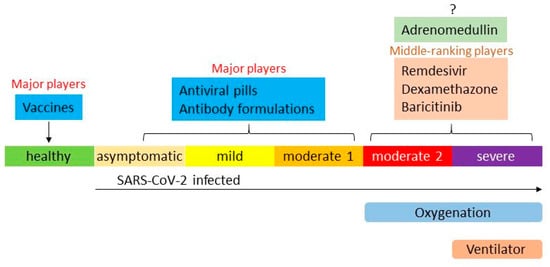
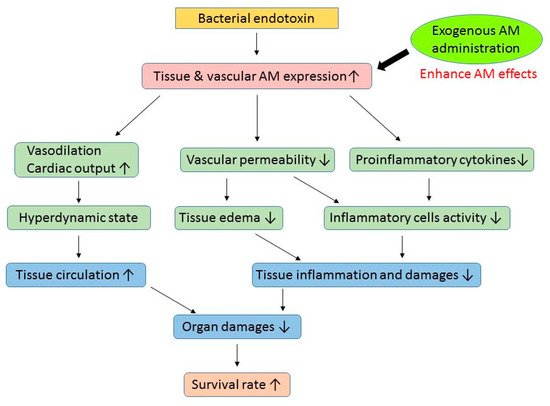
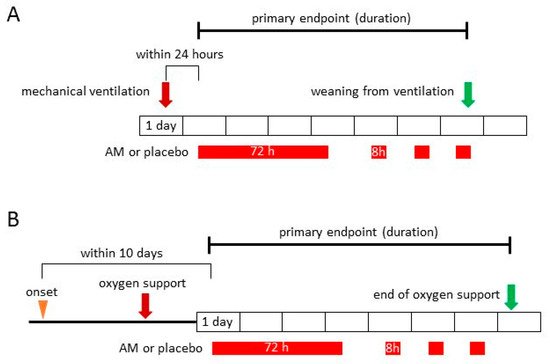
The COVID-19 pandemic is still in progress, and a significant number of patients have presented with severe illness. Recently introduced vaccines, antiviral medicines, and antibody formulations can suppress COVID-19 symptoms and decrease the number of patients exhibiting severe disease. However, complete avoidance of severe COVID-19 has not been achieved and there are insufficient methods to treat it. Adrenomedullin (AM) is an endogenous peptide that maintains vascular tone and endothelial barrier function. The AM plasma level is markedly increased during severe inflammatory disorders, such as sepsis, pneumonia, and COVID-19, and associated with its prognosis. Exogenous AM administration reduced inflammation and related organ damage in rodent models. The results strongly suggest that AM could be an alternative therapy for COVID-19. Researchers are currently conducting an investigator-initiated phase 2a trial for moderate to severe COVID-19 using AM.
The COVID-19 pandemic is still in progress, and a significant number of patients have presented with severe illness. Recently introduced vaccines, antiviral medicines, and antibody formulations can suppress COVID-19 symptoms and decrease the number of patients exhibiting severe disease. However, complete avoidance of severe COVID-19 has not been achieved and there are insufficient methods to treat it. Adrenomedullin (AM) is an endogenous peptide that maintains vascular tone and endothelial barrier function. The AM plasma level is markedly increased during severe inflammatory disorders, such as sepsis, pneumonia, and COVID-19, and associated with its prognosis. Exogenous AM administration reduced inflammation and related organ damage in rodent models. The results strongly suggest that AM could be an alternative therapy for COVID-19. We are currently conducting an investigator-initiated phase 2a trial for moderate to severe COVID-19 using AM.
- adrenomedullin
- translational study
- clinical trial
- COVID-19
- pneumonia
1. Introduction
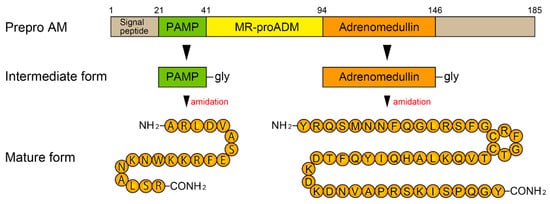
2. Biosynthesis of AM and Its Receptors
3. AM and Sepsis
| Genetic Intervention | |||
| Animal | Procedure | Results | Reference |
| Mouse | AM-deficient (+/−) + LPS-endotoxemia |
compared to WT mice · ↑ mortality · ↑ liver dysfunction |
[58] |
| Mouse | AM-deficient (+/−) + LPS-endotoxemia |
compared to WT mice · ↑ TNF-α, IL-1β · ↑ liver dysfunction |
[59] |
| Mouse | AM transgenic + LPS-endotoxemia |
compared to WT mice · ↓ BP decline · ↓ organ damage · ↑ survival rate |
[60] |
| Exogenous Adrenomedullin Administration | |||
| Animal | Procedure | Effects | Reference |
| Mouse | Pneumococcal pneumonia + Mechanical ventilation |
· ↓ VILI (pulmonary permeability↓) · ↓ liver and gut injury |
[25] |
| Rat | BDL + CLP (obstructive jaundice + polymicrobial sepsis) |
· ↓ tissue injury and inflammatory responses · ↑ survival rate |
[61] |
| Rat | Staphylococcus aureus α-toxin induced septic shock | · ↓ translocation of dextran from the gut into the systemic circulation | [62] |
| Rat | Cecal ligation and puncture (CLP) | · ↓ tissue injury · ↓ proinflammatory cytokine levels · ↓ intestinal-barrier dysfunction · ↑ survival rate |
[63] |
| Sheep | Endotoxin (LPS) infusion | · ↑ cardiac index · ↓ mean pulmonary artery pressure |
[64] |
| Rat | Endotoxin (LPS) injection | · ↑ PPER-γ level · ↓ TNF-α |
[65] |
| Rat | Intestinal ischemia/reperfusion | · ↓ lung injury · ↓ proinflammatory cytokines |
[66] |
| Rat | Staphylococcus aureus α-toxin induced septic shock | · ↓ vascular hyperpermeability · ↑ survival rate |
[67] |
| Rat | Intestinal ischemia/reperfusion | · ↓ inflammatory cytokines · ↓ tissue injury · ↑ survival rate |
[68] |
AM: adrenomedullin, LPS: lipopolysaccharide, WT: wild type. TNF: tumor necrosis factor, IF: interferon, BP: blood pressure. VILI: ventilator induced lung injury, BDL: common bile duct ligation. PPER: peroxisome proliferator-activated receptor.
4. Adrecizumab and Sepsis
5. Overview of Therapies for COVID-19
6. AM and COVID-19
7. Clinical Trials Using AM for COVID-19
7.1. Progress of Clinical Trials Using AM
7.2. Phase 2a Clinical Trial for COVID-19
8. Conclusions
References
- COVID-19 Dashboard by the Center for Systems Science and Engineering at Johns Hopkins University. Available online: https://coronavirus.jhu.edu/map.html (accessed on 5 January 2022).
- Mahmud, M.S.; Kamrujjaman, M.; Adan, M.M.Y.; Hossain, M.A.; Rahman, M.M.; Islam, M.S.; Mohebujjaman, M.; Molla, M.M. Vaccine Efficacy and SARS-CoV-2 Control in California and U.S. During the Session 2020–2026: A Modeling Study. Infect. Dis. Modell. 2022, 7, 62–81. [Google Scholar] [CrossRef] [PubMed]
- Bernal, A.J.; da Silva, M.M.G.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Reyes, V.D.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID-19: Pfizer’s Paxlovid Is 89% Effective in Patients At Risk of Serious Illness, Company Reports. BMJ 2021, 375, n2713. [Google Scholar] [CrossRef] [PubMed]
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef]
- Chen, P.; Nirula, A.; Heller, B.; Gottlieb, R.L.; Boscia, J.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. SARS-CoV-2 Neutralizing Antibody LY-CoV555 in Outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 229–237. [Google Scholar] [CrossRef]
- Crichton, M.L.; Goeminne, P.C.; Tuand, K.; Vandendriessche, T.; Tonia, T.; Roche, N.; Chalmers, J.D.; European Respiratory Society. COVID-19 Task Force. The Impact of Therapeutics on Mortality in Hospitalised Patients with COVID-19: Systematic Review and Meta-Analyses Informing the European Respiratory Society Living Guideline. Eur. Respir. Rev. 2021, 30, 210171. [Google Scholar] [CrossRef]
- ACTIV-3/TICO LY-CoV555 Study Group; Lundgren, J.D.; Grund, B.; Barkauskas, C.E.; Holland, T.L.; Gottlieb, R.L.; Sandkovsky, U.; Brown, S.M.; Knowlton, K.U.; Self, W.H.; et al. A Neutralizing Monoclonal Antibody for Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 905–914. [Google Scholar] [CrossRef]
- Rahim, F.; Amin, S.; Noor, M.; Bahadur, S.; Gul, H.; Mahmood, A.; Usman, M.; Khan, M.A.; Ullah, R.; Shahab, K. Mortality of Patients with Severe COVID-19 in the Intensive Care Unit: An Observational Study from a Major COVID-19 Receiving Hospital. Cureus 2020, 12, e10906. [Google Scholar] [CrossRef]
- Roedl, K.; Jarczak, D.; Thasler, L.; Bachmann, M.; Schulte, F.; Bein, B.; Weber, C.F.; Schäfer, U.; Veit, C.; Hauber, H.P.; et al. Mechanical Ventilation and Mortality Among 223 Critically Ill Patients with Coronavirus disease 2019: A Multicentric Study in Germany. Aust. Crit. Care. 2021, 34, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Christ-Crain, M.; Morgenthaler, N.G.; Struck, J.; Harbarth, S.; Bergmann, A.; Müller, B. Mid-Regional Pro-Adrenomedullin as a Prognostic Marker in Sepsis: An Observational Study. Crit. Care 2005, 9, R816–R824. [Google Scholar] [CrossRef]
- Valenzuela Sanchez, F.; Valenzuela Méndez, B.; Bohollo de Austria, R.; Rodríguez Gutierrez, J.F.; Jaen Franco, M.; García, G.; Jareño Chaumel, A. Diagnostic and prognostic usefulness of mid-regional pro-adrenomedullin levels in patients with severe sepsis. Intensive Care Med. Exp. 2015, 3 (Suppl. 1), A306. [Google Scholar] [CrossRef]
- Enguix-Armada, A.; Escobar-Conesa, R.; García-De La Torre, A.G.; De La Torre-Prados, M.V. Usefulness of Several Biomarkers in the Management of Septic Patients: C-Reactive Protein, Procalcitonin, Presepsin and Mid-Regional Pro-Adrenomedullin. Clin. Chem. Lab. Med. 2016, 54, 163–168. [Google Scholar] [CrossRef]
- Andaluz-Ojeda, D.; Nguyen, H.B.; Meunier-Beillard, N.; Cicuéndez, R.; Quenot, J.P.; Calvo, D.; Dargent, A.; Zarca, E.; Andrés, C.; Nogales, L.; et al. Superior Accuracy of Mid-Regional Proadrenomedullin for Mortality Prediction in Sepsis with Varying Levels of Illness Severity. Ann. Intensive Care 2017, 7, 15. [Google Scholar] [CrossRef]
- Charles, P.E.; Péju, E.; Dantec, A.; Bruyère, R.; Meunier-Beillard, N.; Dargent, A.; Prin, S.; Wilson, D.; Quenot, J.P. Mr-Proadm Elevation upon Icu Admission Predicts the Outcome of Septic Patients and Is Correlated with Upcoming Fluid Overload. Shock 2017, 48, 418–426. [Google Scholar] [CrossRef]
- Elke, G.; Bloos, F.; Wilson, D.C.; Brunkhorst, F.M.; Briegel, J.; Reinhart, K.; Loeffler, M.; Kluge, S.; Nierhaus, A.; Jaschinski, U.; et al. The Use of Mid-Regional Proadrenomedullin to Identify Disease Severity and Treatment Response to Sepsis—A Secondary Analysis of a Large Randomised Controlled Trial. Crit. Care 2018, 22, 79. [Google Scholar] [CrossRef]
- Spoto, S.; Fogolari, M.; De Florio, L.; Minieri, M.; Vicino, G.; Legramante, J.; Lia, M.S.; Terrinoni, A.; Caputo, D.; Costantino, S.; et al. Procalcitonin and MR-proAdrenomedullin Combination in the Etiological Diagnosis and Prognosis of Sepsis and Septic Shock. Microb. Pathog. 2019, 137, 103763. [Google Scholar] [CrossRef]
- Spoto, S.; Nobile, E.; Carnà, E.P.R.; Fogolari, M.; Caputo, D.; De Florio, L.; Valeriani, E.; Benvenuto, D.; Costantino, S.; Ciccozzi, M.; et al. Best Diagnostic Accuracy of Sepsis Combining SIRS Criteria or qSOFA Score with Procalcitonin and Mid-Regional Pro-Adrenomedullin Outside ICU. Sci. Rep. 2020, 10, 16605. [Google Scholar] [CrossRef]
- Marino, R.; Struck, J.; Maisel, A.S.; Magrini, L.; Bergmann, A.; Di Somma, S.; Adrenomedullin, P. Plasma Adrenomedullin Is Associated with Short-Term Mortality and Vasopressor Requirement in Patients Admitted with Sepsis. Crit. Care 2014, 18, R34. [Google Scholar] [CrossRef]
- Chen, Y.X.; Li, C.S. Prognostic Value of Adrenomedullin in Septic Patients in the ED. Am. J. Emerg. Med. 2013, 31, 1017–1021. [Google Scholar] [CrossRef]
- Guignant, C.; Voirin, N.; Venet, F.; Poitevin, F.; Malcus, C.; Bohé, J.; Lepape, A.; Monneret, G. Assessment of Provasopressin and Pro-Adrenomedullin as Predictors of 28-Day Mortality in Septic Shock Patients. Intensive Care Med. 2009, 35, 1859–1867. [Google Scholar] [CrossRef]
- Caironi, P.; Latini, R.; Struck, J.; Hartmann, O.; Bergmann, A.; Maggio, G.; Cavana, M.; Tognoni, G.; Pesenti, A.; Gattinoni, L.; et al. Circulating Biologically Active Adrenomedullin (Bio-ADM) Predicts Hemodynamic Support Requirement and Mortality During Sepsis. Chest 2017, 152, 312–320. [Google Scholar] [CrossRef]
- Mebazaa, A.; Geven, C.; Hollinger, A.; Wittebole, X.; Chousterman, B.G.; Blet, A.; Gayat, E.; Hartmann, O.; Scigalla, P.; Struck, J.; et al. Circulating Adrenomedullin Estimates Survival and Reversibility of Organ Failure in Sepsis: The Prospective Observational Multinational Adrenomedullin and Outcome in Sepsis and Septic Shock-1 (AdrenOSS-1) Study. Crit. Care 2018, 22, 354. [Google Scholar] [CrossRef]
- Geven, C.; Kox, M.; Pickkers, P. Adrenomedullin and Adrenomedullin-Targeted Therapy as Treatment Strategies Relevant for Sepsis. Front. Immunol. 2018, 9, 292. [Google Scholar] [CrossRef]
- Müller-Redetzky, H.C.; Will, D.; Hellwig, K.; Kummer, W.; Tschernig, T.; Pfeil, U.; Paddenberg, R.; Menger, M.D.; Kershaw, O.; Gruber, A.D.; et al. Mechanical Ventilation Drives Pneumococcal Pneumonia into Lung Injury and Sepsis in Mice: Protection by Adrenomedullin. Crit. Care 2014, 18, R73. [Google Scholar] [CrossRef]
- van Oers, J.A.H.; Kluiters, Y.; Bons, J.A.P.; de Jongh, M.; Pouwels, S.; Ramnarain, D.; de Lange, D.W.; de Grooth, H.J.; Girbes, A.R.J. Endothelium-Associated Biomarkers Mid-Regional Proadrenomedullin and C-Terminal proendothelin-1 Have Good Ability to Predict 28-Day Mortality in Critically Ill Patients with SARS-CoV-2 Pneumonia: A Prospective Cohort Study. J. Crit. Care 2021, 66, 173–180. [Google Scholar] [CrossRef]
- García de Guadiana-Romualdo, L.; Martínez Martínez, M.; Rodríguez Mulero, M.D.; Esteban-Torrella, P.; Hernández Olivo, M.; Alcaraz García, M.J.; Campos-Rodríguez, V.; Sancho-Rodríguez, N.; Galindo Martínez, M.; Alcaraz, A.; et al. Circulating MR-ProADM Levels, as an Indicator of Endothelial Dysfunction, for Early Risk Stratification of Mid-Term Mortality in COVID-19 Patients. Int. J. Infect. Dis. 2021, 111, 211–218. [Google Scholar] [CrossRef]
- Zaninotto, M.; Mion, M.M.; Marchioro, L.; Padoan, A.; Plebani, M. Endothelial Dysfunction and Mid-Regional Proadrenomedullin: What Role in SARS-CoV-2 Infected Patients? Clin. Chim. Acta 2021, 523, 185–190. [Google Scholar] [CrossRef]
- Lo Sasso, B.; Gambino, C.M.; Scichilone, N.; Giglio, R.V.; Bivona, G.; Scazzone, C.; Muratore, R.; Milano, S.; Barbagallo, M.; Agnello, L.; et al. Clinical Utility of Midregional Proadrenomedullin in Patients with COVID-19. Lab. Med. 2021, 52, 493–498. [Google Scholar] [CrossRef]
- Roedl, K.; Jarczak, D.; Fischer, M.; Haddad, M.; Boenisch, O.; de Heer, G.; Burdelski, C.; Frings, D.; Sensen, B.; Karakas, M.; et al. MR-proAdrenomedullin as a Predictor of Renal Replacement Therapy in a Cohort of Critically Ill Patients with COVID-19. Biomarkers 2021, 26, 417–424. [Google Scholar] [CrossRef]
- García de Guadiana-Romualdo, L.; Calvo Nieves, M.D.; Rodríguez Mulero, M.D.; Calcerrada Alises, I.; Hernández Olivo, M.; Trapiello Fernández, W.; González Morales, M.; Bolado Jiménez, C.; Albaladejo-Otón, M.D.; Fernández Ovalle, H.; et al. MR-ProADM as Marker of Endotheliitis Predicts COVID-19 Severity. Eur. J. Clin. Investig. 2021, 51, e13511. [Google Scholar] [CrossRef]
- Spoto, S.; Agrò, F.E.; Sambuco, F.; Travaglino, F.; Valeriani, E.; Fogolari, M.; Mangiacapra, F.; Costantino, S.; Ciccozzi, M.; Angeletti, S. High Value of Mid-Regional Proadrenomedullin in COVID-19: A Marker of Widespread Endothelial Damage, Disease Severity, and Mortality. J. Med. Virol. 2021, 93, 2820–2827. [Google Scholar] [CrossRef]
- Gregoriano, C.; Koch, D.; Kutz, A.; Haubitz, S.; Conen, A.; Bernasconi, L.; Hammerer-Lercher, A.; Saeed, K.; Mueller, B.; Schuetz, P. The Vasoactive Peptide MR-Pro-Adrenomedullin in COVID-19 Patients: An Observational Study. Clin. Chem. Lab. Med. 2021, 59, 995–1004. [Google Scholar] [CrossRef]
- Sozio, E.; Tascini, C.; Fabris, M.; D’Aurizio, F.; De Carlo, C.; Graziano, E.; Bassi, F.; Sbrana, F.; Ripoli, A.; Pagotto, A.; et al. MR-ProADM as Prognostic Factor of Outcome in COVID-19 Patients. Sci. Rep. 2021, 11, 5121. [Google Scholar] [CrossRef]
- Montrucchio, G.; Sales, G.; Rumbolo, F.; Palmesino, F.; Fanelli, V.; Urbino, R.; Filippini, C.; Mengozzi, G.; Brazzi, L. Effectiveness of Mid-Regional Pro-Adrenomedullin (MR-ProADM) as Prognostic Marker in COVID-19 Critically Ill Patients: An Observational Prospective Study. PLoS ONE 2021, 16, e0246771. [Google Scholar] [CrossRef]
- Benedetti, I.; Spinelli, D.; Callegari, T.; Bonometti, R.; Molinaro, E.; Novara, E.; Cassinari, M.; Frino, C.; Guaschino, R.; Boverio, R.; et al. High Levels of Mid-Regional Proadrenomedullin in ARDS COVID-19 Patients: The Experience of a Single, Italian Center. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1743–1751. [Google Scholar] [CrossRef]
- Kitamura, K.; Kangawa, K.; Kawamoto, M.; Ichiki, Y.; Nakamura, S.; Matsuo, H.; Eto, T. Adrenomedullin: A Novel Hypotensive Peptide Isolated from Human Pheochromocytoma. Biochem. Biophys. Res. Commun. 1993, 192, 553–560. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Amylin, Calcitonin Gene-Related Peptide, Calcitonin, and Adrenomedullin: A Peptide Superfamily. Crit. Rev. Neurobiol. 1997, 11, 167–239. [Google Scholar] [CrossRef]
- Takei, Y.; Inoue, K.; Ogoshi, M.; Kawahara, T.; Bannai, H.; Miyano, S. Identification of Novel Adrenomedullin in Mammals: A Potent Cardiovascular and Renal Regulator. FEBS Lett. 2004, 556, 53–58. [Google Scholar] [CrossRef]
- Kitamura, K.; Kato, J.; Kawamoto, M.; Tanaka, M.; Chino, N.; Kangawa, K.; Eto, T. The Intermediate Form of Glycine-Extended Adrenomedullin Is the Major Circulating Molecular Form in Human Plasma. Biochem. Biophys. Res. Commun. 1998, 244, 551–555. [Google Scholar] [CrossRef]
- Struck, J.; Tao, C.; Morgenthaler, N.G.; Bergmann, A. Identification of an Adrenomedullin Precursor Fragment in Plasma of Sepsis Patients. Peptides 2004, 25, 1369–1372. [Google Scholar] [CrossRef]
- Fischer, J.P.; Els-Heindl, S.; Beck-Sickinger, A.G. Adrenomedullin—Current Perspective on a Peptide Hormone with Significant Therapeutic Potential. Peptides 2020, 131, 170347. [Google Scholar] [CrossRef]
- Shindo, T.; Kurihara, Y.; Nishimatsu, H.; Moriyama, N.; Kakoki, M.; Wang, Y.; Imai, Y.; Ebihara, A.; Kuwaki, T.; Ju, K.H.; et al. Vascular Abnormalities and Elevated Blood Pressure in Mice Lacking Adrenomedullin Gene. Circulation 2001, 104, 1964–1971. [Google Scholar] [CrossRef]
- Caron, K.M.; Smithies, O. Extreme Hydrops fetalis and Cardiovascular Abnormalities in Mice Lacking a Functional Adrenomedullin Gene. Proc. Natl. Acad. Sci. USA 2001, 98, 615–619. [Google Scholar] [CrossRef]
- Dackor, R.T.; Fritz-Six, K.; Dunworth, W.P.; Gibbons, C.L.; Smithies, O.; Caron, K.M. Hydrops fetalis, Cardiovascular Defects, and Embryonic Lethality in Mice Lacking the Calcitonin Receptor-Like Receptor Gene. Mol. Cell. Biol. 2006, 26, 2511–2518. [Google Scholar] [CrossRef]
- Shindo, T.; Sakurai, T.; Kamiyoshi, A.; Ichikawa-Shindo, Y.; Shimoyama, N.; Iinuma, N.; Arai, T.; Miyagawa, S. Regulation of Adrenomedullin and Its Family Peptide by RAMP System—Lessons from Genetically Engineered Mice. Curr. Protein Pept. Sci. 2013, 14, 347–357. [Google Scholar] [CrossRef]
- Yamauchi, A.; Sakurai, T.; Kamiyoshi, A.; Ichikawa-Shindo, Y.; Kawate, H.; Igarashi, K.; Toriyama, Y.; Tanaka, M.; Liu, T.; Xian, X.; et al. Functional Differentiation of RAMP2 and RAMP3 in Their Regulation of the Vascular System. J. Mol. Cell. Cardiol. 2014, 77, 73–85. [Google Scholar] [CrossRef]
- Li, P.; Wang, C.; Pang, S. The Diagnostic Accuracy of Mid-Regional Pro-Adrenomedullin for Sepsis: A Systematic Review and Meta-Analysis. Minerva Anestesiol. 2021, 87, 1117–1127. [Google Scholar] [CrossRef]
- Bełtowski, J.; Jamroz, A. Adrenomedullin--what do we know 10 years since its discovery? Pol. J. Pharmacol. 2004, 56, 5–27. [Google Scholar]
- Eto, T.; Kato, J.; Kitamura, K. Regulation of Production and Secretion of Adrenomedullin in the Cardiovascular System. Regul. Pept. 2003, 112, 61–69. [Google Scholar] [CrossRef]
- Nagaya, N.; Goto, Y.; Satoh, T.; Sumida, H.; Kojima, S.; Miyatake, K.; Kangawa, K. Intravenous adrenomedullin in myocardial function and energy metabolism in patients after myocardial infarction. J. Cardiovasc. Pharmacol. 2002, 39, 754–760. [Google Scholar] [CrossRef]
- Terata, K.; Miura, H.; Liu, Y.; Loberiza, F.; Gutterman, D.D. Human coronary arteriolar dilation to adrenomedullin: Role of nitric oxide and K(+) channels. Am. J. Physiol. Heart Circ. Physiol. 2000, 279, H2620–H2626. [Google Scholar] [CrossRef] [PubMed]
- Iring, A.; Jin, Y.J.; Albarrán-Juárez, J.; Siragusa, M.; Wang, S.; Dancs, P.T.; Nakayama, A.; Tonack, S.; Chen, M.; Künne, C.; et al. Shear Stress-Induced Endothelial Adrenomedullin Signaling Regulates Vascular Tone and Blood Pressure. J. Clin. Investig. 2019, 129, 2775–2791. [Google Scholar] [CrossRef] [PubMed]
- Temmesfeld-Wollbrück, B.; Hocke, A.C.; Suttorp, N.; Hippenstiel, S. Adrenomedullin and Endothelial Barrier Function. Thromb. Haemost. 2007, 98, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Zhou, M.; Chaudry, I.H.; Wang, P. Novel Approach to Prevent the Transition from the Hyperdynamic Phase to the Hypodynamic Phase of Sepsis: Role of Adrenomedullin and Adrenomedullin Binding protein-1. Ann. Surg. 2002, 236, 625–633. [Google Scholar] [CrossRef]
- Ince, C.; Mayeux, P.R.; Nguyen, T.; Gomez, H.; Kellum, J.A.; Ospina-Tascón, G.A.; Hernandez, G.; Murray, P.; De Backer, D.; ADQI XIV Workgroup. The Endothelium in Sepsis. Shock 2016, 45, 259–270. [Google Scholar] [CrossRef]
- Müller-Redetzky, H.C.; Suttorp, N.; Witzenrath, M. Dynamics of Pulmonary Endothelial Barrier Function in Acute Inflammation: Mechanisms and Therapeutic Perspectives. Cell Tissue Res. 2014, 355, 657–673. [Google Scholar] [CrossRef]
- Saito, R.; Shimosawa, T.; Ogihara, T.; Maruyama, N.; Fujita, T.; Okamura, N.; Nakahara, K. Function of Adrenomedullin in Inflammatory Response of Liver Against LPS-Induced Endotoxemia. APMIS 2012, 120, 706–711. [Google Scholar] [CrossRef]
- Dackor, R.; Caron, K. Mice Heterozygous for Adrenomedullin Exhibit a More Extreme Inflammatory Response to Endotoxin-Induced Septic Shock. Peptides 2007, 28, 2164–2170. [Google Scholar] [CrossRef]
- Shindo, T.; Kurihara, H.; Maemura, K.; Kurihara, Y.; Kuwaki, T.; Izumida, T.; Minamino, N.; Ju, K.H.; Morita, H.; Oh-Hashi, Y.; et al. Hypotension and Resistance to Lipopolysaccharide-Induced Shock in Transgenic Mice Overexpressing Adrenomedullin in Their Vasculature. Circulation 2000, 101, 2309–2316. [Google Scholar] [CrossRef]
- Yang, J.; Wu, R.; Zhou, M.; Wang, P. Human Adrenomedullin and Its Binding Protein Ameliorate Sepsis-Induced Organ Injury and Mortality in Jaundiced Rats. Peptides 2010, 31, 872–877. [Google Scholar] [CrossRef]
- Temmesfeld-Wollbrück, B.; Brell, B.; zu Dohna, C.; Dorenberg, M.; Hocke, A.C.; Martens, H.; Klar, J.; Suttorp, N.; Hippenstiel, S. Adrenomedullin Reduces Intestinal Epithelial Permeability In Vivo and In Vitro. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 297, G43–G51. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Higuchi, S.; Dong, W.; Ji, Y.; Zhou, M.; Marini, C.P.; Ravikumar, T.S.; Wang, P. Reversing Established Sepsis in Rats with Human Vasoactive Hormone Adrenomedullin and Its Binding Protein. Mol. Med. 2009, 15, 28–33. [Google Scholar] [CrossRef]
- Ertmer, C.; Morelli, A.; Rehberg, S.; Lange, M.; Hucklenbruch, C.; Van Aken, H.; Booke, M.; Westphal, M. Exogenous Adrenomedullin Prevents and Reverses Hypodynamic Circulation and Pulmonary Hypertension in Ovine Endotoxaemia. Br. J. Anaesth. 2007, 99, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Miksa, M.; Wu, R.; Cui, X.; Dong, W.; Das, P.; Simms, H.H.; Ravikumar, T.S.; Wang, P. Vasoactive Hormone Adrenomedullin and Its Binding Protein: Anti-Inflammatory Effects by Up-Regulating Peroxisome Proliferator-Activated Receptor-Gamma. J. Immunol. 2007, 179, 6263–6272. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.J.; Wu, R.; Nguyen, E.; Higuchi, S.; Wang, H.; Krishnasastry, K.; Marini, C.P.; Ravikumar, T.S.; Wang, P. Adrenomedullin and Adrenomedullin Binding protein-1 Prevent Acute Lung Injury After Gut Ischemia-Reperfusion. J. Am. Coll. Surg. 2007, 205, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Temmesfeld-Wollbrück, B.; Brell, B.; Dávid, I.; Dorenberg, M.; Adolphs, J.; Schmeck, B.; Suttorp, N.; Hippenstiel, S. Adrenomedullin Reduces Vascular Hyperpermeability and Improves Survival in Rat Septic Shock. Intensive Care Med. 2007, 33, 703–710. [Google Scholar] [CrossRef]
- Carrizo, G.J.; Wu, R.; Cui, X.; Dwivedi, A.J.; Simms, H.H.; Wang, P. Adrenomedullin and Adrenomedullin-Binding protein-1 Downregulate Inflammatory Cytokines and Attenuate Tissue Injury After Gut Ischemia-Reperfusion. Surgery 2007, 141, 245–253. [Google Scholar] [CrossRef]
- Zaks-Zilberman, M.; Salkowski, C.A.; Elsasser, T.; Cuttitta, F.; Vogel, S.N. Induction of Adrenomedullin mRNA and Protein by Lipopolysaccharide and Paclitaxel (Taxol) in Murine Macrophages. Infect. Immun. 1998, 66, 4669–4675. [Google Scholar] [CrossRef]
- Geven, C.; van Lier, D.; Blet, A.; Peelen, R.; ten Elzen, B.; Mebazaa, A.; Kox, M.; Pickkers, P. Safety, Tolerability and Pharmacokinetics/-Dynamics of the Adrenomedullin Antibody Adrecizumab in a First-Inhuman Study and During Experimental Human Endotoxemia in Healthy Subjects. Br. J. Clin. Pharmacol. 2018, 84, 2129–2141. [Google Scholar] [CrossRef]
- Geven, C.; Peters, E.; Schroedter, M.; Struck, J.; Bergmann, A.; McCook, O.; Radermacher, P.; Kox, M.; Pickkers, P. Effects of the Humanized Anti-Adrenomedullin Antibody Adrecizumab (HAM8101) on Vascular Barrier Function and Survival in Rodent Models of Systemic Inflammation and Sepsis. Shock 2018, 50, 648–654. [Google Scholar] [CrossRef]
- Blet, A.; Deniau, B.; Geven, C.; Sadoune, M.; Caillard, A.; Kounde, P.R.; Polidano, E.; Pickkers, P.; Samuel, J.L.; Mebazaa, A. Adrecizumab, a Non-Neutralizing Anti-Adrenomedullin Antibody, Improves Haemodynamics and Attenuates Myocardial Oxidative Stress in Septic Rats. Intensive Care Med. Exp. 2019, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Thiele, C.; Simon, T.P.; Szymanski, J.; Daniel, C.; Golias, C.; Hartmann, O.; Struck, J.; Martin, L.; Marx, G.; Schuerholz, T. Effects of the Non-Neutralizing Humanized Monoclonal Anti-Adrenomedullin Antibody Adrecizumab on Hemodynamic and Renal Injury in a Porcine Two-Hit Model. Shock 2020, 54, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Laterre, P.F.; Pickkers, P.; Marx, G.; Wittebole, X.; Meziani, F.; Dugernier, T.; Huberlant, V.; Schuerholz, T.; François, B.; Lascarrou, J.B.; et al. Safety and Tolerability of Non-Neutralizing Adrenomedullin Antibody Adrecizumab (HAM8101) in Septic Shock Patients: The AdrenOSS-2 phase 2a Biomarker-Guided Trial. Intensive Care Med. 2021, 47, 1284–1294. [Google Scholar] [CrossRef] [PubMed]
- Assouline, B.; Faivre, A.; Verissimo, T.; Sangla, F.; Berchtold, L.; Giraud, R.; Bendjelid, K.; Sgardello, S.; Elia, N.; Pugin, J.; et al. Thiamine, Ascorbic Acid, and Hydrocortisone as a Metabolic Resuscitation Cocktail in Sepsis: A Meta-Analysis of Randomized Controlled Trials with Trial Sequential Analysis. Crit. Care Med. 2021, 49, 2112–2120. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Noori, M.; Nejadghaderi, S.A.; Arshi, S.; Carson-Chahhoud, K.; Ansarin, K.; Kolahi, A.A.; Safiri, S. Potency of BNT162b2 and mRNA-1273 Vaccine-Induced Neutralizing Antibodies Against Severe Acute Respiratory Syndrome-CoV-2 Variants of Concern: A Systematic Review of In Vitro Studies. Rev. Med. Virol. 2021, e2277. [Google Scholar] [CrossRef]
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.G.; Gray, G. Effectiveness of BNT162b2 Vaccine Against Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Valoriani, B.; Barbieri, C.; Occhineri, S.; Mazzetti, P.; Vatteroni, M.L.; Suardi, L.R.; Riccardi, N.; Pistello, M.; et al. Efficacy of Bamlanivimab/Etesevimab and Casirivimab/Imdevimab in Preventing Progression to Severe COVID-19 and Role of Variants of Concern. Infect. Dis. Ther. 2021, 10, 2479–2488. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, A.; Singh, R.; Misra, A. An Updated Practical Guideline on Use of Molnupiravir and Comparison with Agents Having Emergency Use Authorization for Treatment of COVID-19. Diabetes Metab. Syndr. 2022, 16, 102396. [Google Scholar] [CrossRef]
- Agarwal, A.; Rochwerg, B.; Lamontagne, F.; Siemieniuk, R.A.; Agoritsas, T.; Askie, L.; Lytvyn, L.; Leo, Y.S.; Macdonald, H.; Zeng, L.; et al. A Living WHO Guideline on Drugs for COVID-19. BMJ 2020, 370, m3379. [Google Scholar] [CrossRef]
- Ngamprasertchai, T.; Kajeekul, R.; Sivakorn, C.; Ruenroegnboon, N.; Luvira, V.; Siripoon, T.; Luangasanatip, N. Efficacy and Safety of Immunomodulators in Patients with COVID-19: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Infect. Dis. Ther. 2022, 11, 231–248. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in Patients Admitted to Hospital with COVID-19 (RECOVERY): A Randomised, Controlled, Open-Label, Platform Trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; de Cassia Pellegrini, R.; et al. Efficacy and Safety of Baricitinib for the Treatment of Hospitalised Adults with COVID-19 (COV-BARRIER): A Randomised, Double-Blind, Parallel-Group, Placebo-Controlled phase 3 Trial. Lancet Respir. Med. 2021, 9, 1407–1418. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Muñoz Martin, A.J. Thrombosis and Coagulopathy in COVID-19. Curr. Probl. Cardiol. 2021, 46, 100742. [Google Scholar] [CrossRef]
- Hadid, T.; Kafri, Z.; Al-Katib, A. Coagulation and Anticoagulation in COVID-19. Blood Rev. 2021, 47, 100761. [Google Scholar] [CrossRef]
- Asakura, H.; Ogawa, H. COVID-19-associated Coagulopathy and Disseminated Intravascular Coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef]
- Vincent, J.L.; Levi, M.; Hunt, B.J. Prevention and Management of Thrombosis in Hospitalised Patients with COVID-19 Pneumonia. Lancet Respir. Med. 2021, 21, S2213–S2600. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Ferrario, C.M.; Jessup, J.; Chappell, M.C.; Averill, D.B.; Brosnihan, K.B.; Tallant, E.A.; Diz, D.I.; Gallagher, P.E. Effect of Angiotensin-Converting Enzyme Inhibition and Angiotensin II Receptor Blockers on Cardiac Angiotensin-Converting enzyme 2. Circulation 2005, 111, 2605–2610. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Ma, Z.; Yang, K.Y.; Huang, Y.; Lui, K.O. Endothelial Contribution to COVID-19: An Update on Mechanisms and Therapeutic Implications. J. Mol. Cell. Cardiol. 2021, 164, 69–82. [Google Scholar] [CrossRef]
- Dirican, A.; Ildir, S.; Uzar, T.; Karaman, I.; Ozkaya, S. The Role of Endotheliitis in COVID-19: Real-World Experience of 11 190 Patients and Literature Review for a Pathophysiological Map to Clinical Categorization. Int. J. Clin. Pract. 2021, 75, e14843. [Google Scholar] [CrossRef]
- Flaumenhaft, R.; Enjyoji, K.; Schmaier, A.A. Vasculopathy in COVID-19. Blood 2022. ahead of print. [Google Scholar] [CrossRef]
- Brell, B.; Temmesfeld-Wollbrück, B.; Altzschner, I.; Frisch, E.; Schmeck, B.; Hocke, A.C.; Suttorp, N.; Hippenstiel, S. Adrenomedullin Reduces Staphylococcus aureus alpha-Toxin-Induced Rat Ileum Microcirculatory Damage. Crit. Care Med. 2005, 33, 819–826. [Google Scholar] [CrossRef]
- Hippenstiel, S.; Witzenrath, M.; Schmeck, B.; Hocke, A.; Krisp, M.; Krüll, M.; Seybold, J.; Seeger, W.; Rascher, W.; Schütte, H.; et al. Adrenomedullin Reduces Endothelial Hyperpermeability. Circ. Res. 2002, 91, 618–625. [Google Scholar] [CrossRef]
- Wilson, D.C.; Schefold, J.C.; Baldirà, J.; Spinetti, T.; Saeed, K.; Elke, G. Adrenomedullin in COVID-19 Induced Endotheliitis. Crit. Care. 2020, 24, 411. [Google Scholar] [CrossRef]
- Martin-Fernandez, M.; Vaquero-Roncero, L.M.; Almansa, R.; Gómez-Sánchez, E.; Martín, S.; Tamayo, E.; Esteban-Velasco, M.C.; Ruiz-Granado, P.; Aragón, M.; Calvo, D.; et al. Endothelial Dysfunction Is an Early Indicator of Sepsis and Neutrophil Degranulation of Septic Shock in Surgical Patients. BJS Open 2020, 4, 524–534. [Google Scholar] [CrossRef]
- Hupf, J.; Mustroph, J.; Hanses, F.; Evert, K.; Maier, L.S.; Jungbauer, C.G. RNA-Expression of Adrenomedullin Is Increased in Patients with Severe COVID-19. Crit. Care 2020, 24, 527. [Google Scholar] [CrossRef]
- Simon, T.P.; Stoppe, C.; Breuer, T.; Stiehler, L.; Dreher, M.; Kersten, A.; Kluge, S.; Karakas, M.; Zechendorf, E.; Marx, G.; et al. Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study. J. Clin. Med. 2021, 10, 1667. [Google Scholar] [CrossRef]
- Karakas, M.; Jarczak, D.; Becker, M.; Roedl, K.; Addo, M.M.; Hein, F.; Bergmann, A.; Zimmermann, J.; Simon, T.P.; Marx, G.; et al. Targeting Endothelial Dysfunction in Eight Extreme-Critically Ill Patients with COVID-19 Using the Anti-Adrenomedullin Antibody Adrecizumab (HAM8101). Biomolecules 2020, 10, 1171. [Google Scholar] [CrossRef]
- Ashizuka, S.; Inagaki-Ohara, K.; Kuwasako, K.; Kato, J.; Inatsu, H.; Kitamura, K. Adrenomedullin Treatment Reduces Intestinal Inflammation and Maintains Epithelial Barrier Function in Mice Administered Dextran Sulphate Sodium. Microbiol. Immunol. 2009, 53, 573–581. [Google Scholar] [CrossRef]
- Ashizuka, S.; Inatsu, H.; Kita, T.; Kitamura, K. Adrenomedullin Therapy in Patients with Refractory Ulcerative Colitis: A Case Series. Dig. Dis. Sci. 2016, 61, 872–880. [Google Scholar] [CrossRef]
- Meeran, K.; O’Shea, D.; Upton, P.D.; Small, C.J.; Ghatei, M.A.; Byfield, P.H.; Bloom, S.R. Circulating Adrenomedullin Does Not Regulate Systemic Blood Pressure but Increases Plasma Prolactin After Intravenous Infusion in Humans: A Pharmacokinetic Study. J. Clin. Endocrinol. Metab. 1997, 82, 95–100. [Google Scholar] [CrossRef]
- Kita, T.; Kitamura, K. Translational Studies of Adrenomedullin and Related Peptides Regarding Cardiovascular Diseases. Hypertens. Res. 2022, 45, 389–400. [Google Scholar] [CrossRef]
- Ashizuka, S.; Ishikawa, N.; Kato, J.; Yamaga, J.; Inatsu, H.; Eto, T.; Kitamura, K. Effect of Adrenomedullin Administration on Acetic Acid-Induced Colitis in Rats. Effect of Adrenomedullin Administration on Acetic Acid-Induced Colitis in Rats. Peptides 2005, 26, 2610–2615. [Google Scholar] [CrossRef]
- Kita, T.; Suzuki, Y.; Kitamura, K. Hemodynamic and Hormonal Effects of Exogenous Adrenomedullin Administration in Humans and Relationship to Insulin Resistance. Hypertens. Res. 2010, 33, 314–319. [Google Scholar] [CrossRef]
- Kita, T.; Tokashiki, M.; Kitamura, K. Aldosterone Antisecretagogue and Antihypertensive Actions of Adrenomedullin in Patients with Primary Aldosteronism. Hypertens. Res. 2010, 33, 374–379. [Google Scholar] [CrossRef]
- Ashizuka, S.; Kita, T.; Inatsu, H.; Kitamura, K. Adrenomedullin: A Novel Therapy for Intractable Ulcerative Colitis. Inflam. Bowel Dis. 2013, 19, E26–E27. [Google Scholar] [CrossRef] [PubMed]
- Ashizuka, S.; Kuroishi, N.; Nakashima, K.; Inatsu, H.; Kita, T.; Kitamura, K. Adrenomedullin: A Novel Therapy for Intractable Crohn’s Disease with a Loss of Response to Infliximab. Intern. Med. 2019, 58, 1573–1576. [Google Scholar] [CrossRef] [PubMed]
- Kita, T.; Kaji, Y.; Kitamura, K. Safety, Tolerability, and Pharmacokinetics of Adrenomedullin in Healthy Males: A Randomized, Double-Blind, phase 1 Clinical Trial. Drug Des. Dev. Ther. 2020, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kita, T.; Ashizuka, S.; Ohmiya, N.; Yamamoto, T.; Kanai, T.; Motoya, S.; Hirai, F.; Nakase, H.; Moriyama, T.; Nakamura, M.; et al. Adrenomedullin for Steroid-Resistant Ulcerative Colitis: A Randomized, Double-Blind, Placebo-Controlled phase-2a Clinical Trial. J. Gastroenterol. 2021, 56, 147–157. [Google Scholar] [CrossRef]
- Karakas, M.; Akin, I.; Burdelski, C.; Clemmensen, P.; Grahn, H.; Jarczak, D.; Keßler, M.; Kirchhof, P.; Landmesser, U.; Lezius, S.; et al. Single-Dose of Adrecizumab Versus Placebo in Acute Cardiogenic Shock (ACCOST-HH): An Investigator-Initiated, Randomised, Double-Blinded, Placebo-Controlled, Multicentre Trial. Lancet Respir. Med. 2021. ahead of print. [Google Scholar] [CrossRef]