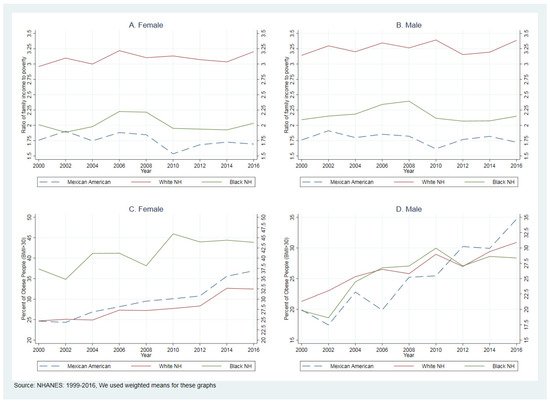
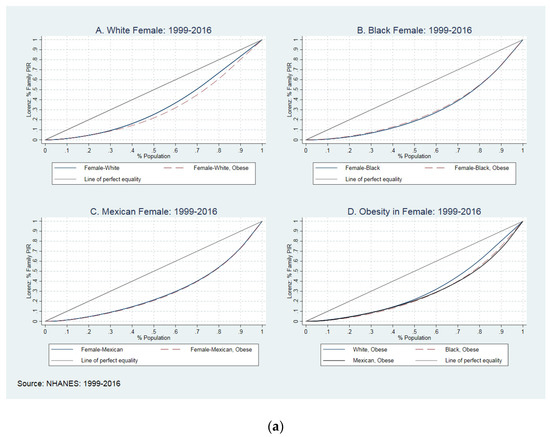
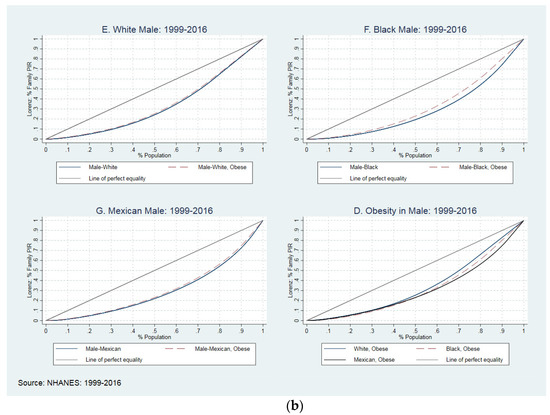
Obesity is a major public health problem both globally and within the U.S. It varies by multiple factors, including but not limited to income and sex. After controlling for potential covariates, there is little evidence to determine the association between income and obesity and how obesity may be moderated by sex and family income. We examined the association between income and obesity in U.S. adults aged 20 years and older, and tested whether this relationship differs by race or ethnicity groups. For this analysis, we used data from the 1999–2016 National Health and Nutrition Examination Surveys (NHANES). Obesity was determined using Body Mass Index ≥ 30 kg/m2; the Gini coefficient (GC) was calculated to measure income inequality using the Poverty Income Ratio (PIR). We categorized the PIR into five quintiles to examine the relationship between income inequality and obesity. For the first set of analyses, we used a modified Poisson regression in a sample of 36,665 adults, with an almost equal number of men and women (women’s ratio was 50.6%), including 17,303 white non-Hispanics (WNH), 7475 black non-Hispanics (BNHs), and 6281 Mexican Americans. The models included age, racial/ethnic groups, marital status, education, health behaviors (smoking and drinking status and physical activities), health insurance coverage, self-reported health, and household structure (live alone and size of household). Adjusting for potential confounders, our findings showed that the association between PIR and obesity was positive and significant more frequently among WNH and BNH in middle and top PIR quintiles than among lower-PIR quintiles; this association was not significant in Mexican Americans (MAs). Results of GC in obese women showed that in comparison with WNHs (GC: 0.34, S.E.: 0.002), BNHs (GC: 0.38, S.E.: 0.004) and MAs (GC: 0.41, S.E.: 0.006) experienced higher income inequality, and that BNH obese men experienced the highest income inequality (GC: 0.45, S.E.: 0.011). The association between PIR and obesity was significant among WNHs and BNHs men in the 3rd, 4th and 5th PIR quintiles. The same association was not found for women. In treating obesity, policymakers should consider not only race/ethnicity and sex, but also strategies to reduce inequality in income.
- income inequality
- obesity
- Gini coefficient
- racial disparities
1. Introduction
Income Distribution and Obesity
2. Analysis on Results
2.1. Association between Income-Level and Obesity
| All n = 36,665 |
White NH n = 17,303 |
Black NH n = 7475 |
Mexican American |
|---|
| All n = 36,665 |
White NH n = 17,303White NH n = 17,303 |
Black NH n = 7475Black NH n = 7475 |
Mexican American n = 6281n = 6281 |
Mexican American |
|
|---|---|---|---|---|---|
| n | = 6281 | ||||
| Mean | Mean | Mean | Gini Coeff. (SE) | Gini Coeff. (SE)Mean | Gini Coeff. (SE)p-Value |
2.4. How Is the Association between Income and Obesity in Men and Women?
| White NH N = 17,303 |
Black NH N = 7475 |
Mexican American N = 6281 |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Gini Coeff. (SE) | Male | p-Value | |||||||||
| Female | Male | Female | |||||||||||
| Obese (%) | 34.9% | 33.7% | 45.5% | 40.0% | |||||||||
| 0.000 | |||||||||||||
| Women | Ratio of family income to poverty (%) | ||||||||||||
| Ratio of family income to poverty (%) (Ref. if PIR < 0.80) | b/se | b/se | b/se | ||||||||||
| Ratio of family income to poverty (%) (Ref. if PIR < 0.80) | PR, 95% CI | PR, 95% CI | PR, 95% CI | PR, 95% CI | PR, 95% CI | PR, 95% CI | |||||||
| Obese | 0.342 (0.002) | 0.301 (0.004) | 0.380 (0.004) | ||||||||||
| 2nd quintile (PIR: 0.81–1.36) | 1.11 | 0.99 | 0.98 | ||||||||||
| 2nd quintile (PIR: 0.81–1.36) | 1.10 | 0.410 (0.006) | 0.000 | 1.01 | 0.96 | 1.02 | 0.97 | 1st quintile (PIR: <0.80) | 9.4 (24.0) | 6.0 (16.0) | 18.0 (44.6) | 20.8 (50.8) | |
| Non-Obese | 0.306 (0.002) | 0.269 (0.003) | 0.392 (0.005) | 0.395 (0.005) | 0.000 | 2nd quintile (PIR: 0.81–1.36) | 12.9 (27.6) | 10.4 (20.5) | 17.1 (43.7) | 24.2 (53.6) | |||
| Men | 0.449 (0.011) | 0.372 (0.15) | 0.000 | ||||||||||
| Non-Obese | 0.298 (0.002) | 0.254 (0.003) | 0.440 (0.004) | 0.416 (0.004) | 0.000 | ||||||||
2.3. The Association between Income and Obesity
| [0.91–1.34] | [0.80–1.21] | [0.84–1.14] | ||||||||||
| 3rd quintile (PIR: 1.37–2.33) | 1.22 * | 1.19 * | 1.05 | 3rd quintile (PIR: 1.37–2.33) | 17.7 (31.5) | Obese | 16.2 (24.8) | 21.9 (47.9) | 23.9 (53.4) | |||
| 0.285 (0.003) | 0.247 (0.004) | |||||||||||
| [1.03–1.45] | [1.00–1.41] | [0.89–1.24] | [0.91–1.14] | [0.86–1.20] | 4th quintile (PIR: 2.34–4.10) | 24.6 (35.5) | 2.6 (29.3) | 23.4 (49.1) | 18.9 (49.0) | |||
| 4th quintile (PIR: 2.34–4.10) | 1.34 *** | |||||||||||
| [0.78–1.05] | 1.30 ** | 1.11 | ||||||||||
| 4th quintile (PIR: 2.34–4.10) | 1.28 ** | 1.01 | 1.23 * | 1.02 | 1.04 | 0.91 | 5th quintile (PIR: 4.11–5.00) | 35.4 (39.4) | 41.8 (33.1) | 19.6 (46.0) | 12.0 (40.7) | |
| [1.15–1.57] | [1.11–1.54] | [0.93–1.33] | Socio-demographic variables | |||||||||
| 5th quintile (PIR: 4.11–5.00) | 1.29 ** | 1.38 *** | 1.01 | |||||||||
| Age in years at screening (mean, SD) | 46.9 (13.8) | 48.6 (11.3) | ||||||||||
| [1.08–1.50] | [0.89–1.15] | [1.03–1.47] | [0.89–1.16] | [0.86–1.26] | [0.73–1.12] | 44.5 (18.4) | 40.1 (18.1) | |||||
| 5th quintile (PIR: 4.11–5.00) | 1.20 * | 0.88 | 1.28 ** | 0.98 | 0.93 | 0.000 | ||||||
| 0.89 | [1.10–1.52] | |||||||||||
| [1.02–1.42] | [0.76–1.01] | [1.08–1.52] | [0.87–1.10] | [0.72–1.20] | Female sex (%) | 50.6% | 50.6% | 53.8% | 44.9% | 0.000 | ||
| [1.18–1.62] | [0.79–1.29] | |||||||||||
| [0.73–1.09] | Socio-demographic variables | |||||||||||
| Socio-demographic variables | Racial/ethnic groups (%) | |||||||||||
| Female | 1.36 ** | 1.83 *** | ||||||||||
| Age | 1.40 *** | 1.00 | 1.00 | 1.00 | 1.00 | White NH | 70.9% | 100.0% | - | - | - | |
| 1.00 | 1.00 ** | [1.13–1.64] | [1.56–2.14] | [1.22–1.61] | Black NH | 10.5% | ||||||
| [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.01] | - | 100.0% | |||||
| Age | 1.00 | 1.00 | 1.00 * | - | ||||||||
| Married | 1.10 | 1.01 | 1.34*** | 1.00 | 1.30*** | 1.03 | Mexican American | 7.6% | - | - | 100.0% | |
| [1.00–1.00] | [1.00–1.00] | [1.00–1.01] | ||||||||||
| [1.00–1.21] | [0.92–1.10] | [1.19–1.52] | [0.93–1.07] | [1.15–1.47] | [0.92–1.14] | Marital status (%) | ||||||
| Married | 1.05 | |||||||||||
| 1.10 ** | 1.13 ** | |||||||||||
| Education (Ref. less than high school) | Married | 64.2% | 67.1% | 44.5% | 68.2% | |||||||
| [0.98–1.12] | 0.000 | |||||||||||
| [1.03–1.17] | [1.05–1.21] | |||||||||||
| High school graduate/GED | 1.15 * | 1.13 * | 1.28 *** | 1.00 | 1.32 *** | 1.14 | Education (%) | |||||
| Education (Ref. less than high school) | ||||||||||||
| [1.01–1.31] | [1.03–1.25] | [1.14–1.43] | [0.91–1.11] | [1.15–1.51] | [1.00–1.30] | Less than high school | 16.7% | 11.4% | ||||
| More than high school | 1.1324.4% | 48.1% | 1.01 | 1.20 * | 1.030.000 | |||||||
| 1.30 *** | High school graduate/GED | 23.7% | 24.5% | 25.1% | 21.0% | 0.432 | ||||||
| 1.20 ** | ||||||||||||
| [0.99–1.28] | [0.91–1.12] | [1.04–1.38] | [0.94–1.12] | [1.13–1.49] | [1.06–1.36] | More than high school | 59.6% | 64.1% | 50.5% | 31.0% | 0.000 | |
| Health system and behaviors | Health system variables (%) | |||||||||||
| Covered by any kind of health insurance | 82.3% | 87.4% | 76.5% | 53.5% | 0.000 | |||||||
| Health behaviors | ||||||||||||
| High school graduate/GED | 1.14 *** | 1.10 ** | 1.24 *** | |||||||||
| [1.06–1.23] | [1.03–1.17] | [1.13–1.36] | ||||||||||
| More than high school | 1.06 | 1.09 * | 1.25 *** | |||||||||
| [0.98–1.15] | ||||||||||||
| Covered by any kind of health insurance | 1.17 * | [1.02–1.17] | [1.13–1.38] | |||||||||
| 1.00 | 1.05 | 1.05 | 1.26 *** | 1.04 | Health system and behaviors | |||||||
| [1.03–1.31] | [0.90–1.11] | [0.93–1.19] | [0.96–1.14] | [1.11–1.44] | [0.93–1.15] | Covered by any kind of health insurance | 1.08 | 1.06 | 1.15 *** | |||
| Smoking status (%) | ||||||||||||
| [1.00–1.18] | [0.99–1.14] | |||||||||||
| [1.06–1.25] | Never | 52.8% | 49.8% | 58.7% | 61.6% | 0.000 | ||||||
| Smoking status (Ref. never smoked) | [0.95–1.12] | [0.92–1.19] | [0.98–1.30] | Former | 25.1% | 28.1% | ||||||
| Current smoker | 15.4% | |||||||||||
| 0.76 *** | 0.79 *** | 0.74 *** | 0.90 * | 0.95 | 1.19 * | [1.03–1.16] | [0.96–1.10] | [0.99–1.19] | ||||
| Current smoker | ||||||||||||
| [0.68–0.85] | [0.71–0.88] | [0.65–0.84] | [0.83–0.98] | 0.78 *** | 0.83 *** | 1.03 | ||||||
| [0.83–1.08] | [1.04–1.37] | |||||||||||
| Drinking status (Ref. never drink) | [0.72–0.84] | [0.77–0.89] | [0.93–1.15] | |||||||||
| Drinking status (Ref. never drink) | ||||||||||||
| Former drinker | 1.34 *** | 1.21 *** | 1.12 | 1.09 | 0.81 | 1.05 | ||||||
| [1.15–1.55] | [1.09–1.34] | [0.92–1.36] | [1.00–1.19] | [0.62–1.07] | [0.92–1.21] | Former drinker | 1.24 *** | 1.10 * | 1.00 | |||
| Current drinker | 1.02 | 0.93 | 1.08 | 1.02 | 0.90 | 0.98 | [1.13–1.36] | [1.01–1.20] | ||||
| [0.88–1.14] | ||||||||||||
| [0.90–1.16] | [0.85–1.02] | [0.92–1.26] | [0.94–1.11] | Current drinker | 0.95 | 1.04 | 0.98 | |||||
| 0.93 | [0.73–1.11] | [0.86–1.11] | ||||||||||
| Physical activities | [0.88–1.03] | [0.96–1.13] | [0.87–1.09] | |||||||||
| No rigorous activities | 1.33 *** | 1.40 *** | 0.99 | 0.96 | 1.20 *** | 1.15 ** | Physical activities | |||||
| No rigorous activities | 1.37 *** | 0.98 | 1.18 *** | |||||||||
| [1.30–1.44] | [0.92–1.04] | [1.11–1.26] | ||||||||||
| Self-reported health: Fair–poor (=1, if fair–poor) | 1.42 *** | 1.38 *** | 1.35 *** | |||||||||
| [1.34–1.51] | [1.31–1.45] | [1.25–1.45] | ||||||||||
| HH structure | ||||||||||||
| Live alone (=1, if alone) | 1.10 | 1.04 | 0.97 | |||||||||
| [0.99–1.22] | [0.95–1.13] | [0.81–1.16] | Household’s size | 1.06 *** | 1.02 | 1.01 | ||||||
| [1.03–1.08] | [1.00–1.04] | [0.98–1.04] |
| [0.90–1.33] | [0.89–1.14] | [0.78–1.19] | [0.92–1.14] | [0.83–1.13] | [0.82–1.07] | ||
| 3rd quintile (PIR: 1.37–2.33) | 1.19 | 1.05 | 1.15 | 1.01 | 1.01 | 0.90 | |
| [1.00–1.41] | [0.92–1.19] | [0.97–1.37] | |||||
| Smoking status (Ref. never smoked) | |||||||
| Former smoker | 1.12 ** | 1.06 | 1.00 | 1.04 | 1.04 | 1.13 | |
| Former smoker | 1.09 ** | 1.03 | |||||
| [1.03–1.21] | 19.9% | ||||||
| [0.97–1.15] | 1.08 | Current | 22.1% | 22.1% | 25.9% | 18.5% | |
| [0.89–1.13] | Drinking status (%) | ||||||
| Never | 12.6% | 10.3% | 18.5% | 15.4% | 0.000 | ||
| Former | 11.5% | 10.2% | 16.6% | 12.3% | |||
| Current | 76.0% | 79.5% | 65.0% | 72.3% | |||
| Physical inactivity (%) | |||||||
| Has no rigorous or moderate activities | 40.5% | 37.6% | 48.6% | 52.6% | 0.000 | ||
| Self-reported health (%) | |||||||
| Fair–poor (=1, if fair–poor) | 16.7% | 13.6% | 23.3% | ||||
| [1.23–1.43] | [1.31–1.50] | [0.89–1.09]31.7% | [0.90–1.03]0.000 | ||||
| [1.09–1.32] | [1.05–1.27] | HH structure (%) | |||||
| Live alone (=1, if alone) | 13.4% | 14.7% | 15.9% | 4.5% | 0.094 | ||
| Total number of people in the household | 5.78 | 5.93 | 4.53 | 6.14 | 0.000 |
2.2. A Gap in Income and Highest Income Inequality in Communities of Color
| Self-reported health: Fair–poor (=1, if fair–poor) | ||||||
| 1.38 *** | ||||||
| 1.46 *** | ||||||
| 1.45 *** | ||||||
| 1.34 *** | ||||||
| 1.29 *** | ||||||
| 1.38 *** | ||||||
| [1.25–1.51] | ||||||
| [1.36–1.58] | [1.31–1.61] | [1.26–1.43] | [1.15–1.45] | [1.27–1.51] | ||
| HH structure | ||||||
| Live alone (=1, if alone) | 1.16 * | 1.05 | 1.26 ** | 0.95 | 1.14 | 0.88 |
| [1.01–1.34] | [0.92–1.20] | [1.06–1.49] | [0.85–1.05] | [0.86–1.50] | [0.72–1.07] | |
| Household’s size | 1.07 *** | 1.04 ** | 1.03 | 1.01 | 1.01 | 1.01 |
| [1.03–1.10] | [1.02–1.07] | [1.00–1.07] | [0.99–1.03] | [0.97–1.05] | [0.97–1.04] |
3. Current Insights
3.1. What Is the Impact of Income Inequality, Racial Composition, and Poverty on Health Outcomes?
3.2. Education and Lifestyle Changes
-
Following healthy dietary patterns at an early life stage.
-
Cutting back foods high in solid fats, added sugars, and salt.
-
Eating the right number of calories, meeting food group needs, and being physically active.
3.3. Nutrition Assessment
References
- Deaton, A. What’s wrong with inequality? Lancet 2013, 381, 363.
- Khullar, D.; Chokshi, D.A. Health, income, & poverty: Where we are & what could help. Health Aff. 2018, 10.
- Zumbrun, J. Is the Gender Pay Gap Closing or Has Progress Stalled? The Wall Street Journal. 2014. Available online: https://www.wsj.com/articles/BL-REB-24473 (accessed on 25 October 2021).
- Stiglitz, J.E. The Price of Inequality: How Today’s Divided Society Endangers our Future; W. W. Norton & Company: New York, NY, USA, 2015.
- National Academies of Sciences, Engineering, and Medicine. Communities in Action: Pathways to Health Equity; The National Academies Press: Washington, DC, USA, 2017.
- Marmot, M.; Wilkinson, R.G. Psychosocial and material pathways in the relation between income and health: A response to Lynch et al. BMJ 2001, 322, 1233–1236.
- Marmot, M. The influence of income on health: Views of an epidemiologist. Health Aff. 2002, 21, 31–46.
- Subramanian, S.V.; Kawachi, I. Income inequality and health: What have we learned so far? Epidemiol. Rev. 2004, 26, 78–91.
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic disparities in health behaviors. Annu. Rev. Sociol. 2010, 36, 349–370.
- Kirby, J.B.; Kaneda, T. Neighborhood socioeconomic disadvantage and access to health care. J. Health Soc. Behav. 2005, 46, 15–31.
- Craig, M.; Hales, M.D.C.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief No. 360 February 2020. U.S. Departmnet of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. 2020. Available online: https://www.cdc.gov/nchs/data/databriefs/db360-h.pdf (accessed on 25 October 2021).
- Syed, I.U. In biomedicine, thin is still in: Obesity surveillance among racialized, (Im) migrant, and female bodies. Societies 2019, 9, 59.
- GWU. Stop Obesity Alliance. Fast Facts: The Cost of Obesity. School of Public Health and Health Services. The George Washington University. 2013. Available online: https://stop.publichealth.gwu.edu/sites/stop.publichealth.gwu.edu/files/documents/Fast%20Facts%20Cost%20of%20Obesity.pdf (accessed on 25 October 2021).
- Trogdon, J.G.; Finkelstein, E.A.; Hylands, T.; Dellea, P.S.; Kamal-Bahl, S. Indirect costs of obesity: A review of the current literature. Obes. Rev. 2008, 9, 489–500.
- Lee, H. Inequality as an explanation for obesity in the United States. Sociol. Compass 2011, 5, 215–232.
- Bell, C.N.; Kerr, J.; Young, J.L. Associations between obesity, obesogenic environments, and structural racism vary by county-level racial composition. Int. J. Environ. Res. Public Health 2019, 16, 861.
- Campbell, A.D.; Baker, E.H. Do income inequalities in higher weight status depend on social integration? Soc. Sci. Res. 2019, 83, 102301.
- Zare, H.; Gaskin, D.D.; Thorpe, R.J. Income Inequality and Obesity among US Adults 1999–2016: Does Sex Matter? Int. J. Environ. Res. Public Health 2021, 18, 7079.
- Matthew, P.; Brodersen, D.M. Income inequality and health outcomes in the United States: An empirical analysis. Soc. Sci. J. 2018, 55, 432–442.
- Pabayo, R.; Fuller, D.; Lee, E.Y.; Horino, M.; Kawachi, I. State-level income inequality and meeting physical activity guidelines; differential associations among US men and women. J. Public Health 2018, 40, 229–236.
- Oksuzyan, A.; Juel, K.; Vaupel, J.W.; Christensen, K. Men: Good health and high mortality. Sex differences in health and aging. Aging Clin. Exp. Res. 2008, 20, 91–102.
- Westenhoefer, J. Age and gender dependent profile of food choice. Diet Diversif. Health Promot. 2005, 57, 44–51.
- Zellner, D.A.; Saito, S.; Gonzalez, J. The effect of stress on men’s food selection. Appetite 2007, 49, 696–699.
- Deaton, A.; Lubotsky, D. Mortality, inequality and race in American cities and states. Soc. Sci. Med. 2003, 56, 1139–1153.
- Haithcoat, T.L.; Avery, E.E.; Bowers, K.A.; Hammer, R.D.; Shyu, C.-R. Income inequality and health: Expanding our understanding of state-level effects by using a geospatial big data approach. Soc. Sci. Comput. Rev. 2019, 39, 543–561.
- Mackenbach, J.P. Income inequality and population health: Evidence favouring a negative correlation between income inequality and life expectancy has disappeared. Br. Med J. Publ. Group 2002, 324, 1.
- Gujarati, D.N. Econometrics by Example; Palgrave Macmillan: New York, NY, USA, 2011; Volume 1.
- Soobader, M.-J.; LeClere, F.B. Aggregation and the measurement of income inequality: Effects on morbidity. Soc. Sci. Med. 1999, 48, 733–744.
- Lovasi, G.S.; Schwartz-Soicher, O.; Quinn, J.W.; Berger, D.K.; Neckerman, K.M.; Jaslow, R.; Lee, K.K.; Rundle, A. Neighborhood safety and green space as predictors of obesity among preschool children from low-income families in New York City. Prev. Med. 2013, 57, 189–193.
- Lochner, K.; Pamuk, E.; Makuc, D.; Kennedy, B.P.; Kawachi, I. State-level income inequality and individual mortality risk: A prospective, multilevel study. Am. J. Public Health 2001, 91, 385.
- Subramanian, S.; Kawachi, I.; Kennedy, B.P. Does the state you live in make a difference? Multilevel analysis of self-rated health in the US. Soc. Sci. Med. 2001, 53, 9–19.
- Muller, A. Education, income inequality, and mortality: A multiple regression analysis. BMJ 2002, 324, 23.
- Deaton, A. Inevitable Inequality? American Association for the Advancement of Science: Washington, DC, USA, 2014.
- Marmot, M. Income inequality, social environment, and inequalities in health. J. Policy Anal. Manag. 2001, 20, 156–159.
- Cooksey-Stowers, K.; Schwartz, M.B.; Brownell, K.D. Food swamps predict obesity rates better than food deserts in the United States. Int. J. Environ. Res. Public Health 2017, 14, 1366.
- Gordon-Larsen, P. Food availability/convenience and obesity. Adv. Nutr. 2014, 5, 809–817.
- Mode, N.A.; Evans, M.K.; Zonderman, A.B. Race, neighborhood economic status, income inequality and mortality. PLoS ONE 2016, 11, e0154535.
- Christafore, D.; Leguizamon, S. Neighbourhood inequality spillover effects of gentrification. Pap. Reg. Sci. 2019, 98, 1469–1484.
- Thorpe Jr, R.J.; Kelley, E.; Bowie, J.V.; Griffith, D.M.; Bruce, M.; LaVeist, T. Explaining racial disparities in obesity among men: Does place matter? Am. J. Men’s Health 2015, 9, 464–472.
- Chen, Z.; Crawford, C.A.G. The role of geographic scale in testing the income inequality hypothesis as an explanation of health disparities. Soc. Sci. Med. 2012, 75, 1022–1031.
- Kim, D.; Wang, F.; Arcan, C. Peer Reviewed: Geographic Association Between Income Inequality and Obesity Among Adults in New York State. Prev. Chronic Dis. 2018, 15, E123. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6198674/. (accessed on 25 October 2021).
- USDA. U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025. 9th Edition. December 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf (accessed on 25 October 2021).
- Harmon, A.H. Community supported agriculture: A conceptual model of health implications. Austin J. Nutr. Food Sci. 2014, 2, 1024.
- Rakel, R. Textbook of Family Medicine 2007; Saunders Elsevier: Philadelphia, PA, USA, 2009.
- Zare, H.; Eisenberg, M.D.; Anderson, G. Comparing the value of community benefit and Tax-Exemption in non-profit hospitals. Health Serv. Res. 2021.
- IRS. Department of the Treasury Internal Revenue Service. 2017 Instructions for Schedule H (Form 990). 2017. Available online: https://www.irs.gov/pub/irs-prior/i990sh--2017.pdf (accessed on 25 October 2021).
- Busch, F. Gender segregation, occupational sorting, and growth of wage disparities between women. Demography 2020, 57, 1063–1088.