Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Conner Chen and Version 5 by Conner Chen.
Diagnosis and quantification of ischemia in ocular burns is essential to determine the need for interventions in the acute phase and the final prognosis. Clinical signs in isolation are rarely sufficient to accurately assess limbal ischemia. With anterior segment optical coherence tomography angiography (AS-OCTA), the presence and extent of ischemia can be objectively confirmed and quantified.
- optical coherence tomography
- angiography
- anterior segment OCT
- Corneal angiography
- Ocular burns
- limbal ischemia
1. Introduction
Ocular burns can present with a myriad of clinical manifestations in the acute phase. The grade of injury and the extent of ocular structures involved often determines the type and severity of the chronic sequelae that ensue. Limbal stem cell deficiency (LSCD) is one such chronic feature that can cause significant visual morbidity due to the corneal scarring and vascularization that occurs in its end stages [1]. The development of this pathology is usually heralded by the presence of limbal ischemia in the acute phase of the disease [2]. The detection and grading of this finding can help identify those individuals who are at a higher risk of developing LSCD. This cohort of patients can then be subjected to regular monitoring which will facilitate early identification and treatment of LSCD to prevent its complications and restore visual function.
However, the diagnosis of ischemia in the acute phase is based on subjective clinical findings which are often difficult to discern in an inflamed eye [2]. Thus, the adoption of diagnostic tools can provide an objective method of confirming ischemia of the limbal vasculature and assessing its progression. An anterior segment optical coherence tomography (AS-OCT) is usually available in most anterior segment practices and provides rapid, high-definition images of sections of the cornea with relative ease [3]. The utility of its angiography feature (AS-OCTA) has recently been explored to detect ischemia in acute burns as it can provide a real time in-vivo image of the limbal and perilimbal vasculature [4][5][4,5]. The use of image processing software has also aided in objectively quantifying the degree of vascular changes observed [6].
2. Principle and Technology of Optical Coherence Tomography Angiography (OCTA)
2.1. Principle
2.1. Principle
2.2. Technology
2.2. Technology
3. Comparison with Fluorescein Angiography (FA) and Indocyanine Green Angiography (ICG)
The most important factor that sets OCTA apart from its counterpart vessel-imaging modalities is its non-invasive nature as it is not dependent on the use of a dye [21][22][21,22]. This obviates the injection-associated trauma and dye-associated risks such as nausea, vomiting, and, rarely, anaphylaxis [23][24][23,24]. By avoiding the use of an external dye, the time taken for the angiography is significantly decreased with the use of OCTA which is especially desirable in patients with painful disorders such as acute burns. The test can be repeated multiple times without any need for recurrent dye injections. Additionally, the ischemic zones may be obscured by leakage of the dye from the inflamed vessels in these eyes and this disadvantage is circumvented with OCTA [25]. The use of light in the infrared wavelength by the OCTA provides an added advantage as the device can image vessels beneath hemorrhages from superficial conjunctival vessels [6][26][6,26]. This is of particular significance in eyes with acute burns as these traumatic sub-conjunctival hemorrhages (SCH) are common and may mask areas of ischemia when viewed via conventional angiographic techniques. However, shadow artifacts can also be seen in AS-OCTA images due to these hemorrhages. This contrast has been depicted in Figure 1 where in the inferior area the vasculature is obscured by the SCH. At the same time in the region abutting the inferior limbus, the vasculature is clear despite the presence of the SCH. One possible explanation for this discrepancy can be the relative position of the SCH when compared to the vessels. Very superficial and large hemorrhages may block the view of all the underlying vessels as opposed to deeper SCH which may allow the imaging of vessels overlying the hemorrhage.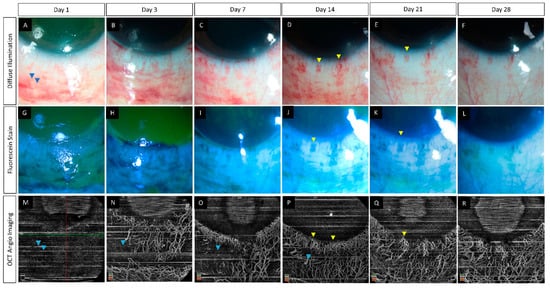
Figure 1. (A–R) Serial monitoring with slit lamp photographs (without and with fluorescein staining) along with anterior segment optical coherence tomography angiography (AS-OCTA) imaging in an eye with acute chemical burns. (A–L) These images show the progressive healing of the corneal and conjunctival epithelial defects in the inferior part of the eye which is complete by day 7. (M–R) AS-OCTA images show a blocked signal in the initial three visits due to the subconjunctival hemorrhages inferiorly (blue arrow heads) with clear delineation of the vasculature following the resolution of the hemorrhages. The hemorrhages abutting the limbus, however, have not affected the vascular signal (yellow arrow heads).