was the first consumed derivative of piperazines in 1996 in the United States. It is usually combined in pills with 1-(3-trifluoromethylphenyl)piperazine (TFMPP), giving rise to the much sought-after 3,4-methylenedioxymethamphetamine (MDMA) in humans, despite being weaker in comparison
[1][7][8][13,35,36]. The appearance of new piperazines in Europe has been irregular, and the first case of piperazine abuse reported in Europe occurred in Sweden in 1999. These were not reported until 2006 by the EU Early Warning System (EWS). Subsequently to their first identification, piperazines appeared and were detected from 2005 to 2019. Only in 2004 they were considered NPS, and the EU proceeded to control their consumption in 2008
[14][42]. In England and Wales, between 2008 and 2009, deaths caused by drugs of abuse mainly involved piperazines. Currently, these compounds have spread worldwide, and around 10% of the population from developed countries has already used these types of designer drugs
[2][7][31,35]. Piperazines are among the leading deaths caused by synthetic psychoactive stimulants and hallucinogens
[15][43].
Piperazine derived drugs can be consumed as capsules, tablets, loose powders, or in liquid forms, and can also appear as adulterants of MDMA and cocaine
[1][2][7][13,31,35]. Therefore, they can enter the system through oral ingestion, nasal insufflation, injection, and smoking
[7][35].
Doses can vary between 50 and 250 mg
[3][7][32,35]. Party pills contain 28 to 133 mg of BZP, with an average level of 65 mg per tablet, even though some reports have presented this amount to be up to 1000 mg. Party tablets show a composition of 2:1 to 10:1 of BZP and TFMPP, respectively. (1-(3-chlorophenyl)piperazine) (mCPP) rounded 45 mg per pill
[16][17][18][19][44,45,46,47]. These compounds are rapidly absorbed from the gastrointestinal tract, subsequently metabolized by the liver, and finally excreted in the urine in their conjugated form. Benzyl piperazines are more stable and barely metabolized as opposed to phenyl piperazines. The latter are extensively metabolized and excreted as metabolites, making it more difficult to find the parent compound in human samples
[1][2][8][9][13,31,36,37]. They are also redistributed by different organs, such as the kidney, liver, and brain
[8][36]. It has been proposed that these compounds are metabolized in the liver by CYP2D6, CYP1A2, and CYP3A4, isoenzymes belonging to the cytochrome P450 superfamily
[7][8][35,36]. Despite these findings, recent studies have determined high concentrations of BZP, TFMPP, and mCPP in body fluids, such as blood, 24 h urine and 30 h plasma samples after the ingestion of a standard portion of 200 mg. Consequently, in overdose cases, the original drug should be detectable, even though the results might be discrepant between different subjects
[2][7][9][31,35,37].
Anita et al. determined that after consuming an average dose of BZP (200 mg) this drug showed an elimination half-life (t1/2) of 5.5 h and clearance of 99 L/h. TFMPP exhibited two half-life disposition phases, 2.04 h (±0.19 h) and 5.95 h (±1.63 h) respectively, and a clearance of 384 L/hour (±45 L/h). In turn, mCPP presented a high variability clearance (11–92 mL/h) and bioavailability (14–108%)
[7][20][21][22][35,48,49,50]. Hondebrink et al. estimated that the concentration ranges of BZP, TFMPP, and mCPP in the brain were 0.2–36 μmol/L, 22–89 μmol/L, and 1.7–85 μmol/L, respectively
[21][49].
Piperazine derivatives increase the levels of dopamine, serotonin, and noradrenaline
[3][23][32,51] by influencing their reuptake transporters (DAT, SERT, and NET, respectively)
[3][24][32,52]. These compounds are less potent than amphetamines, MDMA, and methamphetamine
[2][7][31,35].
BZP is the most studied compound
[1][3][25][13,32,53], causing motion disorders, tremors, hypertension, urinary retention, vomiting, and paranoid psychosis related to dopaminergic activity, while anxiety, insomnia, dilated pupils, dizziness, palpitations, and chest pain are due to its adrenergic properties
[1][3][26][13,32,54]. Cholinergic effects include vomiting, xerostomia, immunological disorders, hypersensitivity reactions, and pruritus
[3][26][32,54]. Lastly, serotonergic activity results in agitation, dissociation states, nausea, confusion, abdominal pain, and headaches
[3][32]. The dopaminergic effects of BZP are the increase in positive agitation, and the reaction to uncertainty decreases. TFMPP increases the emotional response
[3][27][32,55].
The combination of BZP with mCPP or TFMPP can mimic ecstasy’s characteristics, where TFMPP and mCPP act as serotoninergic agonists and BZP releases DA
[3][28][32,56]. In psychiatric practice, mCPP is used to study serotonin function showing dose-dependent effects. Piperazine derivatives also present toxic effects on cardiac cells, since they disturb Ca
2+ homeostasis, provoke adenosine triphosphate (ATP) depletion and loss of mitochondrial membrane potential, leading to cell death. Disruption of Ca
2+ homeostasis can alter heart rate
[1][2][3][13,31,32].
Besides the previously mentioned effects, piperazines can cause psychiatric disorders, such as insomnia, drowsiness, fatigue, lowered mood, tension, depression, euphoria/dysphoria, mood swings, panic, hallucinations, and withdrawal from social interactions
[1][3][23][24][26][29][30][31][32][33][13,32,51,52,54,57,58,59,60,61]. They also cause cardiovascular effects, such as increased systolic and diastolic blood pressure, tachycardia, palpitations, myocardial infarction, circulatory collapse, and prolongation of the QT interval
[3][24][26][29][30][32][33][34][35][36][37][32,52,54,57,58,60,61,62,63,64,65]. At the neurological level, they cause, dizziness, blurred vision, convulsions, epileptic seizures, increased sensitivity towards light and noise, and poor concentration
[1][3][24][26][29][30][32][33][34][38][13,32,52,54,57,58,60,61,62,66]. They cause metabolic and respiratory acidosis, hyponatremia, increases in plasma prolactin, adrenocorticotropic hormone, and cortisol
[1][3][24][26][30][33][34][13,32,52,54,58,61,62]. Dehydration and lack of appetite are symptoms at the gastrointestinal level
[1][3][24][26][29][31][32][33][34][39][40][13,32,52,54,57,59,60,61,62,67,68]. Piperazines also affect the kidney, and initiate renal failure, acute kidney injury, and affect lungs, causing hyperventilation
[1][3][24][26][30][33][34][13,32,52,54,58,61,62]. At the muscle level, the symptoms are rhabdomyolysis and muscle contractions
[3][24][26][32][32,52,54,60]. Piperazines still have other complications such as hyperthermia, abundant sweating, bruxism, and chills, and can affect the skin
[1][3][24][26][29][32][33][34][13,32,52,54,57,60,61,62]. The heaviest complications are multiple organ failure, hepatotoxicity, intravascular coagulation, serotonin syndrome, attempted suicide, nephrotoxicity requiring dialysis, malignant neoplasms, autoimmune diseases, and can lead to death
[1][3][17][23][24][26][29][30][34][41][42][43][44][13,32,45,51,52,54,57,58,62,69,70,71,72].
There is a broad age range for consumption, with young adults being the most significant consumers. There are many fatal and non-fatal reports, but some cases may have gone unnoticed since piperazines are usually not targeted in hospital toxicological analysis
[7][35]. Several non-fatal cases are shown in
Supplementary Material Table S2.
2. Aminoindanes
Aminoindanes have been investigated as research chemicals. They can act in the dilation of blood vessels, enabling strong potential for aiding in respiratory processes and thus leading to acting as strong bronchodilators. The first development regarding their research relied on these properties
[45][46][47][73,74,75].
In 1944, an animal study conducted by Levin et al. demonstrated that 2-AI and other derivatives were more effective vasodilators than
L-ephedrine, but without showing the toxicity of other amphetamines
[48][76]. In 1961 and 1963, two different research papers investigated the analgesic potential of these compounds
[49][50][77,78]. In 1973, aminoindanes were also investigated in the context of neurodegenerative diseases. Martin et al. conducted an animal study in which a few aminoindanes derivatives were tested for anti-Parkinson effects, but no evidence that they could reduce or even act on the disease’s symptoms was observed in spite of monoamine oxidase (MAO) being inhibited by some compounds
[51][79]. The MAO-B inhibition allows for a longer action of dopamine in the brain, ameliorating Parkinson’s symptoms
[52][80]. Martin et al. concluded that the biological effect of aminoindanes is directly related to the position and type of the amine substitute
[53][81].
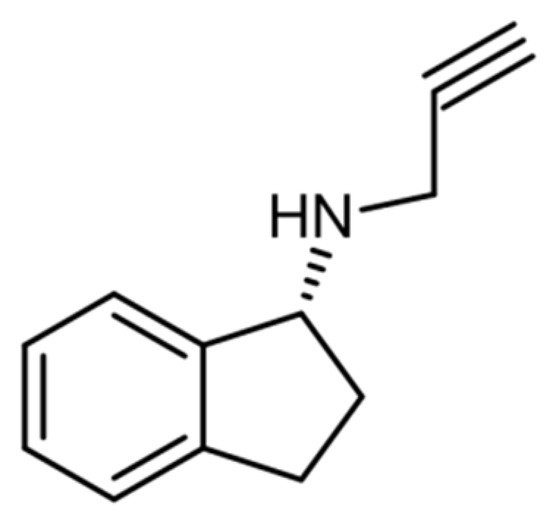
The inhibitory effect of aminoindanes on MAO-B was further investigated by Kalir et al. in 1981, leading to the identification of a strong inhibitor that did not reveal any cardiovascular or central nervous system (CNS) adverse effects. This compound was rasagiline (
Figure 2), which was used in the treatment of Parkinson’s disease
[54][82].
Figure 2.
Chemical structure of rasagiline.
Selegiline is an analog of rasagiline, its main metabolites are L-amphetamine and L-methamphetamine, whereas rasagiline does not metabolize into these compounds
[54][55][82,83].
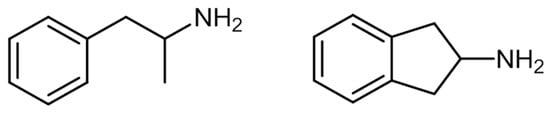
The chemical structure of aminoindanes is very similar to that of amphetamines (
Figure 3)
[56][14].
Figure 3.
Chemical structure of amphetamine (
left
) and 2-AI (
right
).
In 1986, Nichols et al. defined a group of psychoactive substances for therapeutic use featuring molecules such as MDMA, 3,4-Methylenedioxyamphetamine (MDA), and 5,6-methylenedioxy-2-aminoindane (MDAI)
[57][58][84,85]. The authors conducted a study using an animal model to understand the differences between the use of MDMA and aminoindanes, such as MDAI. The results pointed out that aminoindanes mimic the effects of MDMA and other derivatives without neurotoxicity in 5-HT receptors
[59][86]. In 2014, Simmler et al.
[28][56] performed a monoamine transporters (MATs) inhibition test on human embryonic kidney cells and concluded that MDAI, 2-AI, and 5-iodo-2-aminoindane (5-IAI) had lower inhibitory effects than MDMA.
Around 2010, and due to their similarity to amphetamines, aminoindanes emerged in the United Kingdom’s illicit drug market as a new class of NPS-synthetic aminoindanes posing as alternatives to legislated compounds from other classes
[60][87].
The ability of these compounds to mimic the effects of serotonin-releasing drugs, such as MDMA and other amphetamines, makes them effective alternatives to these drugs. Furthermore, these compounds stimulate the CNS, mediating the action of serotonin, norepinephrine, and dopamine
[61][88]. MDMA arose recent interest for the treatment of post-traumatic stress disorder
[62][89]. However, its application in other comorbid psychiatric conditions has been poorly investigated. Some studies have proven pro-cognitive effects, such as improving social connectedness and mood, increased responsiveness, and emotional sensitivity. However, other studies have also proven anti-cognitive effects
[62][89].
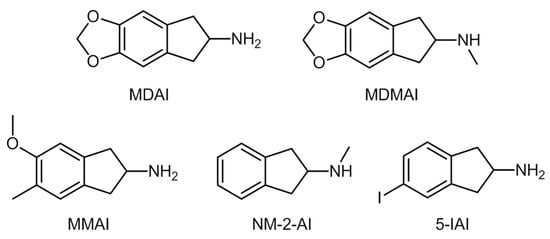
These synthetic aminoindanes derive from 2-AI (
Figure 4), some of the most common originating from structural modifications on the 2-AI precursor molecule
[61][88]. Some examples of these molecules are MDAI, 5,6-Methylenedioxy-
N-methyl-2-aminoindane (MDMAI), 5-methoxy-6-methyl-2,3-dihydro-1
H-inden-2-amine (MMAI),
N-methyl-2,3-dihydro-1
H-inden-2-amine (NM-2-AI), and 5-IAI.
Figure 4.
Chemical structures of synthetic aminoindanes.
There is still a lack of general information about these substances, mainly concerning their pharmacological effects, which makes the legislation of these compounds challenging. The UNODC reports that none of these NPS is under international control
[61][63][88,90]. In fact, until 2012, aminoindanes were the second smaller NPS group reported to the UNODC, with just 34 reported cases at a global scale against 684 of synthetic cathinones
[64][12].
Synthetic aminoindanes are usually found as powders and crystals, and are consumed through ingestion, snorting, or rectal application. No reported cases of the injection or smoking of these substances exist
[65][66][67][91,92,93]. Common street names are “
MDAI gold” or “
Pink Champagnes”, the former for MDAI-based substances and the latter for preparations containing 2-AI
[68][94].
Information on the effects and consequences of the consumption of these compounds has been found in forums of users’ experiences, such as Erowid. Some known effects are stimulation, empathy, and euphoria, while adverse effects include anxiety, depression, and tachycardia
[56][14]. Users have reported the onset of effects for these substances being about 30 min after oral consumption, and the window for maximum effect is between 45 min and 3 h after ingestion
[69][95].
Manier et al.
[47][75] investigated in vivo and in vitro metabolic pathways for 2-AI and NM-2-AI. The former is metabolized via
N-acetylation, while the latter suffers hydroxylation. The authors identified the formation of hydroxylamine in the metabolic pathway of this last compound, which can be toxic for humans or animals at high concentrations
[70][96].
Palenicek et al. in 2016
[71][97] demonstrated that MDAI (administered to rats at 10 mg/kg) was rapidly absorbed in the brain, even though the larger concentration was found in the lungs. The authors observed increased and selective neurotoxicity for this compound. Some studies on animal models stated that the intake of aminoindanes at larger doses increases neurotoxicity and body temperature, which can originate toxic conditions (for instance, serotoninergic syndrome)
[56][61][14,88].
Aminoindanes act primarily on 5-HT-receptors, and therefore stimulation is not as high as occurs when other compounds (cocaine, MDMA) are used. Thus, users consume higher doses of the compounds or mix them with other stimulant drugs, which has a potential risk of cardio- and neurotoxic conditions
[65][72][91,98].
Gallagher et al. reported in 2012 that MDAI has been linked to several toxic conditions, such as renal and hepatic failure, valvular heart disease, and respiratory distress syndrome
[73][99].
Postmortem situations related to MDAI, 5-Iodo-2-aminoindane (5-IAI), and 2-AI have been reported
[65][74][91,100], the most illustrative example being a young woman who died of cardiac arrest, showing MDAI concentrations of 26.3 mg/L
[65][91].