Translational research made with Cannabis sativa L. and its biocompounds provides data for some targeted diseases, as also symptoms associated with Autism Spectrum Disorders (ASDs). The main compounds ∆9-tetrahydrocannabinol (THC) and cannabidiol (CBD), are capable of modulating the endocannabinoid system since its dysregulation interferes with the pathophysiology of ASDs there are clinical evidence for its potential use in the treatment of the disease. Conventional therapy still has limitations, as it does not always treat the central symptoms, and there are many patients who do not respond to treatment, which demands more research on new therapies. Through the analysis of published literature on this topic, it is verified that cannabinoids, in particular CBD, improves symptoms associated with common comorbidities in ASDs. Some studies also demonstrate the therapeutic potential of these compounds in the treatment of central symptoms of autism. In addition, cannabinoid therapy to ASDs is associated with low adverse effects and a reduction in concomitant medication.
- cannabinoids
- cannabidiol
- clinical trial
- anxiety
- FAAH
- social interaction
- inflammation
- gamma-aminobutyric acid
- glutamate
- neuroimaging
1. Introduction
2. Cannabis, Flos
2. Cannabis, Flos
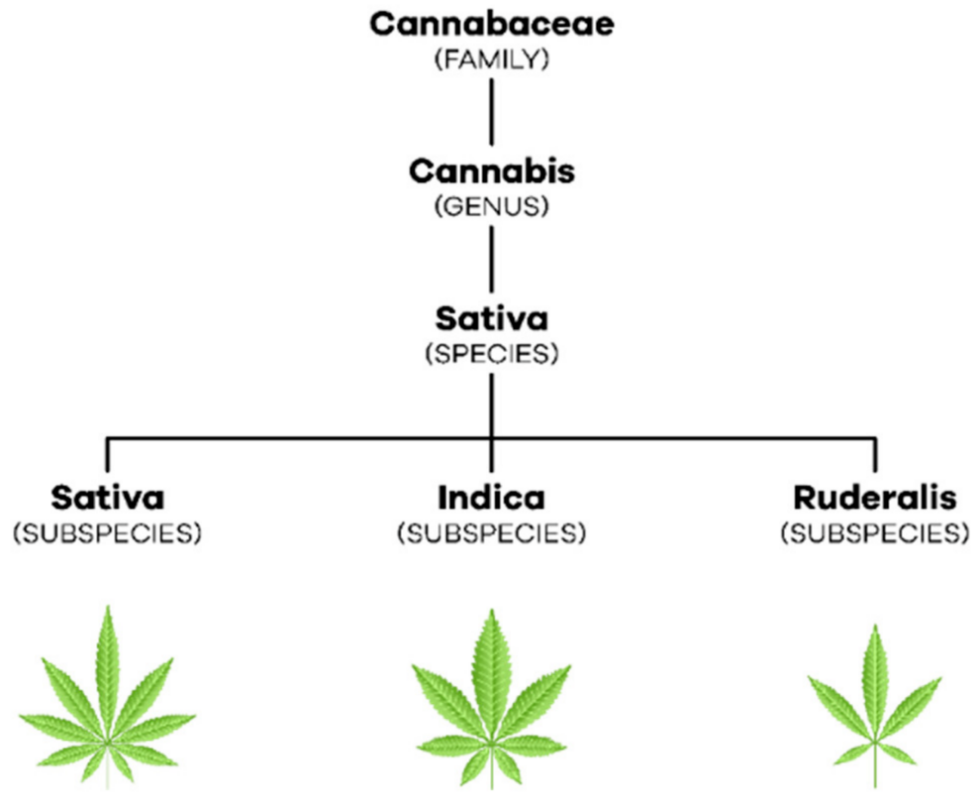
To date, a monograph of the drug “Cannabis, flos” is not available in the European Pharmacopoeia but it is largely followed by the one in German Pharmacopoeia, where it is defined as “dried shoot apices of female Cannabis sativa L. (Cannabaceae) plants. The drug contains not less than 90.0 and not more than 110.0 percent of cannabinoid quantities indicated in the label, such as ∆9-tetrahydrocannabinol and cannabidiol, as well as cannabinoid-carbon acids, such as ∆9-tetrahydrocannabinolic acid and cannabidiolic acid, calculated as ∆9-tetrahydrocannabinol (C21H30O2; Mr 314.5) and cannabidiol (C21H30O2; Mr 314.5), referenced to dried drug” [10]. Cannabis is a dioecious annual plant [3] (p. 304) that belongs to the Cannabaceae family, which includes about 170 species [11] (pp. 203–204). With regard to taxonomy, in 1753, Linnaeus began by describing only one species of this plant, Cannabis sativa. Later, in 1785, Lamarck considered the existence of two species of cannabis, Cannabis sativa, which came from the West, and Cannabis indica, which came from India, Southeast Asia, and Southern Africa ([2][11] (p. 236), (pp. 207–208)). Only in the 19th century emerged the reference to a new species of cannabis, Cannabis ruderalis [2] (p. 236). Currently, most authors consider that there is only one species, C. sativa L., which comprises three subspecies, C. sativa subsp. sativa, C. sativa subsp. indica and C. sativa subsp. ruderalis [12] (p. 3) (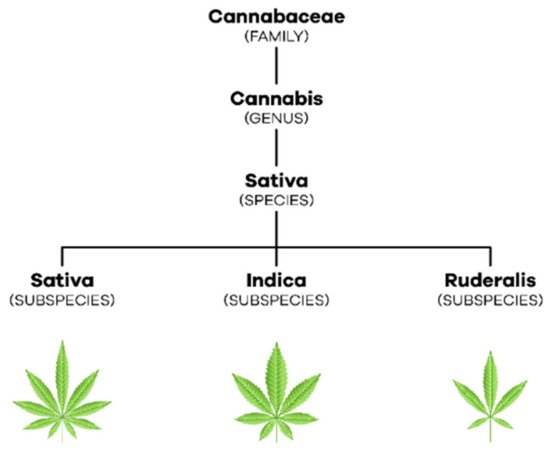
3. Endocannabinoid System
3.1. Cannabinoid Receptors
3.2. Endocannabinoids
3. Endocannabinoid System
The endocannabinoid system is involved in the organism’s homeostasis [1] (p.413) through the modulation of multiple organs comprising the cardiovascular (CVS), central nervous (CNS), peripheral nervous (PNS), endocrine, reproductive, immune and digestive systems ([15][16] (p. 2) (p. 554)).3.1. Cannabinoid Receptors
The two main receptors of the endocannabinoid system are the cannabinoid receptor type 1 (CB1), encoded by the CNR1 gene which is made with 472 amino acids, and the cannabinoid receptor type 2 (CB2), encoded by the CNR2 gel and composed of 360 amino acids [17] (p. 2). Both are G protein-coupled metabotropic receptors ([18][19] (p. 2), (p. 3)) and their expression varies depending on the body region [16] (p. 559). The CB1 receptor is found mainly in CNS neurons with high expression density in the basal ganglia, cerebral cortex, hippocampus, and cerebellum [17] (p. 5). Thus, it is involved in motor control, cognitive functions, movement coordination, learning, and memory. It is also expressed in PNS and peripheral tissues, namely, in sympathetic nerve terminals, gastrointestinal tract, lungs, musculoskeletal tissue, reproductive and immune system, among others [16] (p. 559). Furthermore, its hepatic and cardiovascular expression increases in the presence of pathological conditions [17] (p. 5). In turn, the CB2 receptor is mostly found in peripheral cells of the immune system [20] (p. 1140) such as the spleen, tonsils, and thymus [16] (p. 559). It is also expressed in lower concentrations in the pancreas, liver, bone marrow, bones, and skin [21] (p. 3). At the cerebral level, it is found in low amounts, however, in inflammatory states, its expression increases both in microglia and in other glial cells [3] (p. 309).3.2. Endocannabinoids
The most studied endocannabinoids are N-arachidonylethanolamine or anandamide (AEA) and 2-arachidonylglycerol (2-AG) [3] (p. 308). AEA is known to be a high-affinity partial agonist for the CB1 receptor and with very low affinity for the CB2 receptor, while 2-AG is a full agonist with low to moderate affinity for the two cannabinoid receptors [17] (p. 2). Neurotransmission in the postsynaptic neuron leads to an increase in intracellular calcium and, consequently, to the production of endocannabinoids from their lipid precursors [22] (p. 4). AEA is produced from N-acyl-phosphatidylethanolamine (NAPE) by N-acyl-phosphatidylethanolamine-specific phospholipase D (NAPE-PLD) while 2-AG is formed from diacylglycerol (DAG) by diacylglycerol lipase (DAGL) [19] (p. 3). As lipid molecules, they are able to cross the plasma membrane and travel in a retrograde direction to the presynaptic terminals [17] (p. 4). There, the endocannabinoids bind and activate cannabinoid receptors, which, in turn, inhibit the adenylate cyclase (AC) enzyme, decreasing the formation of cyclic adenosine monophosphate (cAMP) and the activation of protein kinase A (PKA) [18] (pp. 2–3). Thus, hyperpolarization occurs by opening potassium channels, the consequent closure of calcium channels, and the release of neurotransmitters ceases [22] (p. 4). The endocannabinoids get retaken by the membrane transporter of endocannabinoids and then hydrolyzed by the respective enzymes [23] (pp. 2–3). AEA is catabolized by fatty acid amide hydrolase (FAAH), giving rise to AA and ethanolamine while 2-AG is catabolized by monoacylglycerol lipase (MAGL) giving rise to AA and glycerol ([3][22] (p. 308), (p. 4)) (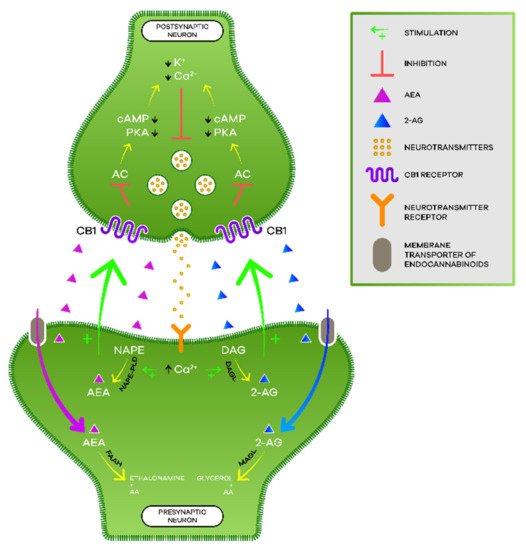

3.3. Phytocannabinoids
3.3. Phytocannabinoids
Phytocannabinoids are biosynthesized in C. sativa L. and, currently, there are more than 100 phytocannabinoids identified among the more than 500 compounds discovered in this plant. Its distribution is variable but phytocannabinoids accumulate, in large quantities, in the trichomes present in female flowers as previously referred to in this text [3] (p. 305). Among them, THC and CBD are the most studied ones. The structures are in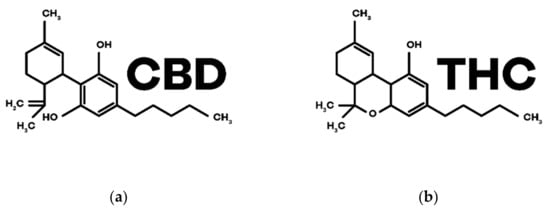
4. Physiological and Therapeutic Effects of Cannabinoids
4. Physiological and Therapeutic Effects of Cannabinoids
The endocannabinoid system is associated with the balance of homeostasis and, as cannabinoids interact with this system, they have been studied, in recent decades, for the treatment of various pathologies (| Diseases and Symptoms | Therapeutic Potential of Cannabinoids |
|---|---|
| Alzheimer’s Disease | Anti-inflammatory Neuroprotector Antioxidant |
| Parkinson’s Disease | |
| Huntington’s Disease | |
| Multiple Sclerosis | Antispastic Analgesic |
| Epilepsy | Anticonvulsant |
| Tourette’s Syndrome | Improvement of symptomatology |
| Cancer | Analgesic Antiemetic Appetite stimulator Antitumor |
| Glaucoma | Intraocular pression reduction |
| Inflammatory Bowel Diseases | Anti-inflammatory Healing |
| Schizophrenia | Antipsychotic |
| Sleep Disorders | Decrease sleep latency and nocturnal awakenings Sedative |
| Pain | Analgesic |
| Post-Traumatic Stress Disorder | Anxiolytic |
| Nausea and Vomiting | Antiemetic |
| Anorexia | Appetite stimulator |