Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Christian Bailly and Version 2 by Rita Xu.
The disaccharide lactose is an excipient commonly used in pharmaceutical products. The two anomers, α- and β-lactose (α-L/β-L), differ by the orientation of the C-1 hydroxyl group on the glucose unit. In aqueous solution, a mutarotation process leads to an equilibrium of about 40% α-L and 60% β-L at room temperature.
- lactose
- galectin-9
- PD-1/PD-L1
- TIM-3
- soluble PD-L1
1. Introduction
The modulation of cancer immunity represents the most potent therapeutic modality in oncology. Over the past ten years, the clinical approval of different immune checkpoint blockers has led to considerable improvement in the clinical outcome of cancer patients, notably those with solid tumors such as melanoma and lung cancer. However, for several other major cancers, death rates continue to increase, or the improvement progresses very slowly [1]. Research efforts must continue and novel approaches to improve prevention, early detection, and treatment are needed.
Novel immune checkpoint targets are proposed to offer new therapeutics and modalities to treat aggressive cancers such as pancreatic cancer, brain tumors, pleural mesothelioma, and triple-negative breast cancer for example [2][3][4][5][6][7][2,3,4,5,6,7]. Intense research efforts are also dedicated to improving the treatment of onco-hematological diseases. Targeting the immune system is considered a privileged axis to combat acute myeloid leukemia (AML) which is a highly aggressive disease, or to fight lymphoma in young patients, and multiple myeloma [8][9][10][8,9,10]. One of the emerging immune checkpoint molecules is the T-cell immunoglobulin mucin-3 (Tim-3)/Galectin-9 (Gal-9) checkpoint, viewed as a promising target for the treatment of breast cancer, bladder cancer and others [11][12][13][14][11,12,13,14]. Blockade of the TIM-3/Gal-9 checkpoint is considered a valid option in hematological malignancies, notably for the treatment of AML and myelodysplastic syndromes [15][16][17][18][15,16,17,18].
2. Lactose: α- and β-Anomers
Lactose is a disaccharide composed of a galactose unit linked to a glucose unit via a β-1,4 linkage (4-O-β-D-galactopyranosyl-D-glucopyranose, or Gal β(1→4) Glc). There are two anomers, α- and β-lactose, which differ in the configuration of the C-1 hydroxyl group of the glucose unit. α-Lactose (α-L) has an axial hydroxyl whereas the hydroxyl of β-lactose (β-L) is equatorial (Figure 1). The two anomers coexist in a solution, with an equilibrium of about 40% α-L and 60% β-L at room temperature. The α-anomer presents three crystalline forms: α-lactose monohydrate (α-LM), hygroscopic anhydrous α-lactose (α-LH) and stable anhydrous α-lactose (α-LS). The β-anomer (β-L) has one crystalline form [19][20][19,20]. The polymorphs of lactose exhibit distinct physical properties, in terms of solubility, density, stability, shelf life, dissolution rate, and bioavailability. α- and β-lactose differ considerably in solubility, β-L being much more water-soluble than α-L [21]. The interconversion between the different forms has been well investigated. During the mutarotation process, a short-lived hemiacetal intermediate is generated upon a ring-opening reaction of the glucose unit [22][23][22,23]. Similarly, the conversion of α-LM to the anhydrous forms is well-controlled [24]. The α/β lactose epimerization reaction occurs rapidly in aqueous solution (t1/2 = 28.3 min at 25 °C) and the product is stable [22]. An efficient method for the preparation of pure β-L from α-LM has been reported recently [25][26][25,26].
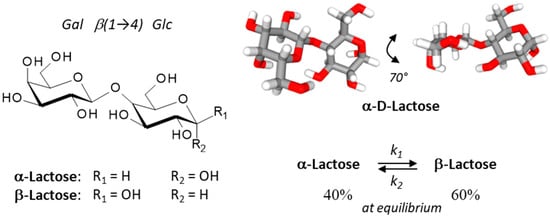
Figure 1. Structures of the two lactose anomers, α-lactose and β-lactose. Lactose contains a β-D-galactose unit linked to an α or a β-D-glucose unit through a β(1→4) bond. α-Lactose presents two crystalline forms, anhydrous α-lactose (C12H22O11) and α-lactose monohydrate (C12H22O11•H2O). The stability of lactose in aqueous solution has been determined [22]. An overall lactose epimerization rate constant (k) of 4.4 × 10−4 s−1 was measured at 25 °C (forward rate constant k1 of 2.5 × 10−4 s−1, and a reverse rate constant k2 of 1.5 ×10−4 s−1; K = 1.6 ± 0.1) and the half-life (t1/2) was 28.3 min at 25 °C. At equilibrium, the α/β anomeric ratio of lactose samples was about 39–41/59–61%, as determined at 25°, 45° and 60 °C.
Lactose is used as an additive in many foods and as a filler or diluent in pharmaceutical products. α-LM is an excipient commonly used for the manufacturing of dry granules and tablets. However, β-L anhydrous is also used in direct compression of tablet processes and as a filler in capsules [27]. As an excipient, lactose is present in nearly half of all solid medicines because it is readily available, cost-effective, chemically stable, and easily compatible with other excipients and active ingredients and has a bland taste. It provides a convenient matrix to stabilize different types of active pharmaceutical ingredients (API). α-Lactose monohydrate is also one of the most used carriers for dry powder inhaler formulations [28][29][30][28,29,30]. The lactose used as an excipient has generally a very high anomeric purity (about 96% α and 4% β) although the anomeric content of α-LM can vary significantly from one batch to another, and this variation can influence bioavailability from final formulations [31]. In solution, a rapid lactose epimerization process can occur [22]. Dehydration leads to solid-state epimerization in α-lactose powders [32]. The form of lactose can be extremely important as it can serve to modulate the property of the active ingredient. For example, the use of highly porous lactose as a carrier can significantly improve the solubility of the flavonoid quercetin and its release, compared to a conventional α-lactose carrier [33]. The lactose excipient can influence the dissolution properties of the API present in the drug tablet, notably to improve the dissolution behavior of an insoluble API. Different types of lactose-based excipients and co-excipients are available [34][35][34,35].
Lactose is considered a pharmacologically inactive substance, which is the definition of an excipient. However, lactose is not devoid of biological activity. People intolerant to lactose may experience severe clinical symptoms (such as diarrhea and bloating); the disease severity varies considerably among individuals. The intolerance is generally due to the absence or deficiency of the lactase enzyme (lactase-phlorizin hydrolase) found in the small intestinal brush border, which hydrolyses lactose into glucose and galactose. Lactose intolerance is a relatively common gastrointestinal condition, at least in children, caused by the inability to digest and absorb dietary lactose [36][37][36,37]. Lactose can serve as an inducer of protein synthesis in cell cultures [38] and can induce senescence in human lung fibroblasts [39]. Moreover, in recent years the immunological functions of lactose have been delineated, notably its role as a galectin ligand and more specifically as a key regulator of the TIM-3 receptor. The present review highlights the importance of lactose as a checkpoint regulator.
3. The TIM-3 Immune Checkpoint and Its Targeting with Antibodies
Monoclonal antibodies (mAbs) targeting critical immune checkpoints, such as PD-1/PD-L1 and CTLA-4, have significantly ameliorated the treatment of advanced solid tumors, such as lung (NSCLC), skin and liver cancers. Immune checkpoint inhibitors targeting and blocking the interaction of certain cell surface proteins, such as PD-1 expressed on diverse immune cells or PD-L1 expressed on cancer cells, act as brakes on immune responses [40][41][40,41]. A handful of mAbs directed against PD-1 or PD-L1 have been approved for cancer treatment, including pembrolizumab, nivolumab, atezolizumab, camrelizumab and others. Often combined with chemo- or radiotherapy, these mAbs have provided significant survival benefits in cancer patients [42]. However, not all tumors are sufficiently sensitive to anti-PD-1/PD-L1 therapies and durable responses are not always achieved. Therefore, novel immunotherapeutic approaches are needed to combat advanced or relapsed cancers. As for PD-1, other immune checkpoints commonly associated with T cells such as LAG-3 and TIM-3 have been considered [43][44][43,44].
T cell immunoglobulin and mucin domain molecule 3 (TIM-3) is a protein now well exploited as a therapeutic target for cancer immunotherapy [45][46][47][48][45,46,47,48]. This co-inhibitory receptor is expressed on CD4+ and CD8+ T cells which produce interferon-γ (IFN-γ) and on specific innate immune cells (Figure 2). In addition, the expression of membrane TIM-3 has been evidenced at the surface of cancer cells, such as renal, lung, gastric, prostate, and other types of cancer cells. TIM-3 plays major roles in the regulation of tumorigenesis, inflammation, and antitumor immunity [49]. Importantly, TIM-3 is upregulated on CD8+ T cells and Tregs, in tumors treated with radiotherapy and anti-PD-L1 antibodies. The treatment with an anti-TIM-3 mAb concurrently with anti-PD-L1 and radiotherapy induced a significant tumor growth delay, an enhancement of T-cell cytotoxicity, a decrease of Tregs, and improved survival in models of head and neck squamous cell carcinoma [50]. The data suggested that the blockade of Tim-3 can antagonize the resistance of PD-1/PD-L1 blocking therapy [51]. Major anticancer effects have been reported in cases of Tim-3 blockade, in different types of experimental tumors, incusing breast cancer [12][52][12,52], hepatocellular carcinoma [53], and other solid tumors [54]. The blockade of TIM-3 is also a promising approach for the treatment of hematological malignancies, including myelodysplastic syndromes (MDS) and acute myeloid leukemia (AML) [17][55][56][57][17,55,56,57]. In AML, studies have shown an overexpression of TIM-3 on leukemia stem cells (LSC) but not on healthy stem cells [58][59][60][58,59,60]. The blockade of the receptor induces a direct inhibition of AML cell proliferation and restores T cell function [16]. Thus, targeting TIM-3 offers a unique opportunity to target the LSC population resistant to chemotherapy and largely implicated in tumor relapse [61].
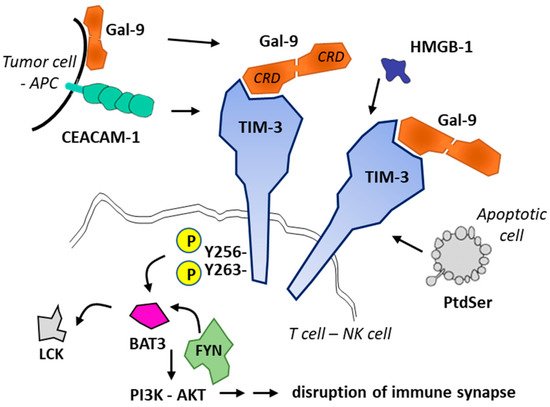
Figure 2. Ligands and signaling of TIM-3. Four TIM-3 ligands have been identified: CEACAM1, phosphatidylserine (PtdSer released from apoptotic cells), HMGB-1 and Gal-9. Gal-9 can be secreted by antigen-presenting cells (APCs) or tumor cells or present at the cell surface. Gal-9 (with two carbohydrate recognition domains (CRD) separated by a short linker) promotes oligomerization of TIM3 and triggers signaling via phosphorylation of residues Tyr256 and Tyr263 in the intracellular domain of TIM3. The phosphorylation releases the adaptor protein BAT3 (HLA-B-associated transcript 3) and allows recruitment of tyrosine kinase FYN, whereas in its ligand-unbound form, TIM-3 interacts with BAT3 and recruits the kinase LCK to maintain T cell activation. Fyn and Bat3 are two adaptor molecules involved in inhibition and activation of Tim-3 downstream signaling, respectively. Gal-9-mediated recruitment of FYN leads to the disruption of immune synapse formation and to cell apoptosis [45].
There are several anti-TIM-3 monoclonal antibodies in (pre)clinical development [62], such as (i) sabatolimab which is currently evaluated for the treatment of advanced solid tumors [63] and myelodysplastic syndromes [64], (ii) the fully human anti-TIM-3 antibody M6903 in preclinical development [65], (iii) LY3321367 currently tested in advanced solid tumors [66], and a few other antibodies [49][67][49,67] (Table 1). Over the past two years, TIM-3 has emerged as an important immune-checkpoint molecule and recent data demonstrated that the receptor plays multiple roles, well beyond CD4+/CD8+ T cells, notably as a key regulator of dendritic cell functions via the regulation of inflammasome activation [68]. The discovery of the many functions of the TIM-3 receptor has encouraged the design and development of different therapeutic entities, monoclonal antibodies but also anti-TIM-3 chimeric antigen receptor (CAR)-directed T lymphocyte therapy [44] and anti-TIM-3 oligonucleotide aptamers [69][70][69,70] (Figure 3).
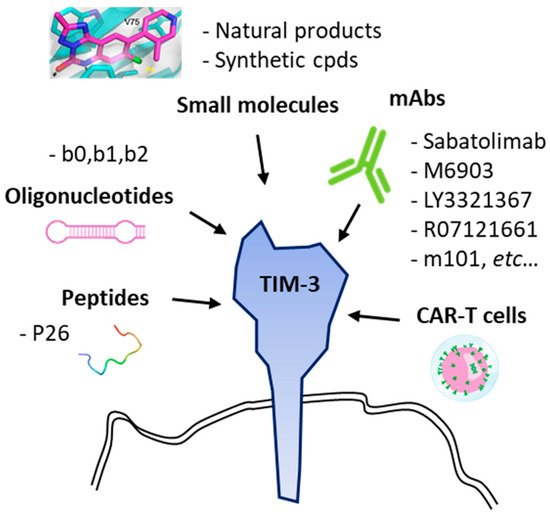
Table 1. Human anti-TIM-3 antibodies in development.
| Anti-TIM-3 Antibodies | Current Development | References |
|---|---|---|
| LY3321367 (Eli Lilly; Indianapolis, IN, USA) |
Phase 1 trial in patients with relapsed/refractory solid tumor, alone or in combination with an anti-PD-L1 mAb. NCT03099109 * | [66][72][66,72] |
| Sabatolimab (MBG453, Novartis, Basel, Switzerland) |
Fast track designation by US FDA for the treatment of patients with myelodysplastic syndromes (MDS) | [73] |
| Phase 1 trial in patients with advanced solid tumor, alone or in combination with anti-PD-1 spartalizumab. | [63] | |
| Phase 1 trial in patients with Acute Myeloid Leukemia (AML). NCT04812548, NCT04623216, NCT04878432, NCT04150029 * | [74] | |
| BMS-986258 (ONO 7807, BMS, Lawrenceville, NJ, USA) |
Fully human anti-TIM-3 mAb, tested in combination with anti-PD-1 nivolumab in patients with advanced solid tumors (Phase 1). NCT03446040 * | |
| Cobolimab (TSR-022, GSK, Brentford, UK) |
Anti-TIM-3 mAb in combination with anti-PD-1 in patients with liver cancer or with a melanoma (Phase 1). NCT04655976, NCT03680508, NCT04139902, NCT02817633 * | |
| Sym023 (Symphogen; Ballerup, Denmark) |
Fully human anti-TIM-3 mAb, in patients with advanced solid tumor malignancies or lymphomas (Phase 1). NCT03489343 * | |
| INCAGN02390 (Incyte, Agenus; Wilmington, DE, USA) |
Phase 1 study to determine the safety, tolerability, and preliminary efficacy in participants with advanced malignancies. Fully human Fc-engineered IgG1k. NCT03652077, NCT04370704. | [75] |
| RO7121661 (Roche; Basel, Switzerland) |
Anti-PD-1/TIM-3 bispecific mAbs, tested in patients with advanced and/or metastatic solid tumors (Phase 1). NCT03708328 * | |
| BGB-A425 (BeiGene Ltd., Beijing, China) |
Humanized anti-TIM-3 mAb, in combination with anti-PD-1 mAb tislelizumab, in patients with advanced solid tumors (phase I/II trial). NCT03744468 * | [76] |
| M6903 | Fully human anti-TIM-3 mAb, without effector function, which blocks binding of TIM-3 to the 3 ligands phosphatidylserine, CEACAM1, and Gal-9. Experimental laboratories studies. | [65] |
| F38.2E2 | Anti-human TIM-3 antibody capable of blocking binding of TIM-3 to phosphatidylserine and CEACAM1. Experimental tool. | [77] |
* ClinicalTrials.gov Identifier.
Anti-TIM-3 biotherapeutic agents have demonstrated potent efficacy in preclinical models and the first clinical data obtained with sabatolimab look promising for the treatment of MDS [78]. A phase 2 trial is ongoing in MDS with sabatolimab combined with azacitidine and venetoclax (NCT04812548). Combined with azacytidine, the anti-TIM-3 antibody might turn to be also useful for the treatment refractory acute myeloid leukemia (AML). A major phase 1–2 trial is currently ongoing (NCT04623216). However, the challenge remains high at present, as no definite proof of long-term clinical efficacy has been reported in AML or MDS. In CD8+ T cells collected from patients with chronic lymphocytic leukemia (CLL), the blockade of an anti-TIM-3 antibody has failed to restore the function of these exhausted T cells [79]. Moreover, a study has shown that the treatment with anti-TIM-3 mAb can inhibit the phagocytic ability of alveolar macrophages in the lungs of mice and thus might cause pneumonitis [80]. The biological and clinical consequences of TIM-3 blockade are not completely understood at present.
Therapeutic antibodies and engineered cells targeting TIM-3 have been designed and are being tested. However, to our knowledge, no small molecules specifically targeting TIM-3 have been clinically developed as yet, despite the potential benefits of the targeting approach in oncology and in other therapeutic fields [14]. The TIM-3-associated immune dysregulation mechanisms of CD4+ or CD8+ T cells have been associated with different inflammatory diseases such as vitiligo [81][82][81,82], rheumatoid arthritis [83][84][83,84], liver diseases [85] and in viral infections such as human papilloma virus (HPV) positive cervical cancer [86]. There is a need for small molecules targeting TIM-3, to reduce the cost of treatment compared to mAbs, to facilitate drug combinations and to allow oral treatments. Thus far, the development of small molecules lags far behind the development of small molecules, as discussed below.