Lumbosacral traumatic injuries are reported as 39% of canine vertebral lesions. This area is prone to fracture and luxation. Non-ambulatory paraparesis/plegia, sciatic nerve involvement, faecal/urinary incontinence, and severe back lumbar pain were the most reported signs. Survey radiographs were the most reported technique to confirm the diagnoses. The seventh lumbar vertebra fracture, despite the different surgical techniques performed, had a favourable prognosis for long-term outcome and neurological recovery.
- spinal fracture
- L7 fracture
- traumatic lumbosacral joint dislocation
- spine stabilization
- dog
1. Introduction
2. Canine Seventh Lumbar Vertebra Fracture
2.1. Anatomical and Biomechanical Considerations
2.2. Clinical Presentation
The lumbosacral joint fracture causes severe back lumbar pain due to mechanical instability and secondary neurological deficits. The clinical presentation may consist of an ambulatory paraparesis, non-ambulatory paraparesis, or plegia from sciatic nerve involvement and faecal/urinary incontinence. Moreover, concomitant injuries (i.e., hindlimb fractures, concomitant pelvic fractures and coxofemoral luxation, and severe soft tissues damage) are often reported and need to be addressed before the LS surgical approach. Ambulatory paraparesis was detected in 31.5% (12/38) of the cases, non/ambulatory paraparesis or plegia in 60.5% (23/38), sciatic nerve involvement in 21.0% (8/38), and faecal/urinary incontinence in 42.1% (16/38). Moreover, at the rump inspection, different authors reported a typical dorsal displacement of the spinous process of L7 as compared to the level of the ilial wing in L7 fracture [5][6][8][11][12][13][18][19][20]. Decreased or absent pelvic limb withdrawal reflex secondary to sciatic nerve dysfunction as well as faecal and urinary incontinence due to damage of the pudendal nerve and sacral plexus were detected and reported by several authors. As reported in the literature, all dogs presented with L7 fracture had neurological signs consistent with an L6-S2 myelopathy [5][6].2.3. Imaging
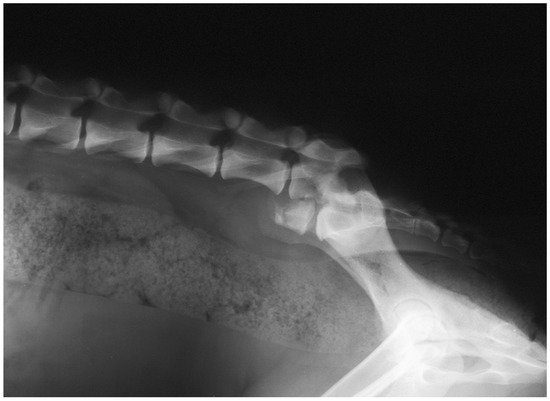
All patients with L7 fractures underwent survey radiographs in latero-lateral (LL) recumbency to confirm the diagnoses and assess the fracture or luxation [5][6][8][11][12][13][18][19][20] (Figure 1). The ventro-dorsal (VD) view was not performed for L7 fracture. In 4/38 patients, Computer Tomography (CT)-myelography was used [18].
2.4. Treatment
None of the patients with L7 fractures underwent to conservative treatment. Several surgical techniques were performed to reduce and stabilize the L7 fracture. Dulisch and colleagues, in 1981, used a double transilial pins and plastic plates to treat the L7 fracture in one patient [19]. McAnulty and colleagues in 1986 described the use of the Steinmann pins placed transversely through both ilial wings at the level of the sacral dorsal lamina, bent at a right angle, and then placed alongside the laminae and attached to the articular facets and spinous process by a stainless steel wire [8].
2.5. Complications and Prognosis
All patients surgically treated regain the ability to deambulate [5][6][8][11][12][13][18][19][20]. The failure of fixation is the primary complication detected, and incorrect choice of fixation technique, incorrect execution of fixation technique, and incorrect post-operative management are the factors leading to instability. Bone lysis around pins and pin tract infection due to inflammation/infection and breakage of pins/screw were reported as the main causes of implant failure [8][13][20]. However, the long-term prognosis can be considered favourable for outcome and neurological recovery. Caudal lumbar lesions had a better neurological status as compared to more cranially located vertebral injuries [12]. Moreover, the bone healing via callus of L7 body vertebra quickly stabilizes the fractured site ensuring a rapid solution of the orthopaedic injuries and a good neurological recovery [6].3. Conclusions
References
- Turner, W.D. Fractures and fracture-luxations of the lumbar spine: A retrospective study in the dog. J. Am. Anim. Hosp. Assoc. 1987, 23, 459–464.
- Selcer, R.R.; Bubb, W.J.; Walker, T.L. Management of vertebral column fractures in dogs and cats: 211 cases (1977–1985). J. Am. Vet. Med. Assoc. 1991, 198, 1965–1968.
- Jeffery, N.D. Vertebral fracture and luxation in small animals. Vet. Clin. N. Am. Small Anim. Pract. 2010, 40, 809–828.
- Bali, M.S.; Lang, J.; Jaggy, A.; Spreng, D.; Doherr, M.G.; Forterre, F. Comparative study of vertebral fractures and luxations in dogs and cats. Vet. Comp. Orthop. Traumatol. 2009, 22, 47–53.
- Di Dona, F.; Della Valle, G.; Lamagna, B.; Balestriere, C.; Murino, C.; Santangelo, B.; Lamagna, F.; Fatone, G. Percutaneous transilial pinning for treatment of seventh lumbar vertebral body fracture: A retrospective analysis of 17 cases. Vet. Comp. Orthop. Traumatol. 2016, 29, 164–169.
- Della Valle, G.; Di Dona, F.; Mennonna, G.; Lamagna, B.; Pasolini, M.P.; Caterino, C.; Lamagna, F.; Fatone, G. Traumatic lumbosacral joint dislocation in 3 dogs: Clinical presentation, diagnosis, treatment and short-term follow-up. Pak. Vet. J. 2021, 41, 97–101.
- Slocum, B.; Rudy, R.L. Fractures of the seventh lumbar vertebra in the dog. J. Am. Anim. Hosp. Assoc. 1975, 11, 167–174.
- McAnulty, J.F.; Lenehan, T.M.; Maletz, L.M. Modified Segmental Spinal Instrumentation in Repair of Spinal Fractures and Luxations in Dogs. Vet. Surg. 1986, 15, 143–149.
- Shores, A.; Nichols, C.; Rochat, M.; Fox, S.M.; Burt, G.J.; Fox, W.R. Combined Kirschner-Ehmer device and dorsal spinal plate fixation technique for caudal lumbar vertebral fractures in dogs. J. Am. Vet. Med. Assoc. 1989, 195, 335–339.
- Ullman, S.L.; Boudrieau, R.J. Internal Skeletal Fixation Using a Kirschner Apparatus for Stabilization of Fracture/Luxations of the Lumbosacral Joint in Six Dogs: A Modification of the Transilial Pin Technique. Vet. Surg. 1993, 22, 11–17.
- Harrington, M.L.; Bagley, R.S. Realignment of a Seventh Lumbar Vertebral Fracture/Luxation Using a Senn Retractor in Two Puppies. J. Am. Anim. Hosp. Assoc. 1998, 34, 377–380.
- Beaver, D.P.; MacPhersont, G.C.; Muir, P.; Johnson, K.A. Methyl-methacrylate and bone screw repair of seventh lumbar vertebral fracture-luxations in dogs. J. Small Anim. Pract. 1996, 37, 381–386.
- Weh, J.M.; Kraus, K.H. Use of a four pin and methylmethacrylate fixation in L7 and the iliac body to stabilize lumbosacral fracture-luxations: A clinical and anatomic study. Vet. Surg. 2007, 36, 775–782.
- Krauss, M.W.; Theyse, L.F.H.; Tryfonidou, M.A.; Hazewinkel, H.A.W.; Meij, B.P. Treatment of spinal fractures using Lubra plates: A retrospective clinical and radiological evaluation of 15 cases. Vet. Comp. Orthop. Traumatol. 2012, 25, 326–331.
- Hermanson, J.W.; de Lahunta, A. Spinal Cord and Meninges. In Miller’s Anatomy of the Dog, 5th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2018; pp. 589–610.
- Denis, F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin. Orthop. Relat. Res. 1984, 189, 65–76.
- Barquet, A.; Menendez, J.; Dubra, A.; Masliah, R.; Pereyra, D. Anterolateral dislocation of the lumbosacral junction. Can. Assoc. Radiol. J. 1993, 44, 129–132.
- Segal, U.; Bar, H.; Shani, J. Repair of lumbosacral fracture–luxation with bilateral twisted string-of-pearls locking plates. J. Small Anim. Pract. 2018, 59, 501–507.
- Dulisch, M.L.; Nichols, J.B. A Surgical Technique for Management of Lower Lumbar Fractures: Case Report. Vet. Surg. 1981, 10, 90–93.
- Wheeler, J.L.; Lewis, D.D.; Cross, A.R.; Sereda, C.W. Closed fluoroscopic-assisted spinal arch external skeletal fixation for the stabilization of vertebral column injuries in five dogs. Vet. Surg. 2007, 36, 442–448.