Sacituzumab govitecan (SG) is a third-generation antibody-drug conjugate, consisting of an anti-Trop-2 monoclonal antibody (hRS7), a hydrolyzable linker, and a cytotoxin (SN38), which inhibits topoisomerase 1. Specific pharmacological features, such as the high antibody to payload ratio, the ultra-toxic nature of SN38, and the capacity to kill surrounding tumor cells (the bystander effect), make SG a very promising drug for cancer treatment.
1. Introduction
Human trophoblast cell-surface antigen-2 (Trop-2), also known as tumor-associated calcium signal transducer 2 (TACSTD2), is a membrane receptor encoded by the gene
TACSTD2 located on chromosome 1p32. This cell-surface glycoprotein, originally identified in human trophoblastic tissue, is commonly expressed in a variety of normal and neoplastic epithelial cells
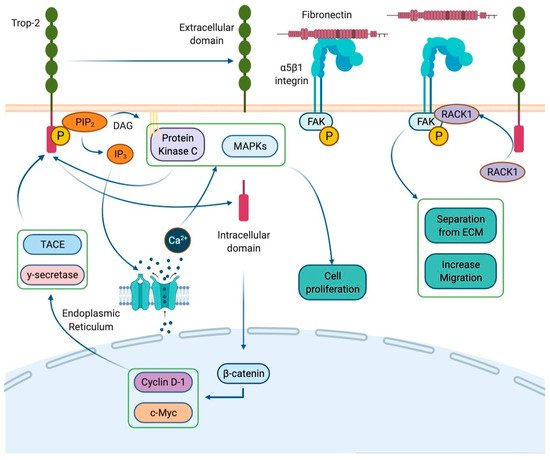
[1]. In physiological conditions, Trop-2 acts as a calcium signal transducer with a cytoplasmatic domain which contains a phosphatidyl-inositol 4,5-bisphosphate (PIP2) binding site. When PIP2 binds to Trop-2, it undergoes phosphorylation by protein kinase C (PKC). This interaction induces PIP2 cleavage into inositol 1,4,5-triphosphate (IP3) and diacylglycerol (DAG) by phospholipase C. In the cytoplasm, IP3 mediates calcium accumulation by opening specific channels in the endoplasmic reticulum. Calcium release recruits mitogen-activated protein kinases (MAPKs) such as ERK1/2, stimulating cell proliferation
[2]. Furthermore, the Trop-2 intra-cytoplasmatic domain undergoes cleavage and translocates in the nucleus, where it colocalizes with β-catenin and up-regulates Cyclin D1 and c-Myc expression, promoting cell cycle progression
[3][4][3,4] (
Figure 1).
Figure 1. Trop-2 signal transduction. Trop-2 is a membrane receptor consisting of an extracellular domain, a transmembrane domain, and an intracellular domain. Its cytoplasmatic domain contains a phosphatidyl-inositol 4,5-bisphosphate (PIP2) binding site. The interaction with PIP2 allows the phosphorylation of the receptor by protein kinase C (PKC). This determines the cleavage of PIP2 into inositol 1,4,5-triphosphate (IP3) and diacylglycerol (DAG) by phospholipase C. IP3 remains in the cytoplasm and mediates the accumulation of intracellular calcium by opening the calcium channels located on the endoplasmic reticulum. Trop-2-induced calcium release leads the recruitment of the mitogen-activated protein kinases (MAPKs), which promote cell proliferation. Furthermore, Trop-2 undergoes the cleavage into two parts by the proteases γ-secretase and TNF-α converting enzyme (TACE). The intracellular domain moves to the nucleus and colocalizes with a β-catenin resulting in the up-regulation of Cyclin D1, which fosters the cell cycle progression. Finally, Trop-2 would seem to be involved in the loss of cell–substrate adhesion, i.e., separation from the extracellular membrane (ECM), and in the promotion of cell migration due the activation of the β1–integrin–RACK1–FAK–Src signaling axis.
In cancer cells, Trop-2 overexpression stimulates growth and metastatic potential by promoting cell proliferation and migration. This protein is also involved in the epithelial-to-mesenchymal transition (EMT) since it determines E-cadherin down-regulation and vimentin expression, resulting in cell migration and stem cell-like properties
[5][6][7][8][5,6,7,8]. Additionally, Trop-2 enhances cellular motility and invasion through the up-regulation of integrin-dependent signaling
[3][4][3,4]. Although Trop-2 overexpression seems to be related to enhanced tumor aggressiveness and inferior prognosis, it can also be exploited as a target for anticancer therapies
[9][10][11][12][13][9,10,11,12,13]. In the last decade, many in vitro, ex vivo, and in vivo evaluations posed the bases for Trop-2-directed therapies in solid tumors
[14][15][16][17][14,15,16,17]. In particular, studies on animals revealed the potential activity of antibody–drug conjugates (ADC) targeting Trop-2 and established their acceptable safety profile
[14]. Given the promising preclinical evidence, some of these compounds warranted further clinical development
[18].
Sacituzumab govitecan (SG), formerly known as IMMU-132, is a third-generation ADC specifically targeting Trop-2. It consists of an anti-Trop-2 humanized antibody (hRS7, sacituzumab) and a cytotoxic payload (SN38, govitecan) joined by a pH-dependent hydrolysable linker
[17]. Unlike first-generation and second-generation ADCs, which typically contain two to four cytotoxins per antibody, hRS7 binds seven to eight molecules of SN38
[17]. Compared to older ADCs, SG is linked with a more toxic payload, effective in the range of pM instead of nM
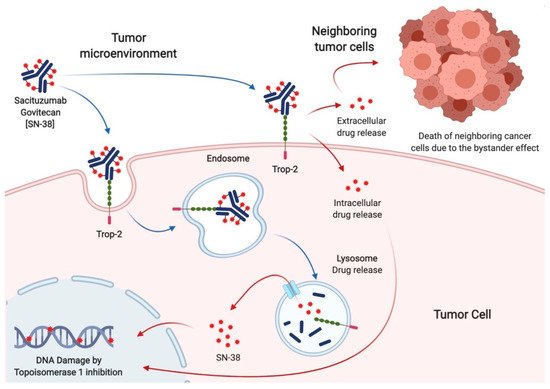
[19][20][19,20]. Indeed, SN38 is a topoisomerase I inhibitor, 100 to 1000-fold more toxic than its precursor irinotecan. The interaction between Sacituzumab and Trop-2 leads to the internalization of the cytotoxic payload into tumor cells, where it induces double-strand DNA breaks and apoptosis during the S phase of the cell cycle. Additionally, due to the acidic cancer environment, the pH-dependent linker can release SN38 from hRS7 in the tumor surroundings. This allows the killing of tumors cells lacking Trop-2 overexpression, a phenomenon known as the bystander effect, which increases SG activity by overcoming the heterogeneity of Trop-2 expression
[20] (
Figure 2).
Figure 2. Mechanism of action of Sacituzumab govitecan. The humanized monoclonal antibody (hRS7) allows the internalization of the cytotoxic payload (SN38) into the tumor cell after binding with the surface receptor Trop-2. The hRS7 complex bound to Trop-2 is internalized through an endosomal vesicle that carries it to the lysosomes. Free SN-38, released after antibody catabolism and linker hydrolysis within the lysosome, induces DNA damage due to the inhibition of topoisomerase 1. Furthermore, the hydrolyzable linker enables SN-38 to be released into the tumor microenvironment. Given its membrane-permeable nature, free SN-38 can also exert its effect on neighboring cancer cells. Thus, tumor cells that express Trop-2 on the surface undergo the cytotoxic effect of SG by the intracellular uptake of SN38, whereas the adjacent ones experience this effect by its extracellular release (the so-called bystander effect).
2. Sacituzumab Govitecan in Breast Cancer
Sacituzumab govitecan has shown remarkable activity in BC patients since the earliest phases of its development.
The IMMU-132-01 phase I/II basket trial enrolled subjects with advanced solid tumors and set the recommended phase II dose (RP2D) of SG at 10 mg/Kg intravenously on days 1 and 8 of each 21-day cycle
[21][22][23][21,27,28]. Of the 178 patients treated in the dose escalation and expansion parts, 53 (29.8%) had TNBC. Among them, those treated at the RP2D achieved a 31.4% objective response rate (ORR) and a 54.8% clinical benefit rate (CBR)
[22][27]. The trial was then expanded in a selected cohort of patients, including metastatic TNBC (mTNBC)
[24][25][29,30]. Preliminary results in 69 women with mTNBC who received at least one previous line of therapy showed an ORR of 30%. Final results were obtained on 108 mTNBC patients treated in the third or later line for metastatic disease. In this heavily pretreated population, SG granted a median progression-free survival (mPFS) of 5.5 months (4.1–6.3 95% CI), a median overall survival (mOS) of 13.0 months (11.2–13.7 95% CI), and a 33.3% ORR
[25][30]. The subsequent open-label randomized phase III trial (ASCENT) compared SG with single-agent chemotherapy of physician’s choice (capecitabine, eribulin, gemcitabine, vinorelbine) in 468 mTNBC patients, pretreated with at least two lines of therapy. Median PFS, the primary endpoint, was 5.6 months in the SG arm and 1.7 months in the control arm (hazard ratio (HR) 0.41; 0.32–0.52 95% CI;
p < 0.001), while mOS was 12.1 months with SG and 6.7 months with chemotherapy (HR 0.48; 0.38–0.59 95% CI;
p < 0.001). In line with previous evidence, SG determined a 35% ORR, compared to 5% with standard treatment
[26][31].
SG also showed signs of activity in patients with hormone receptors positive (HR+)/human epidermal growth factor 2 negative (HER2-) mBC patients, which represented a prespecified subpopulation in the IMMU-132-01 trial. In this study, 54 women with HR+/HER2- mBC received SG after endocrine-based therapy and at least one chemotherapy line. At a median follow-up of 11.5 months, mPFS was 5.5 months (3.6–7.6 95% CI) and mOS was 12.0 months (9.0–18.2 95% CI). Objective responses were observed in 31.5% of patients
[27][32]. Given these encouraging results, a randomized phase III trial (TROPiCS-02, NCT03901339) is currently ongoing to compare SG with treatment of the physician’s choice (capecitabine, eribulin, gemcitabine, vinorelbine) in HR+/HER2- pretreated mBC
[28][33].
Many other trials are ongoing to evaluate SG alone or in combination with other drugs in BC patients, both in the advanced and early settings (Table 1).
Table 1. Selected published and ongoing trials testing Sacituzumab govitecan in breast cancer.
|
| Trial Name |
|
| Phase |
|
| Study Treatment |
|
| Study Population |
| (Number Enrolled If Available) |
|
| Study Design |
|
| Status |
| (Ref. If Published) |
|
|
| NCT01631552 |
|
| I/II |
|
| SG |
|
|
|
Ongoing |
|
|
Legend: BC: breast cancer; HER2-: HER2 negative; HR+: hormone receptor positive; m: metastatic; NACT: Neoadjuvant therapy; pCR: pathologic complete response; SG: Sacituzumab govitecan; TNBC: triple-negative breast cancer; wo: without.
3. Sacituzumab Govitecan in Other Solid Tumors
Published data about the use of SG in solid tumors other than BC are still limited. However, many clinical trials are ongoing
[29][34] (
Table 2).
Table 2. Selected published and ongoing trials testing Sacituzumab govitecan in solid tumors other than breast cancer.
|
| Table |
|
| Phase |
|
| Study Treatment |
|
| Study Population |
| (Number Enrolled If Available) |
|
| Study Design |
|
| Status |
| (Ref. If Published) |
|
|
| Solid Tumors |
| (515) |
|
| Open label, single group |
|
|
|
| NCT04617522 |
|
| 1 |
| Published |
| SG |
|
| Advanced solid tumors and moderate liver impairment |
| [ |
| Open label, non-randomized |
| 25][27]
| [30,32]
|
|
| Ongoing |
|
| NCT04039230 |
|
| I/II |
|
|
| NCT04724018 |
|
| 1 |
| SG + Talazoparib |
|
| SG + Enfortumab vedotin |
| mBC |
|
| Open label, single group |
|
| mUC after platinum and anti-PD1/L1 |
| Ongoing |
|
|
| Open label, single group |
|
| Ongoing |
|
| NCT03424005 |
|
|
|
| NCT03995706 |
| Ib/II |
|
|
| 1 |
| SG + Atezolizumab |
|
| SG |
| mTNBC |
|
|
| Breast cancer with brain metastases and glioblastoma |
| Open label, randomized multi-cohort |
|
| Ongoing |
|
|
| Open label, single group |
|
| Ongoing |
|
| NCT03992131 |
| (SEASTAR) |
|
|
| NCT01631552 |
| (IMMU-132-01) |
| Ib/II |
|
| 1/2 |
| SG + Rucaparib |
|
|
| SG |
| Advanced solid tumors |
|
| Epithelial cancers |
| Open label, non-randomized |
|
| Ongoing |
|
|
|
| Open label, non-randomized |
|
| Published [22]
| [27]
|
| NCT04927884 |
|
| Ib/II |
|
| SG |
|
| mTNBC |
|
|
| NCT04826341 |
|
| 1/2 |
|
| SG + Berzosertib |
|
| Advanced solid tumors > 1 L |
| SCLC after platinum, |
| HRD cancers after PARPi |
| Open label, single group |
|
| Open label, non-randomized |
| Ongoing |
|
|
| Ongoing |
|
| NCT04647916 |
|
| II |
|
|
| NCT04863885 |
| SG |
|
|
| 1/2 |
| HER2-BC and brain metastases |
|
| Open label, single group |
|
| Ongoing |
|
|
| SG + IPI/NIVO |
|
| 1L cisplatin-ineligible mUC |
|
| Open label, non-randomized |
|
| Ongoing |
|
| NCT04468061 |
| (Saci-IO) |
|
| 2 |
|
| SG + Pembrolizumab |
| vs. Pembrolizumab |
|
|
| NCT03869190 |
| (MORPHEUS-UC) |
|
| 1/2 |
| mTNBC |
|
| SG + Atezolizumab |
| Open label, randomized |
|
| mUC |
| Ongoing |
|
|
|
| Open label, randomized, multi-cohort |
|
| Ongoing |
|
| NCT04448886 |
| (Saci-IO HR+) |
|
|
| NCT03992131 |
| 2 |
|
(SEASTAR) |
| SG + Pembrolizumab |
| vs. Pembrolizumab |
|
|
| 1b/2 |
| HR+/HER2-mBC |
|
| SG + Rucaparib |
|
| Advanced or metastatic solid tumors |
| Open label, randomized |
|
| Open label, non-randomized |
| Ongoing |
|
|
| Ongoing |
|
| NCT04230109 (NeoSTAR) |
|
| 2 |
|
| SG + Pembrolizumab |
| vs. Pembrolizumab |
|
| Localized TNBC |
|
| Open label, randomized |
|
| Ongoing |
|
|
| NCT02574455 (ASCENT) |
|
| 3 |
|
| SG |
| vs. Chemotherapy |
|
| mTNBC |
| (529) |
|
| Open label, randomized |
|
| Published [26][27]
| [31 |
|
| NCT03337698 |
| (MORPHEUS-Lung) |
|
| 1b/2 |
|
| SG + Atezolizumab |
|
| mNSCLC |
|
| Open label, randomized |
|
| Ongoing |
|
,32]
|
|
|
|
| NCT03547973 |
| (TROPHY U-01) |
|
| 2 |
|
| SG |
|
| mUC after platinum or anti-PD1/L1 (113) |
|
| Open label, non-randomized |
|
| Published [30]
| [25]
|
NCT03901339 (TROPiCS-02) |
|
| 3 |
|
| SG |
| vs. Chemotherapy |
|
| HR + HER2-mBC |
|
| Open label, randomized |
|
| Ongoing |
|
|
| NCT04251416 |
|
| 2 |
|
| SG |
|
| Persistent/recurrent EC |
|
| Open label, single group assignment |
|
| Ongoing |
|
| NCT04595565 (SASCIA) |
|
|
| NCT03964727 |
| (TROPiCS-03) |
| 3 |
|
|
| 2 |
| SG |
| vs. Chemotherapy |
|
| SG |
| HER2-/BC wo pCR after NACT |
|
| Open label, randomized |
|
| Metastatic solid tumors |
|
| Open label, single group assignment |
|
| Ongoing |
|
|
| NCT04559230 |
|
| 2 |
|
| SG |
|
| Recurrent glioblastoma |
|
| Open label, single group assignment |
|
| Ongoing |
|
|
| NCT03725761 |
|
| 2 |
|
| SG |
|
| Castration-resistant prostate cancer after second-generation ADT |
|
| Open label, single group assignment |
|
| Ongoing |
|
|
| NCT04527991 |
| (TROPiCS-04) |
|
| 3 |
|
| SG |
| vs. TAX/TXT/Vinflunine |
|
| Metastatic or locally advanced unresectable UC |
|
| Open label, randomized |
|
| Ongoing |
|
Legend: 1/2L: first or second line; ADT: androgen deprivation therapy; HRD: homologous repair deficiency; IPI/NIVO: ipilimumab + nivolumab; m: metastatic; EC: endometrial cancer; NSCLC: non-small cell lung cancer; PARPi: poly (ADP-ribose) polymerase-inhibitors; SCLC: small cell lung cancer; SG: Sacituzumab govitecan; TAX: paclitaxel; TXT: docetaxel; UC: urothelial carcinoma.
Additional preclinical evidence and limited clinical experiences suggest a potential role for SG in the treatment of gynecological malignancies, including cervical and endometrial cancer
[31][32][33][26,38,39], as well as in salivary gland tumors
[34][23].