Bronchoscopy has several major diagnostic and therapeutic indications in pulmonology. However, it is an aerosol-generating procedure that places healthcare providers at an increased risk of infection. Now more than ever, during the spread of the coronavirus disease 2019 (COVID-19) pandemic, the infectious risk during bronchoscopy is significantly raised, and for this reason its role in diagnostic management is debated.
- COVID-19
- diagnostic strategies
- bronchoscopy
1. Introduction
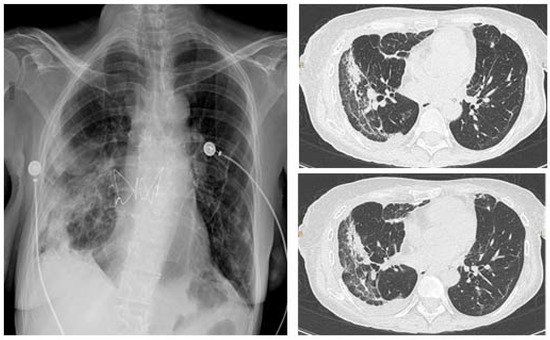
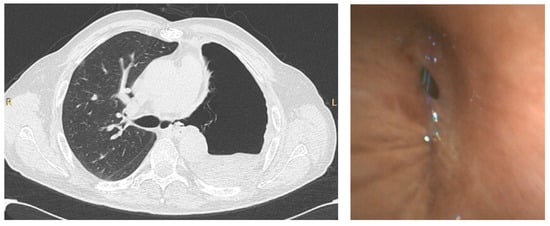
The gold standard diagnostic tests for detecting current SARS-CoV-2 infections are based on reverse transcriptase polymerase chain reaction (RT-PCR) with samples collected from the upper respiratory tract (nasopharyngeal nasal or oropharyngeal swabs) [7][1]. Indeed, in the prodromal phase, when the contagiousness is higher, the active viral replication of the virus can be localized and identified in the upper airways [8][2]. However, these tests do not have high sensitivity, ranging from 32 to 63% due to wrong handling of the specimen, sample collection during the late phase of the disease, or low viral load [9,10][3][4]. Among patients with clinical suspicion of COVID-19, with negative nasopharyngeal swabs, samples from the lower respiratory tract using bronchoscopy could increase sensitivity and help to achieve a correct diagnosis. Indeed, Wang and colleagues compared positive RT-PCR tests on different clinical specimens in patients with COVID-19 and showed that bronchoalveolar lavage fluid (BALF) was positive in 93% of cases, compared to sputum (72%), nasal (63%), and pharyngeal swab (32%) [10][4].
2. Role of Bronchoscopy in the MDianagement ognostic Work-up of COVID-19 Infection
3. Role of Bronchoscopy in the Management of COVID-19 Infection
| Suspected COVID-19 | Confirmed COVID-19: Emergent Indication |
Confirmed COVID-19: Urgent Indication |
|---|---|---|
| Confirm or exclude COVID-19 in those with a negative upper respiratory tract swab, but clinical signs and symptoms consistent for COVID-19 pneumonia [1] | Moderate symptomatic or worsened tracheal/bronchial stenosis; migrated stent | Lung cancer diagnosis (lung mass or mediastinal/hilar lymphadenopathy) |
| Confirm suspected COVID-19 cases with a negative upper respiratory tract swab, but typical clinical and radiological features [5][9][10][11][12][13][14] | Symptomatic central airway obstruction (i.e., due to mucus plug) or lobar atelectasis | Foreign object aspiration |
| Confirm or exclude COVID-19 in those with a negative upper respiratory tract swab and clinical signs and symptoms possible for COVID-19 pneumonia, but an alternative diagnosis could also be considered [1] | Hemoptysis or bloody mucus from the lower respiratory tract | Suspected concomitant pulmonary infection in immunosuppressed patients (i.e., fungal co-infection) |
References
- COVID-19 Treatment Guidelines National Institute of Health. Available online: https://www.covid19treatmentguidelines.nih.gov (accessed on 16 August 2021).
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469.
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tanet, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020, 323, 1843–1844.
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40.
- Group of Interventional Respiratory Medicine, Chinese Thoracic Society. Expert consensus for bronchoscopy during the epidemic of 2019 novel coronavirus infection (Trial version). Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, E006.
- Lentz, R.J.; Colt, H. Summarizing societal guidelines regarding bronchoscopy during the COVID-19 pandemic. Respirology 2020, 25, 574–577.
- Mondoni, M.; Papa, G.F.S.; Rinaldo, R.; Faverio, P.; Marruchella, A.; D’Arcangelo, F.; Pesci, A.; Pasini, S.; Henchi, S.; Cipolla, G.; et al. Utility and safety of bronchoscopy during the SARS-CoV-2 outbreak in Italy: A retrospective, multicentre study. Eur. Respir. J. 2020, 56, 2002767.
- Torrego, A.; Pajares, V.; Fernandez-Arias, C.; Vera, P.; Mancebo, J. Bronchoscopy in patients with COVID-19 with invasive mechanical ventilation: A single-center experience. Am. J. Respir. Crit. Care Med. 2020, 202, 284–287.
- Chang, S.H.; Jiang, J.; Kon, Z.N.; Williams, D.M.; Geraci, T.C.; Smith, D.E.; Cerfolio, R.J.; Zervos, M.; Bizekis, C. Safety and efficacy of bronchoscopy in critically ill patients with coronavirus disease 2019. Chest 2021, 159, 870–872.
- Wahidi, M.M.; Lamb, C.; Murgu, S.; Musani, A.; Shojaee, S.; Sachdeva, A.; Maldonado, F.; Mahmood, K.; Kinsey, M.; Sethi, S.; et al. American Association for Bronchology and Interventional Pulmonology (AABIP) Statement on the Use of Bronchoscopy and Respiratory Specimen Collection in Patients With Suspected or Confirmed COVID-19 Infection. J. Bronchol. Interv. Pulmonol. 2020, 27, e52–e54.
- Darwiche, K.; Ross, B.; Gesierich, W.; Petermann, C.; Huebner, R.; Grah, C.; Gompelmann, D.; Hetzel, J.; Holland, A.; Eisenmann, S.; et al. Recommendations for Performing Bronchoscopy in Times of the COVID-19 Pandemic-Update 12/2020. Pneumologie 2021, 75, 187–190.
- Cordovilla, R.; Alvarez, S.; Llanos, L.; Cases, E.; Ares, A.N.; Perez, D.D.; Flandes, J. Separ and aeer consensus recommendations on the use of bronchoscopy and airway sampling in patients with suspected or confirmed COVID-19 infection. Arch. Bronconeumol. 2020, 56 (Suppl. S2), 19–26.
- Asociación Argentina de Broncoesofagología. RECOMENDACIONES Asociación Argentina de Broncoesofagologia (AABE) basados en la Wold Association for Bronchology and Interventional Pulmonary WABIP para el Manejo de Pacientes con COVID 19 en Situación de Pandemia. Available online: http://www.broncoscopia.org.ar/recomendaciones-asociacion-argentina-de-broncoesofagologia-aabe-basados-en-la-wold-association-for-bronchology-and-interventional-pulmonary-wabip-para-el-manejo-de-pacientes-con-covid-19-en-situacio (accessed on 16 August 2021).
- Gasparini, S.; Failla, G.; Serafino Agrusa, L.; Corcione, N.; Position Paper AIPO-ITS. Ruolo e Modalità di Esecuzione della Broncoscopia nella Pandemia da COVID-19. Position Paper 2020. Available online: http://www.aiponet.it/editoria/aipo-ricerche-edizioni/prodotti-editoriali/127-documenti-covid-19/2489-ruolo-e-modalita-di-esecuzione-della-broncoscopia-nella-pandemia-da-covid-19.html (accessed on 16 August 2021).
- Ora, J.; Puxeddu, E.; Cavalli, F.; Giorgino, F.M.; Girolami, A.; Chiocchi, M.; Sergiacomi, G.; Federici, M.; Rogliani, P. Does bronchoscopy help the diagnosis in COVID-19 infection? Eur. Respir. J. 2020, 56, 2001619.
- Larriva, M.A.-D.; Martín-DeLeon, R.; Royo, B.U.; Fernández-Navamuel, I.; Velando, A.G.; García, L.N.; Clemente, C.C.; García, F.A.; Codern, A.R.; Fernández-Arias, C.; et al. The role of bronchoscopy in patients with SARS-CoV-2 pneumonia. ERJ Open Res. 2021, 7, 00165–02021.
- Cocconcelli, E.; Biondini, D.; Giraudo, C.; Lococo, S.; Bernardinello, N.; Fichera, G.; Barbiero, G.; Castelli, G.; Cavinato, S.; Ferrari, A.; et al. Clinical Features and Chest Imaging as Predictors of Intensity of Care in Patients with COVID-19. J. Clin. Med. 2020, 9, 2990.
- Wahidi, M.W.; Shojaee, S.; Lamb, C.R.; Ost, D.; Maldonado, F.; Eapen, G.; Caroff, D.A.; Stevens, M.P.; Ouellette, D.R.; Lilly, C.; et al. The Use of Bronchoscopy during the Coronavirus Disease 2019 Pandemic CHEST/AABIP Guideline and Expert Panel Report. Chest 2020, 158, 1268–1281.
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209.
- Batah, S.S.; Fabro, A.T. Pulmonary pathology of ARDS in COVID-19: A pathological review for clinicians. Respir. Med. 2021, 176, 106239.
- Luyt, C.-E.; Sahnoun, T.; Gautier, M.; Vidal, P.; Burrel, S.; de Chambrun, M.P.; Chommeloux, J.; Desnos, C.; Arzoine, J.; Nieszkowska, A.; et al. Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: A retrospective cohort study. Ann. Intensiv. Care 2020, 10, 158.
- Giacobbe, D.R.; Battaglini, D.; Enrile, E.M.; Dentone, C.; Vena, A.; Robba, C.; Ball, L.; Bartoletti, M.; Coloretti, I.; Di Bella, S.; et al. Incidence and prognosis of ventilator-associated pneumonia pneumonia in critically ill patients with COVID-19: A multicenter study. J. Clin. Med. 2021, 10, 555.
- Maes, M.; Higginson, E.; Pereira-Dias, J.; Curran, M.D.; Parmar, S.; Khokhar, F.; Cuchet-Lourenço, D.; Lux, J.; Sharma-Hajela, S.; Ravenhill, B.; et al. Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit. Care 2021, 25, 25.
- Lahmer, T.; Kriescher, S.; Herner, A.; Rothe, K.; Spinner, C.D.; Schneider, J.; Mayer, U.; Neuenhahn, M.; Hoffmann, D.; Geisler, F.; et al. Invasive pulmonary aspergillosis in critically ill patients with severe COVID-19 pneumonia: Results from the prospective AspCOVID-19 study. PLoS ONE 2021, 17, e0238825.
- Lemmers, D.H.L.; Abu Hilal, M.; Bnà, C.; Prezioso, C.; Cavallo, E.; Nencini, N.; Crisci, S.; Fusina, F.; Natalini, G. Pneumomediastinum and subcutaneous emphysema in COVID-19: Barotrauma or lung frailty? ERJ Open Res. 2020, 6, 00385–02020.
- Pandolfi, L.; Fossali, T.; Frangipane, V.; Bozzini, S.; Morosini, M.; D’Amato, M.; Lettieri, S.; Urtis, M.; Di Toro, A.; Saracinoet, L.; et al. Broncho-alveolar inflammation in COVID-19 patients: A correlation with clinical outcome. BMC Pulm. Med. 2020, 20, 301.
- Luo, F.; Darwiche, K.; Singh, S.; Torrego, A.; Steinfort, D.P.; Gasparini, S.; Liu, D.; Zhang, W.; Fernandez-Bussy, S.; Herthet, F.J.F.; et al. Performing Bronchoscopy in Times of the COVID-19 Pandemic: Practice Statement from an International Expert Panel. Respiration 2020, 99, 417–422.