1.1.1. The Interdental Space
Bridles are usually adjusted so that the bit is in contact with a largely tooth-free segment of the gums on each side of the mandible, i.e., behind the incisors and in front of the premolars in the so-called “interdental space”
[2][3][4][5][7,104,105,106]. The gums are modified periosteum, i.e., the membrane that surrounds bone, and are richly supplied with nociceptors
[1][6][99,107]. Accordingly, rein tension transmitted as bit pressure applied to the mandibular gums can readily generate intense pain, especially as the pressure per unit area of direct bit–gum contact is amplified by the round cross-section of the bit and the usually narrow upper edge of the interdental mandible
[2][7][3][8][7,11,104,108].
The magnitude of this amplification can be estimated by utilising the following information.
- (1).
-
The established relationship between tension (T, units N), mass (m, units kg) and gravitational acceleration (g = 9.8 metres/sec
2), which is “T = mg” or “T = 9.8 m”
[9][109].
-
- (2).
-
Known rein tensions in various situations. Examples include zero N (Newtons) with a loose rein, maxima of 51 to 166 N, and mean values that ranged from 9 to 59 N
[10][11][12][13][14][15][110,111,112,113,114,115].
-
- (3).
-
An estimated area of bit–gum contact on the interdental space (CA
bg) of 0.387 cm
2 [16][2], which is equivalent to a 6.22 × 6.22 mm square.
-
The mass equivalent (kg) of rein tension (N) may be calculated using a different form of the above equation, namely “m = T / 9.8”, and the mass per unit cross-sectional area (kg/cm
2) using “m / 0.387”. Thus, the mass equivalents of the above values are a minimum of zero kg, a range of maxima of 5.2 to 16.9 kg, and a range of overall mean values of 0.9 to 6.0 kg, respectively. The related figures for mass per unit area are zero kg/cm
2 for the minimum, 13.4 to 43.7 kg/cm
2 for the range of maximum values, and 2.3 to 15.5 kg/cm
2 for the range of overall mean values. The estimated amplification factor is 2.58. Apart from the “loose rein” minimum, and a report of estimated mean bit pressures that were mostly between 0.93 and 1.1 kg/cm
2 [17][116], most of the above bit pressures would be painful, some of them exceptionally so. It is therefore of interest that, with one exception
[15][115], bit-induced pain was not mentioned in any of the above papers on rein tension
[10][11][12][13][14][17][18][110,111,112,113,114,116,117].
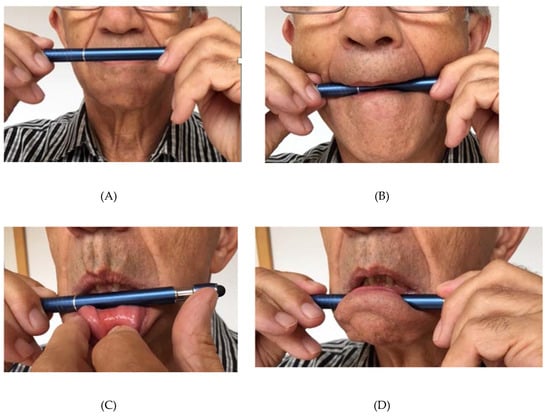
Readers may gain a personal insight into the likely intensity of such pain by conducting on themselves what has come to be known as the “Mellor pen-test”. This test is intended to simulate the compressive effects of bit pressure applied to the gums of the interdental space of a horse. It involves applying pressure to the barrel of a pen placed against the gums below the front incisor teeth of the lower jaw (
Figure 1). In common with the experiences of audiences totaling at least 450 addressed by the author to date (e.g., see
[19][118]), it is anticipated that the vast majority of readers will find that intense pain may be generated by low pressures.
Figure 1. The ‘Mellor pen test.” This simulates bit pressure applied to the gums of the interdental space of the horse. Gums are exquisitely sensitive to painful stimuli, including compression. Rein tension transferred to the bit in contact with the gums of the interdental space causes pain. (A) Position 1: Hold the pen in front of your mouth; (B) Position 2: Open your mouth, place the pen where the upper and lower lips meet on each side, and then push the pen towards the back of your throat. No gum contact, no significant pain; (C) Position 3a: Roll your bottom lip down and locate the pen on your gum, below your central incisors; (D) Position 3b: Now release your lip and with both hands holding the pen, apply compressive pressure to your gum, carefully increasing the pressure in steps from very low until the pain is too intense to continue. How much compression-induced pain could you stand?
As a further exercise, first access a set of top-loading kitchen scales for weighing up to at least 3kg. With an index finger pointing down vertically, place its tip (not the distal fingerprint surface) on the weighing tray so that the bone of the terminal phalanx bears most of the pressure; and then press directly downward to hold the scale readings successively at 1, 2 and 3 kg, taking a break between each level. Bearing in mind that the fingertip is much less immediately susceptible to pain-inducing pressure than are the exquisitely sensitive gums, readers should note how long they can maintain these scale readings before pain compels withdrawal. Now compare these scale levels with the values for bit pressure per unit area (kg/cm2) given above and note that 3 kg/cm2 is considerably less than most of them.
Finally, the reader may also wish to imagine lying flat on their back on a raised platform with sufficient space under it to suspend a small carry-on aircraft flight bag. The bag is attached to light reins fixed to each end of a metal bit located, as with the “Mellor pen test”, on the mandibular gums below the front incisor teeth (Figure 1). Now imagine that the weight of the bag is increased from 2 up to a 7 kg carry-on maximum. Then, imagine that the weight is increased progressively to a 20 kg maximum for stowed luggage, noting that this is less than half the figure of 43.7 kg/cm2 derived from the 166 N maximum rein tension referred to above.
It is anticipated that the combined results of these three exercises will speak for themselves.
The mandibular periostitis (bone spur formation) observed in the interdental space of horses wearing bitted bridles and its absence or virtual absence in free-roaming or feral equids, when taken together, provide evidence of significant traumatic impacts of bit use. Three postmortem studies of equid mandibles illustrate this: (1) interdental bone spurs were found in ~88% of 32 working horses but there were none in 28 Przewalski horses
[20][119]; (2) interdental space roughness was reported in 48% of 87 Warmbloods or trotters, in 25% of eight donkeys, but only in 7% of 68 zebra
[8][108]; and (3) spurs were observed in ~61% of mandibles from 66 domestic horses, but none were seen in 12 feral and Przewalski horses
[2][7]. In addition, live assessment of oral lesions revealed that 28–30% of 50 polo ponies and 50 racehorses had interdental bone spurs, which were generally more severe in the racehorses
[21][120]. Finally, in the first postmortem study mentioned above, the erosion of enamel and dentine of the first mandibular premolar, indicative of bit wear, was observed in 62% of 29 working horses
[20][119]. Likewise, in the third postmortem study above, premolar erosion was observed in 61% of the 66 domestic horse mandibles, such that, overall, 88% of those mandibles exhibited either bone spurs or premolar erosion, or both
[2][7].
The formation of bone spurs in affected horses is apparently due to inflammation associated with repeated incidents of bit-induced bruising, laceration, and/or ulceration of the interdental gums
[2][22][23][24][7,121,122,123]. Such gum lesions reportedly occurred in 26% of 261 Trotters observed after a race
[25][124], increased from 8% before to 31% after events in 77 competition horses
[26][125], and were more common and severe in racehorses than polo ponies
[21][120]. All such lesions are painful
[6][107], and human experience would suggest that the intensity of that pain would be increased when there is further direct compressive contact between these lesions and a bit. Likewise, in view of the dense nociceptive innervation of the dentine and, to a lesser extent, the tooth pulp
[27][126], further compressive bit contact with significantly worn teeth (mentioned above
[2][20][7,119]) would also be likely to increase the intensity of any associated pain.
1.1.2. The Tongue
The tongue, being densely supplied with mechanoreceptors
[1][99], exhibits exceptional tactile sensitivity which underlies its haptic functions of delicate investigation and selective manipulation of food and other objects both inside and outside the mouth. It is also well supplied with nociceptors, although a reported low responsiveness of horses to severe lacerations in the mobile rostral portion of the tongue, amounting in some cases to near amputation
[3][28][104,127], suggests that nociceptor density in the tongue may be less than in the periosteal gums of the interdental space
[1][6][29][99,107,128]. However, this does not imply that the tongue is insensitive to painful stimuli, because injuries such as puncture wounds, abscesses, or ulcers located caudally in the tongue can apparently cause enough pain to seriously impede chewing and swallowing
[28][127].
Nevertheless, several observations suggest that the tongue may be somewhat protected from bit-induced penetrative injuries. Studies that reveal significant bit-related injuries at multiple oral sites report no or very low occurrences of significant tongue lacerations or ulcers
[21][25][26][30][31][120,124,125,129,130]. The tough keratinized squamous epithelial lining of at least the dorsal surface of the tongue
[32][131] may contribute to this, but it might also make bruises from non-penetrative bit-related compression more difficult to detect.
Bruising of the tongue would likely occur at its lateral edges when the horse uses it to partially cushion the interdental gums against significant bit pressure. Under bit pressure, the tongue may lie ventrally across the full width of the oral cavity covering the interdental gums on each side, such that, at its edges, the tongue may become painfully compressed between the bit and the mandible
[7][26][33][11,125,132]. Although this might reduce the overall pain experienced, it would not eliminate it. This is because narrow under-the-bit compression across the width of the tongue between its lateral edges would still be painful, and some pain-inducing nociceptor stimulation may still occur within the highly pain-sensitive interdental spaces
(see Section 4.1.1), despite cushioning by the tongue.
Another strategy apparently deployed by horses to ameliorate bit-induced pain is to manoeuvre the tongue to lie above or behind the bit
[7][34][35][11,133,134]. The position above the bit would potentially enable the frenulum and adjacent sublingual tissues to absorb some of the bit pressure generated by rein tension. Although this would itself be painful, this strategy may be sufficient to reduce the bit pressure applied directly to the interdental gums and/or to the premolars for the outcome to be a net reduction in pain. That a significant proportion of horses utilize this “tongue over the bit” strategy is indicated by the relatively frequent use of tongue ties to prevent them from doing so
[35][36][37][134,135,136]. Thus, 72% of Thoroughbred trainers in Australia reportedly used tongue ties with over 30% of horses wearing a tongue tie at least once
[35][134]. Moreover, once applied to a racehorse, a tongue tie was used in 84% of their subsequent races. Overall tongue tie use was greater in jumps races (45%) than in flat races (32%)
[37][136]. In the United Kingdom, tongue ties were used over a 2-year period in 5% of horses, and after being used once they were applied in an average of 77% of the races run by those horses during the following year
[36][135]. Advocates for this intervention often proffer the justification that “tongue-tied” racehorses are more responsive to the bit and are therefore easier to control, and/or that they are less susceptible to compromised breathing resulting from dorsal displacement of the soft palate which impedes their racing performance
[35][36][37][38][39][134,135,136,137,138]. Note however that contrary evidence exists, which shows that bit-induced mouth pain makes many horses difficult to control
[7][11] (Section 5).
Nevertheless, regarding the greater purported sensitivity to the bit and effectiveness of control, advocates of this intervention reason that: (1) bit-induced mouth pain is used to control potentially unruly horses; (2) some horses relocate their tongues over the bit to alleviate the pain; (3) “tongue over the bit” horses are less responsive to the bit and are therefore harder to control; and (4) when tongue ties are used to restore a “bit over the tongue” configuration, responsiveness to the bit and effectiveness of control return. However, so does a greater intensity of bit-induced pain. It therefore follows that tongue tie use enables its advocates to impose on horses, or threaten them with, bit-induced pain at noxious intensities designed to achieve the sense of control they seek. Note in addition that use of tongue ties is itself aversive and likely adds significantly to the pain.
Tongue ties are usually applied by grasping the tongue, drawing it sideways out of the mouth, winding the tie around the tongue one or more times and securing it below the mandible ventral to the interdental space; the purposes are to hold the tongue flat against the ventral surface of the oral cavity and to stop it from being retracted
[40][139]. Nylon stocking, leather, or rubber bands are used. It is common for a length of tongue beyond the tie to protrude from the horse’s mouth. Problems with tongue tie use, reported by nearly a quarter of Australian Standardbred trainers, include lacerations, bruising and swelling of the tongue, difficulty swallowing, and stress behaviours
[40][41][139,140]. It is proposed here that the stress behaviours indicate pain-related aversion to the tie. The likely sources of significant pain include the following: lengthwise over-stretching of the tongue during application of the tie; compression of the tongue directly under the tie; impeded blood flow to the rostral tongue while the tie is in place and its restoration when the tie is removed (ischaemic pain); and pain linked to any bruising and lacerations. In addition, the tie narrows the tongue medially, which prevents it from overlying the interdental space on each side, thereby increasing the likelihood that, under rein tension, the bit would have direct contact with the highly pain-sensitive periosteal gums .
1.1.3. The Commissures of the Lips and the Buccal Mucosa
The incidence of commissure lesions has been reported in several studies. (1) Acute lesions were apparent in 64% of Finnish trotters, where blood was visible on the bit or the wound in 10% that had the most severe lesions
[25][124]. (2) About 9% of Danish horses in dressage, show jumping, eventing, and endurance competitions had commissure lesions, some of which were accompanied by visible blood
[31][130]. (3) In 50 polo ponies and 50 racehorses, commissure ulcerations numbered 15 and 53, respectively, where both the prevalence and severity of the lesions were greater in the racehorses than the polo ponies
[21][120]. The prevalence in these racehorses was later estimated to be ~25%
[25][124]. (4) Mild, apparently older lesions, both inside the commissures and in the adjacent buccal mucosa, were found in 26% of Icelandic horses prior to prescribed gait competitions, and a further 4% had severe lesions in the buccal mucosa
[26][125]. And (5), buccal ulceration or evidence of previous ulceration adjacent to maxillary molars was apparent in 94% of ridden Swedish horses
[30][129]. These observations and the finding that no fresh lesions were observed in brood mares that had not recently been used wearing a bitted bridle
[30][129] implicate bit use as a cause
[25][124].
Commissure and adjacent buccal bruising, laceration, ulceration, and bleeding provide clear evidence of prior damaging impacts of bit pressure on the nociceptors of the internal mucosal and external lip tissues sufficient to cause significant pain. Moreover, this pain would be intensified by bit and/or molar tooth pressure on any recently formed lesions. A further indication of high bit pressure on the commissures is the readily observable stretching of the lips to up to double their resting non-bitted length when rein tension is applied
[42][7][43][44][45][1,11,96,97,141]. Note that this stretching, whether short-lived or sustained, would itself cause pain. The reader may confirm this by repeating the “Mellor pen test” position 2 (
Figure 1B), but instead of applying little pressure, for this purpose the pen should be pushed carefully towards the back of the mouth as far and for as long as the induced lip-stretching pain will allow.