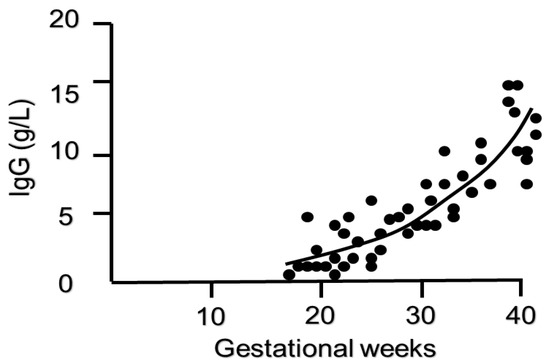
IgG antibodies can cross and do cross the placenta during pregnancy from the mother to the fetus. The passage starts by the end of the first trimester and continues throughout pregnancy. This is a manner by which the fetus gets passive humoral immunity from the mother. In the early neonatal period, these transferred maternal antibodies will act as a defense and help the developing immunity of the baby. While they are short-lived and cleared from the neonatal circulation within several months, they may be very helpful.
A down-side is that in certain maternal autoimmune conditions auto-antibodies seem to have the capacity to hijack the transfer mechanism. It is the case for anti-Ro antibodies. These antibodies are frequent in women with systemic lupus erythematosus and/or Sjogren syndrome. They can lead to fetal atrioventricular block.
- anti-Ro
- fetal heart block
- covid-19
- passive immunity
1. Introduction
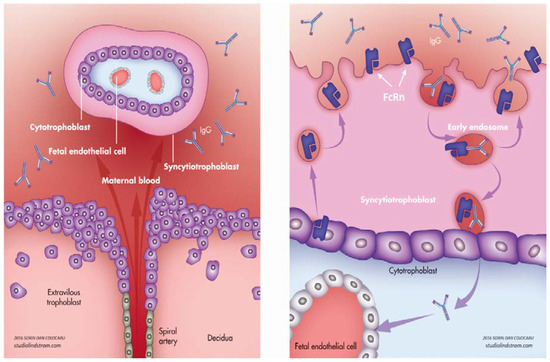
2. Physiological Transfer of IgG
2.1. Role of FcRn
2.2. Timing of IgG Transfer and Other Influencing Factors