In excess of 75 arboviruses have been identified in Australia, some of which are now well established as causative agents of debilitating diseases. These include Ross River virus, Barmah Forest virus, and Murray Valley encephalitis virus, each of which may be detected by both antibody-based recognition and molecular typing. For most of the remaining arboviruses that may be associated with pathology in humans, routine tests are not available to diagnose infection. A number of these so-called ‘neglected’ or ‘orphan’ arboviruses are considered likely to have infected humans at a regular rate for decades. Some may be associated with undifferentiated febrile illness — fever, the cause of which is not obvious — for which around half of all cases each year remain undiagnosed. Ongoing research aims to better understand the distribution, epidemiology, and transmission ecology of these mosquito-transmitted viruses that are currently unique to Australia.
thropod-
rne
viruses (arboviruses) are by definition transmitted between vertebrate hosts by biting arthropods (mosquitoes, ticks, sandflies, midges and gnats) [1], and the infections that they cause pose a significant public health risk worldwide. The International Catalogue of Arboviruses currently lists 537 registered viruses on the basis of their known transmission by arthropods, known for potential infectivity to humans or domestic animals, and antigenic or phylogenetic relationships to known arboviruses [2].
At present, more than 130 arboviruses are recognized as causing mild to fulminant disease in humans [3]. Symptoms of uncomplicated arboviral infection generally occur between 3 and 15 days after exposure to the virus and may persist for a week or so. The most common clinical features of infection are the indistinct influenza-like symptoms of fever, headache, and malaise, which, without recourse to further information regarding a patient’s clinical and exposure history, often preclude a correct diagnosis [4].
Australia is home to over 75 arboviruses that have been isolated from its native arthropods [2]. While so far only 13 of these are found to be associated with human infection, only Barmah Forest virus (BFV) and Ross River virus (RRV) are tested for routinely in diagnostic microbiology laboratories. In a typical year, several thousand positive case notifications may now be expected nationally. Further reliable tests are less widely available for Murray Valley encephalitis virus (MVEV) and West Nile Kunjin virus (KUNV) and are infrequently requested unless for patients with highly suggestive signs and symptoms [5]. The ecology and role of other arboviruses in humans, whether they are associated with any serious infections or undiagnosed undifferentiated febrile illness (UFI), are unknown and their study is not prioritized.
It is implicitly understood that a virus that is associated with human infection could potentially be a pathogen, i.e. it may have been causing a disease, the etiology of which is so far unknown, or it could cause disease under certain circumstances, such as in immunocompromised persons, during pregnancy, or upon secondary infection. An analysis of the notifications of BFV, RRV, MVEV, and KUNV in the last two decades has clearly shown a higher distribution of these viruses in Northern Australia [6] (reviewed in [5]). This is a largely tropical climatic region where both mosquito vectors and vertebrate reservoir hosts are abundant and in which a future major expansion of a human population primarily comprising relocating, previously non-exposed individuals, is predicted.
(arboviruses) are by definition transmitted between vertebrate hosts by biting arthropods (mosquitoes, ticks, sandflies, midges and gnats) [1], and the infections that they cause pose a significant public health risk worldwide. The International Catalogue of Arboviruses currently lists 537 registered viruses on the basis of their known transmission by arthropods, known for potential infectivity to humans or domestic animals, and antigenic or phylogenetic relationships to known arboviruses [2].
At present, more than 130 arboviruses are recognized as causing mild to fulminant disease in humans [3]. Symptoms of uncomplicated arboviral infection generally occur between 3 and 15 days after exposure to the virus and may persist for a week or so. The most common clinical features of infection are the indistinct influenza-like symptoms of fever, headache, and malaise, which, without recourse to further information regarding a patient’s clinical and exposure history, often preclude a correct diagnosis [4].
Australia is home to over 75 arboviruses that have been isolated from its native arthropods [2]. While so far only 13 of these are found to be associated with human infection, only Barmah Forest virus (BFV) and Ross River virus (RRV) are tested for routinely in diagnostic microbiology laboratories. In a typical year, several thousand positive case notifications may now be expected nationally. Further reliable tests are less widely available for Murray Valley encephalitis virus (MVEV) and West Nile Kunjin virus (KUNV) and are infrequently requested unless for patients with highly suggestive signs and symptoms [5]. The ecology and role of other arboviruses in humans, whether they are associated with any serious infections or undiagnosed undifferentiated febrile illness (UFI), are unknown and their study is not prioritized.
It is implicitly understood that a virus that is associated with human infection could potentially be a pathogen, i.e. it may have been causing a disease, the etiology of which is so far unknown, or it could cause disease under certain circumstances, such as in immunocompromised persons, during pregnancy, or upon secondary infection. An analysis of the notifications of BFV, RRV, MVEV, and KUNV in the last two decades has clearly shown a higher distribution of these viruses in Northern Australia [6] (reviewed in [5]). This is a largely tropical climatic region where both mosquito vectors and vertebrate reservoir hosts are abundant and in which a future major expansion of a human population primarily comprising relocating, previously non-exposed individuals, is predicted.
2. Arbovirus Ecology and Epidemiology
Most arboviruses studied thus far are transmitted in zoonotic cycles, i.e. the principal vertebrate host is an animal other than human [7]. The distribution of an arbovirus is restricted to areas inhabited by vertebrate hosts that serve as its reservoirs and vectors. Thus, many arboviruses have clearly defined ecological zones, while some, distributed globally, cause diseases of considerable public health and veterinary importance (reviewed in [8]). Examples of the latter include dengue (worldwide, approximately between the Tropics of Cancer and Capricorn), yellow fever (Africa and South America), Japanese encephalitis (eastern and southeast Asia and Australia), West Nile encephalitis (North America, Europe and the Middle East), chikungunya (Asia, Central and South America, parts of the Pacific), eastern and western equine encephalitis (North America), and Venezuelan equine encephalitis (South America). Due to focal, global, environmental, societal and/or demographic changes, many of these viruses have either emerged or re-emerged in the first years of this century [9,10,11].
Notably, the non-segmented, positive-strand RNA viruses belonging to the genus
Most arboviruses studied thus far are transmitted in zoonotic cycles, i.e. the principal vertebrate host is an animal other than human [7]. The distribution of an arbovirus is restricted to areas inhabited by vertebrate hosts that serve as its reservoirs and vectors. Thus, many arboviruses have clearly defined ecological zones, while some, distributed globally, cause diseases of considerable public health and veterinary importance (reviewed in [8]). Examples of the latter include dengue (worldwide, approximately between the Tropics of Cancer and Capricorn), yellow fever (Africa and South America), Japanese encephalitis (eastern and southeast Asia and Australia), West Nile encephalitis (North America, Europe and the Middle East), chikungunya (Asia, Central and South America, parts of the Pacific), eastern and western equine encephalitis (North America), and Venezuelan equine encephalitis (South America). Due to focal, global, environmental, societal and/or demographic changes, many of these viruses have either emerged or re-emerged in the first years of this century [9][10][11].
Notably, the non-segmented, positive-strand RNA viruses belonging to the genus , are the etiological agents of several major global infectious diseases such as dengue, yellow fever, chikungunya and Zika. Other related pathogens belong to the segmented, negative strand RNA
genus. The vast majority of arbovirus-associated epidemics occur in the tropics and subtropics due to the prevailing hot and humid climate which is conducive to the habitation of vector mosquitoes, including members of
genera [12]. To this growing list of real or potential public health threats posed by arboviruses Mayarocan now be added, identified recently in the Amazon and other tropical regions of South America [13]. The issue of whether neglected Australian arboviruses similarly present an emerging, hitherto unrecognized challenge to humans is a subject of continuing discussion.
3. Arboviruses in Australia
Australia is the sixth largest country in the world by area, the largest country without land borders, and the largest country overall in the southern hemisphere. Early European settlement, urbanization, increased sea and air travel and trade, globalization, pathogen evolution, and elevated mean global temperature are some of the factors that may have influenced the introduction and expanded geographical reach of infectious diseases, including those caused by arboviruses, in Australia [14]. Furthermore, Australia spans tropical and subtropical latitudes, where arboviruses have access to an abundant source of both reservoir hosts and vectors.
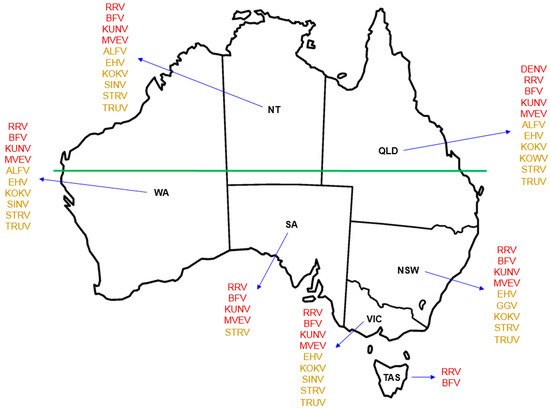
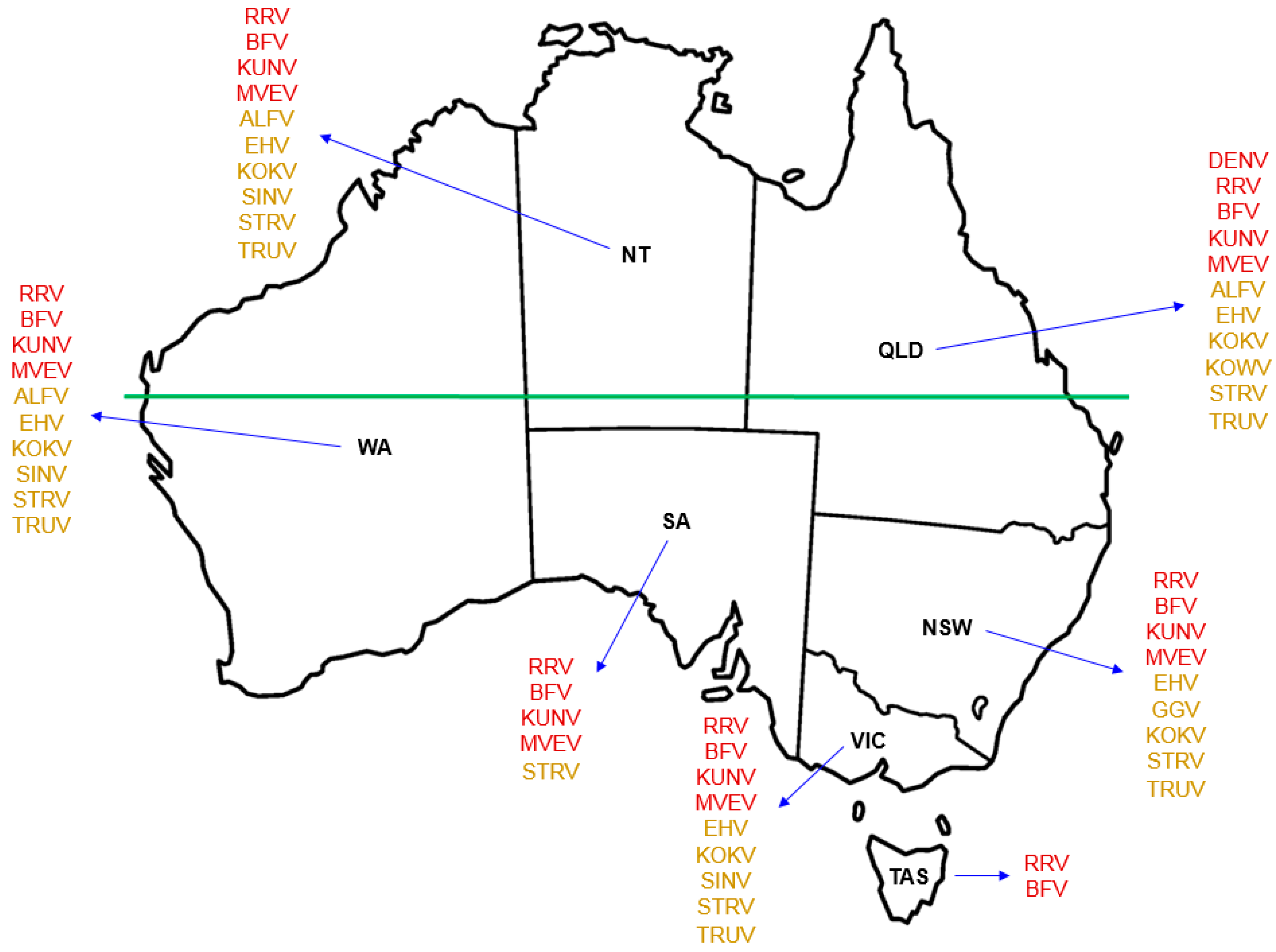
While only 13 of the more than 75 identified arboviruses indigenous to Australia are currently known to cause disease in humans, information is scarce as to the potential human pathogenicity of most others [15]. Of those that are recognized to cause infection in humans in Australia ( Figure 1), the alphaviruses RRV and BFV are the most well-known, infection with either of which triggers an incapacitating and occasionally chronic polyarthritis with accompanying myalgia and lethargy [16,17]. The flaviviruses MVEV and KUNV cause encephalitis, an acute inflammation of the brain [18].
), the alphaviruses RRV and BFV are the most well-known, infection with either of which triggers an incapacitating and occasionally chronic polyarthritis with accompanying myalgia and lethargy [16][17]. The flaviviruses MVEV and KUNV cause encephalitis, an acute inflammation of the brain [18].
Geographical distribution of Australian indigenous arboviruses known to cause human infection. Use of red font for each named virus indicates the state or territory from which that virus is known to be recovered and the notifiable disease for which it is listed in the Australian National Notifiable Disease Surveillance System (ANNDSS). Use of amber font for each named virus indicates the reported recovery of that virus from mosquitoes during mosquito surveillance but that the corresponding virus-associated disease is not currently recorded in the ANNDSS. Named arboviruses: ALFV — Alfuy; BFV — Barmah Forest; DENV — Dengue; EHV — Edge Hill; GGV — Gan Gan; KOKV — Kokobera; KOWV — Kowanyama; KUNV — Kunjin; MVEV — Murray Valley encephalitis; RRV — Ross River; SINV — Sindbis; STRV — Stratford; Trubanaman — TRUV. The land mass above the horizontal green line, which marks the southern edge of the Pilbara Range (latitude 24° S, just south of the Tropic of Capricorn, 23.52° S), approximates to the region termed Northern Australia. States and territory: NSW — New South Wales; NT — Northern Territory; QLD — Queensland; SA — South Australia; TAS — Tasmania; VIC — Victoria; WA- — Western Australia.
Infection with the flavivirus dengue (DENV) is typically characterized by a febrile illness but a small proportion of cases manifest as a life-threatening hemorrhagic fever or shock syndrome (reviewed in [19]). DENV may be acquired outside Australia and brought back by returning travelers, a significant proportion of whom are hospitalized with unrecognized warning signs of severe disease. As intercontinental travel from Australia, particularly to Asia, continues to increase, in order to avert serious outcomes it is crucial that clinicians anticipate, and can recognize and manage, such tropical infectious diseases. While DENV has a trans-global distribution, local outbreaks are also reported regularly in far north Queensland, with foci in the vicinities of Cairns and Townsville [20], where it is well recognized by the resident population as a not insignificant threat to their health [21].
Several other arboviruses that are indigenous to Australia ( Figure 1), such as the alphavirus Sindbis (SINV), the flaviviruses Alfuy (ALFV), Edge Hill (EHV), Kokobera (KOKV) and Stratford (STRV), and the orthobunyaviruses Gan Gan (GGV), Kowanyama (KOWV) and Trubanaman (TRUV), are recognized through eliciting mild symptoms of febrile illness, corroborated by detection of serum antibodies to viral antigens, as being able to infect humans [17,22,23] (reviewed in [5]). There are occasional reports of human disease caused by SINV, EHV and KOKV [24,25,26], but these are not currently included individually in the list of Australian national notifiable diseases by disease type [27]. The magnitude of each of these arboviral infections raises the question as to what is an appropriate threshold for recording cases for the purposes of annual notification at state/territory and national levels. SINV is reportedly the arbovirus most frequently isolated from mosquitoes in Australia [23], but as an alphavirus it does not come under the ‘flavivirus infection (unspecified)’ umbrella presently used for nationwide notification [27].
Other arboviruses have been isolated from arthropods in the Australia-Pacific region [15]. These include the newly identified Bamaga (BGV) and Fitzroy River (FRV) flaviviruses [28,29], which are closely related to the disease-causing yellow fever virus (YFV) and EHV, but for each of which there is scant information about its capacity to infect humans or to cause disease in humans. ), such as the alphavirus Sindbis (SINV), the flaviviruses Alfuy (ALFV), Edge Hill (EHV), Kokobera (KOKV) and Stratford (STRV), and the orthobunyaviruses Gan Gan (GGV), Kowanyama (KOWV) and Trubanaman (TRUV), are recognized through eliciting mild symptoms of febrile illness, corroborated by detection of serum antibodies to viral antigens, as being able to infect humans [17][22][23] (reviewed in [5]). There are occasional reports of human disease caused by SINV, EHV and KOKV [24][25][26], but these are not currently included individually in the list of Australian national notifiable diseases by disease type [27]. The magnitude of each of these arboviral infections raises the question as to what is an appropriate threshold for recording cases for the purposes of annual notification at state/territory and national levels. SINV is reportedly the arbovirus most frequently isolated from mosquitoes in Australia [23], but as an alphavirus it does not come under the ‘flavivirus infection (unspecified)’ umbrella presently used for nationwide notification [27].
Other arboviruses have been isolated from arthropods in the Australia-Pacific region [15]. These include the newly identified Bamaga (BGV) and Fitzroy River (FRV) flaviviruses [28][29], which are closely related to the disease-causing yellow fever virus (YFV) and EHV, but for each of which there is scant information about its capacity to infect humans or to cause disease in humans.
4. Transmission Cycles of Australian Arboviruses
Over several decades, many arboviruses have been identified in Australian mosquitoes, ticks, and biting midges [5,15]. Little is known about their transmission cycles, their pathogenicity for humans, or their potential to cause epidemics. Although large marsupials such as kangaroos and wallabies are considered potential reservoirs for RRV [58,59] and BFV [59,60], and water birds such as herons and egrets are regarded as hosts for MVEV, ALFV and SINV [61,62], there are many other arboviruses whose relationship with reservoirs and vectors, and their role in human infections or diseases, are yet to be defined.
While the epidemiology of these arboviruses is poorly understood, it is likely that they are maintained in zoonotic cycles rather than by human-to-human transmission. It may be that these neglected viruses are harbored by apathogenic, persistent infections in native Australian reservoir mammals and birds, with occasional spillover into humans [5].
Over several decades, many arboviruses have been identified in Australian mosquitoes, ticks, and biting midges [5][15]. Little is known about their transmission cycles, their pathogenicity for humans, or their potential to cause epidemics. Although large marsupials such as kangaroos and wallabies are considered potential reservoirs for RRV [30][31] and BFV [31][32], and water birds such as herons and egrets are regarded as hosts for MVEV, ALFV and SINV [33][34], there are many other arboviruses whose relationship with reservoirs and vectors, and their role in human infections or diseases, are yet to be defined.
While the epidemiology of these arboviruses is poorly understood, it is likely that they are maintained in zoonotic cycles rather than by human-to-human transmission. It may be that these neglected viruses are harbored by apathogenic, persistent infections in native Australian reservoir mammals and birds, with occasional spillover into humans [5].
Although the presence of vectors does not necessarily mean the emergence of human pathogens, sudden climatic and environmental variations [69][35], including high rainfall, more frequent cyclones and resultant increased intensity of flooding, contribute to favorable breeding conditions for mosquito species that are especially well-suited to maintaining arboviruses of potential public health importance [66][36].