Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Amina Yu and Version 1 by Ananth Nag Ramaseri Chandra.
Cybersickness is a form of simulation sickness experienced when using head mounted displays (HMDs) and is a critical issue that needs to be addressed before virtual reality technology is widely accepted. The concept of cybersickness has existed since the early stages of VR system development. ThCybersis work compiles details onckness is a type of simulation sickness and its types, such as cybersickness; causes; theories that explain simulation sickness, guidelines on how to minimize or avoid these issuesthat is experienced in virtual reality.
- virtual reality (VR)
- virtual environment
- simulation sickness
- cybersickness
- head mounted displays (HMDs)
- usability
- design
- user
1. Introduction
Alternative reality creation and interaction requires a different set of capabilities. Modern developments in software and hardware technologies have unlocked new prospects for interactions. Virtual reality (VR) allows for three-dimensional visualization with immersive and interactive features [1]. A soaring interest in virtual reality (VR) technology has increased integration into numerous disciplines such as education, games, and training [2]. A report from artillery intelligence in 2021 states that approximately 23% of US households have access to a virtual reality headset [3]. A Goldman Sachs report on understanding the future of technologies predicts that VR and AR software will become a $35 billion industry by 2025 [4]. Advancements in VR technology have significant shortcomings. Virtual reality tools are known to have adverse physiological and psychological consequences, [5] such as simulation sickness, a type of motion sickness induced by mobile simulators without head tracking [6].
Cybersickness is a form of simulation sickness experienced when using head mounted displays (HMDs) and is a critical issue that needs to be addressed before virtual reality technology is widely accepted. The concept of cybersickness has existed since the early stages of VR system development. However, it was referred to as motion sickness. A combination of symptoms such as nausea, fatigue, headache, strain, postural instability, and vomiting define cybersickness [7], which is a possible consequence of the intense visual and motion cuing when experiencing a virtual environment [8]. Previous research states that approximately 20–80% of virtual reality users have experienced cybersickness or related discomfort at least once [9]. Cybersickness is measured through simulation sickness questionnaires and physiological measurements such as heart rate, postural sway, and galvanic skin response.
Usability, or ease of use, is essential when developing immersive VR applications. Fatigue, space limitation, predictability, and accessibility are usability issues associated with virtual reality content [10]. Cybersickness also limits the overall usability of a VR system [7]. Researchers that study virtual reality, human computer interaction (HCI), and organizations focused on VR have been thriving since they focus on minimizing cybersickness and improving the usability of virtual environments [11,12]. We have focused on simulation sickness in virtual reality environments for this review. Virtual reality offers remarkable opportunities for research and development. Minimizing cybersickness is vital for greater virtual reality application acceptance. Existing research on sickness in virtual reality systems focuses on individual aspects, such as causes, factors, relationships between factors, and cybersickness.
Cybersickness can be a result of software, hardware, or other environmental factors. The motivation for this work is to compile details on simulation sickness and its types, such as cybersickness; causes; theories that explain simulation sickness, such as poison theory and postural instability theory; factors causing simulation sickness; and guidelines on how to minimize or avoid these issues. The identified factors that contribute to simulation sickness are classified according to user, display type, VR content type, and virtual environment design. We have identified and grouped guidelines for users and virtual reality content developers. We attempt to offer insight into existing research on factors and guidelines aimed at minimizing simulation sickness.
2. Simulation Sickness in Virtual Environments—Cybersickness
Virtual reality systems provide an immersive experience with the help of high-resolution displays, spatial sound, and interactive devices. However, interactive environments have shortcomings that contribute to physiological effects and threaten the usability of the virtual reality environment.
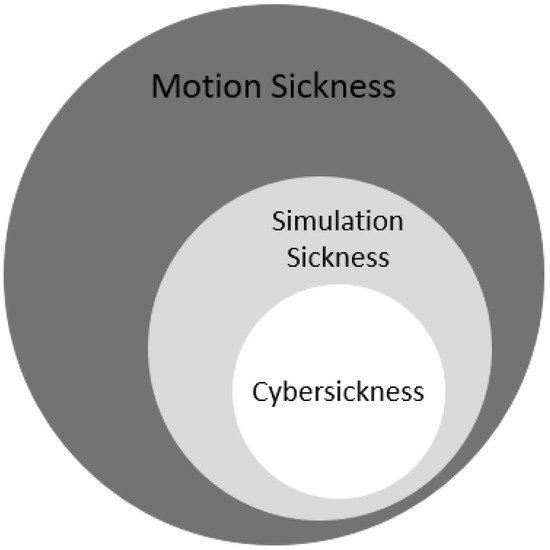
Simulation sickness is a condition that can result in headaches, dizziness, eye strain, disorientation, vertigo, loss of skin color, nausea, and vomiting. This condition, which can appear while using simulators or virtual reality devices, is comparable to motion sickness, though it is technically different. Figure 2. depicts the clear distinction between motion sickness, simulation sickness, and cybersickness.
Previous research, dating back to early 2000s, does not denote or consider advancements in virtual reality and other simulation technologies [32]. Another kind of sickness, more similar to simulation sickness or motion sickness is induced when using a VR system, denoted as virtual reality induced symptoms and effects (VRISE) [15], visually induced motion sickness (VIMS), or cybersickness [12].
Cybersickness is a significant issue that prevents the functional use of fully immersive virtual reality systems. It is a form of motion sickness and is one of the primary health and safety concerns of virtual environments, posing a severe threat to usability and performance [33]. Some of the issues associated with virtual reality systems are assumed to result from poor system design, including virtual scene and user control strategies, technical deficiencies such as image distortions, visual cues, and individual user susceptibility. Some human factors that limit performance also contribute to the reduced popularity of virtual reality systems [34].
2.1. Cause of Sickness—Theories
The occurrence of simulation sickness has been a topic of research since the early 19th century. The earliest theories addressing simulation sickness were based on cerebral anemia, which is deprived blood supply to the brain, or cerebral hyperemia, which is the congestion of blood in the brain and spinal cord. These studies advanced significantly during the post-World War II era. Vestibular and sensory conflict are some of the earliest theories that focus on simulation sickness [35]. Simulation sickness is the result of the difference between the information received by the vestibular and the visual systems in a virtual environment, according to sensory conflict theory [35]. There is a significant mismatch when the visual information specifies movement while the vestibular system indicates that the user is stationary due to the conflict between the sensory inputs, causing the user to experience simulation sickness. Postural instability theory states that extended periods of postural instability cause motion sickness symptoms, the level of which is directly proportional to the duration [36]. Poison theory states that the feeling of nausea caused by simulation sickness is the body’s response to the mismatch of visual and vestibular information. The body assumes it is suffering from food poisoning and triggers the sensation of the need to vomit, or similar sensations [37]. All of these theories, including eye movement, subjective vertical mismatch, and negative reinforcement models, describe the cause of motion sickness that occurs when using virtual reality systems. However, the most widely accepted is sensory conflict theory [34].
2.2. Cybersickness as a Usability Issue
Virtual reality creates an opportunity to visualize an altered three-dimensional world. However, it requires full sensory awareness for maximum effectiveness. Interactions and visual cues in virtual environments must be well designed to be as close to the real world as possible before VR is understood and adapted well. The extent to which the user feels present in the environment indicates its success. Therefore, usability issues will diminish the sense of presence in a virtual environment. Users will not be able to experience the reality of a virtual environment if they struggle to use the environment. D. Geszten et al. [38] suggests that presence and copresence should be the primary goals when designing VR environments and should be examined when evaluating the usability of these environments.
3. Factors Contributing to Cybersickness
Many potential factors contribute to simulation sickness in virtual environments, such as age, gender, calibration, experience, and application type. P.J Costello [5] has tabulated many of these factors based on the individual, simulator type, and task performed. These factors have a profound impact on the severity of cybersickness. The factors affecting virtual reality are classified according to user, design, display types, and type of VR content.
3.1. Users
3.1.1. Age
Cybersickness is primarily based on sensory conflict theory and postural in-stability theory. Literature suggests that younger people are more resistant to simulation sickness [32]. Vestibular perceptual threshold, the weakest stimulus detected, diminishes in humans after the age of 40, making them more susceptible to simulation sickness [39]. Era et al. reported that there were postural balance differences between young and middle-aged test participants. In addition, higher age groups experience diminished postural balance which may lead to sickness [40].
3.1.2. Gender
Simulation sickness may vary according to gender with the use of HMDs. Schafer et al. [41] studied the role of gender, technology, and their potential contribution towards simulation sickness. Using the data obtained from about 223 individuals (108 male and 115 female) they examined the levels of simulation sickness with regards to gender, sensory conflict, and improvements in VR technology. They concluded that women experienced a higher level of simulation sickness compared to men. Stanney et al. [42] conducted multiple experiments and found that females were equally susceptible to motion sickness, and it was due to the improper fit of the VR headset to inter-pupillary distance (distance between the center of one’s eyes). They also suggest a redesign to the VR headsets with alterable inter-pupillary distance to reduce the cybersickness in women.
3.1.3. Exposure
Stanney et al. [43] concluded that an increase in exposure time was directly proportional to the severity of adverse symptoms. Users vulnerable to motion sickness can experience approximately twice the intensity compared to non-susceptible individuals. Users who experience nausea during carnival rides can also expect unpleasant symptoms. Exposing an individual to virtual environments briefly and stopping the encounter before or while experiencing sickness then retrying in a day or two will help the user adapt to the virtual environment. Recurring exposure to virtual environments may lower or eliminate simulation sickness. However, using a virtual environment for longer durations is not recommended [32].
3.1.4. Control
User control and navigation are substantial contributing factors to simulation sickness since input devices, such as data gloves, keyboards, and mice, can be used to control the virtual environment. Greater environmental control may reduce illness and allow users to expect a reaction after an action is performed [15]. Saredakis et al. [44] observed that physical navigation, such as walking, reduces symptoms compared to navigating through controllers.
3.2. Displays
A difference in environments, such as desktop VR, large curved screen displays, or HMD’s can have a varied impact on the level of sickness [15].
3.2.1. Head Mounted Display (HMD)
Factors such as contrast, illumination, exposure duration, and working distance contribute to straining the visual system when working with head mounted displays. Approximately 60% of users reported symptoms such as visual strain, nausea, and headache, while 20% reported a reduction in binocular visual perception when using a stereoscopic HMD, such as EyePhone LX, in an immersive virtual environment for a ten-minute duration [45]. Similar symptoms were experienced by 61% of users after twenty minutes of exposure to immersive virtual content from a DVisor HMD [46]. Technical advancements in VR display hardware, comparing Oculus VR DK1 to Oculus VR DK2, for example, did not have a significant impact on decreased cybersickness [41]. Some symptoms are more likely to occur in virtual environments. However. sensory conflict contributes significantly to nausea and other symptoms. Body motion, head movement-initiated disorientation, and incorrect optical design resulted in strain-producing ocular symptoms. Recent contributions from Tong et al. [47] determined that HMD use caused a higher level of motion sickness compared to stereoscopic desktop displays. Some users enjoyed a higher level of immersion in an HMD. However, they could not sustain the experience for longer periods.
3.2.2. Large and Desktop Displays
Former investigations report that viewing time, viewing distance, and lighting may also contribute to simulation sickness [48,49]. The optimum viewing distance is 65 cm. Swindells et al. concluded that large displays improve a sense of presence, but they do not directly impact or induce simulation sickness [50].
3.3. VR Content Type
3.3.1. Immersion
Guna et al. studied the impact of virtual content type on simulation sickness. They noticed that the type of video content, immersive vs. non-immersive, is a critical factor for virtual environment usability. Video content type influenced the contributor’s sensitivity to simulation sickness and physiology. Their conclusion was based on the results of a simulation sickness questionnaire and other physiological measures. The lowest simulation sickness questionnaire score was recorded for non-immersive virtual content displayed on a television screen, while the highest scores were reported on an HMD with immersive content [51].
3.3.2. Graphic Realism
Chang et al. investigated the results of rendering realistic scenes. Participants who experienced realistic graphic content were prone to a higher level of simulation sickness. The authors also suspect that a sensory discrepancy between the vestibular and visual systems may cause a higher level of discomfort [2].
3.3.3. Field of View
Field of view (FOV) is the maximum visual angle of the virtual environment display. It is the visual range of the virtual world through the HMD or other display device. Altering the FOV of a display manually or dynamically significantly reduces user discomfort during swift and rotating movements [2,8].
3.4. Design
The virtual reality (VR) environment is a rapidly emerging technique for simulating real-world applications. Examples of successful application domains include training, therapy, and design. Simulating realistic features that support a wide range of activities is difficult, even with recent developments. Designing and executing virtual environments with a high degree of similarity to the real world is a significant challenge since human interactions are highly associated with sensory information. Minimal training is needed for interacting when the simulated system is close to natural, which correlates well to the system’s usability. Sustaining realism in the simulated world has its benefits. However, if the virtual environment is far from real, there is a need for remarkable visual patterns based on the application environment. Virtual reality, by definition, comprises immersive environments that use multi-modal inputs, such as haptic, visual, and speech, and outputs, such as HMD’s and other displays, to create a maximum presence for the user. Designing complex virtual environments is a delicate task since it requires managing hardware, general user safety, and visual content that may cause disorientation or sickness. The design process for desktop VR environments is straightforward. However, the presence it draws is minimal and is less effective in tasks that include physical interaction [52].
4. Guidelines to Minimize Simulation Sickness
Hardware improvements improve the usability of virtual environments [53], and existing research suggests that some techniques used to achieve maximum usability can minimize simulation sickness [54]. Virtual reality hardware manufacturers, such as Oculus and HTC, have detailed design guidelines for content developers and hardware safety guidelines for users [55].
4.1. Design
It is impossible to have an ideal set of guidelines for any software system. However, we have summarized some critical ones from existing research, that must be considered when designing virtual environments to reduce simulation sickness symptoms.
4.1.1. Latency and Frame Rate
Latency is the delay between the user and visual reaction in a virtual environment display. Frame rate is a measure of how quickly the frames pass through the rendering pipeline. A drop in frame rate can occur in a VR application with complex graphics. There is a high chance of experiencing simulation sickness if the latency between the user input and virtual content output is high [54]. The minimum recommended latency is 20 milliseconds: anything higher than 46 milliseconds can induce motion sickness. Companies such as Oculus, Sony, and Steam emphasize the importance of virtual content with low latency, responsiveness, and high frame rates for higher virtual content quality [32,56].
4.1.2. Movement
The VR’s user does not always control character movements. This movement unavailability can cause serious issues. Therefore, movement in a virtual environment should be realistic to match sensory expectations. Inappropriate movements, such as fast tilting, rolling, and waveform motion, should be avoided. Examples of these inappropriate movements include gun sway, head bob, and going up and down stairs. Porcino et al. [54] suggest that including movements based on jumps instead of continuous walks may minimize sickness. Uncontrolled user movement outputs should be limited, such as flipping, falling, or zoom transitions [32].
4.1.3. Flicker
Flicker is the brightness fluctuation on video displays and can cause sickness in a VR environment. This fluctuation is visually disturbing and affects the health of the user’s eyes. The user is more likely to experience flicker in the edges of the screen when using larger displays. Flicker avoidance is essential for HMDs with a brighter screen and high refresh rate [2,32].
4.1.4. Rapid Changes in Acceleration and Deceleration
A vital factor in virtual environment discomfort is accelerated movement. Sensory conflicts that cause discrepancies occur due to sudden increased or decreased acceleration. Therefore, increasing or decreasing acceleration slowly would result in a pleasant user experience [54]. Rapidly zoomed movements should also be avoided, such as when the visual cones move faster than expected when a user’s view is zoomed in [32].
4.1.5. Sensory Support
A user might experience higher VR immersion and expect relevant vestibular in- formation after exposure to strong illusions. The system can cause motion sickness if the VR system cannot provide suitable sensory input [8]. Therefore, designing a logical environment in which the players can focus and bind to is essential. The user interface elements should be fixed rather than floating, creating an environment with a clear, steady horizon and reference points that users can focus on to minimize sickness. A world with imbalanced or changing backgrounds should be avoided. Designing a virtual world that supports human sensory systems is ideal [32].
4.1.6. Field of View (FOV)
A wide field of view (FOV) in a display may increase immersion in the virtual environment. Narrow field of views may affect the presence in the virtual environment, which is an important characteristic. Displays with a broader field of view increase the occurrence of simulation sickness more than those with a narrow field of view [8]. The edges of a display with a narrow field of view reduce the simulation view, which reduces the feeling of movement [54].
4.1.7. Length of Exposure
Longer duration of exposure can increase discomfort levels. Applications should be designed to support shorter exposure duration to allow users to pause, rest, and continue later. Optimal application design would include automatic suggestions to the user that encourage regular breaks [54]. There should be provisions for the user to come back and continue from the same stage in the application if they are getting sick and leave the session. Therefore, shorter exposure sessions are beneficial [2,32].
4.2. User
Every user is unique and has individual characteristics and those play a vital role in the way they experience cybersickness. Based on the existing research and some guidelines provided by virtual reality hardware and software organizations users can minimize cybersickness by following best practices.
4.2.1. Duration
Using a virtual environment for longer duration improves the chance of experiencing cybersickness. Using these environments for a shorter duration or taking breaks during longer sessions may reduce nausea during or after exposure [32,55].
4.2.2. Focus
Human brains focus on a fixed point in space outside of a virtual environment. VR confuses the brain since the fixed point in space looks farther, but the image on the headset screen is immediately in front of the eyes. Focusing on an object on the VR scene’s horizon may reduce sickness symptoms [32,57].
4.2.3. Environment
Cybersickness symptoms strengthen in surroundings with high temperature and poor ventilation. Good airflow and ventilation can prevent nausea or support recovery after experiencing dizziness [32].
4.2.4. Physical Health
All of the user’s senses must be optimal to achieve an elevated presence level. Users should be physically healthy and have good balance for the best virtual reality experience. If a user has a cold, headache, or hangover, it is better to avoid a virtual environment since their symptoms may worsen [54]. The guidelines mentioned above will only minimize simulation sickness symptoms and improve the usability of the VR systems. These suggestions will not eliminate the symptoms [32,54]. In Table 6, a combination of guidelines is tabulated.
1. Introduction
Alternative reality creation and interaction requires a different set of capabilities. Modern developments in software and hardware technologies have unlocked new prospects for interactions. Virtual reality (VR) allows for three-dimensional visualization with immersive and interactive features [1]. A soaring interest in virtual reality (VR) technology has increased integration into numerous disciplines such as education, games, and training [2]. From artillery intelligence in 2021 states that approximately 23% of US households have access to a virtual reality headset [3]. A Goldman Sachs report on understanding the future of technologies predicts that VR and AR software will become a $35 billion industry by 2025 [4]. Advancements in VR technology have significant shortcomings. Virtual reality tools are known to have adverse physiological and psychological consequences, [5] such as simulation sickness, a type of motion sickness induced by mobile simulators without head tracking [6].
Cybersickness is a form of simulation sickness experienced when using head mounted displays (HMDs) and is a critical issue that needs to be addressed before virtual reality technology is widely accepted. The concept of cybersickness has existed since the early stages of VR system development. However, it was referred to as motion sickness. A combination of symptoms such as nausea, fatigue, headache, strain, postural instability, and vomiting define cybersickness [7], which is a possible consequence of the intense visual and motion cuing when experiencing a virtual environment [8]. Previous research states that approximately 20–80% of virtual reality users have experienced cybersickness or related discomfort at least once [9]. Cybersickness is measured through simulation sickness questionnaires and physiological measurements such as heart rate, postural sway, and galvanic skin response.
Usability, or ease of use, is essential when developing immersive VR applications. Fatigue, space limitation, predictability, and accessibility are usability issues associated with virtual reality content [10]. Cybersickness also limits the overall usability of a VR system [7]. Researchers that focus on virtual reality, human computer interaction (HCI), and organizations focused on VR have been thriving since they focus on minimizing cybersickness and improving the usability of virtual environments [11][12]. It has focused on simulation sickness in virtual reality environments. Virtual reality offers remarkable opportunities for development. Minimizing cybersickness is vital for greater virtual reality application acceptance. Existing research on sickness in virtual reality systems focuses on individual aspects, such as causes, factors, relationships between factors, and cybersickness.
Cybersickness can be a result of software, hardware, or other environmental factors. The motivation is to compile details on simulation sickness and its types, such as cybersickness; causes; theories that explain simulation sickness, such as poison theory and postural instability theory; factors causing simulation sickness; and guidelines on how to minimize or avoid these issues. The identified factors that contribute to simulation sickness are classified according to user, display type, VR content type, and virtual environment design. It was identified and grouped that guidelines for users and virtual reality content developers. It was attempted to offer insight into existing research on factors and guidelines aimed at minimizing simulation sickness.