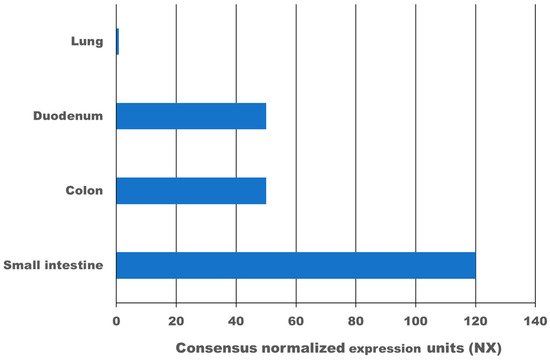
High expression of the transmembrane protein angiotensin I converting enzyme 2 (ACE2), more than 100-times higher as in the lung, and transmembrane serine protease 2 (TMPRSS2) in the gastrointestinal tract leads to infection with SARS-CoV-2. According to meta-analysis data, 9.8–20% of COVID-19 patients experience gastrointestinal symptoms, where diarrhoea is the most frequent, and about 50% shed viruses with high titre through their faeces, where a first faecal transmission was reported. Furthermore, gut inflammation, intestinal damage, and weakening of the gut mucosal integrity that leads to increased permeability has been shown in different studies for COVID-19 patients. This can lead to increased inflammation and bacteraemia. Low mucosal integrity combined with low intestinal damage is a good predictor for disease progression and submission to the intensive care unit (ICU). Several pilot studies have shown that the gut microbiome of COVID-19 patients is changed, microbial richness and diversity were lower, and opportunistic pathogens that can cause bacteraemia were enriched compared to a healthy control group. In a large proportion of these patients, dysbiosis was not resolved at discharge from the hospital and one study showed dysbiosis is still present after 3 months post COVID-19. Consequently, there might be a link between dysbiosis of the gut microbiome in COVID-19 patients and chronic COVID-19 syndrome (CCS). Various clinical trials are investigating the benefit of probiotics for acute COVID-19 patients, the majority of which have not reported results yet. However, two clinical trials have shown that a certain combination of probiotics is beneficial and safe for acute COVID-19 patients. Mortality was 11% for the probiotic treatment group, and 22% for the control group. Furthermore, for the probiotic group, symptoms cleared faster, and an 8-fold decreased risk of developing a respiratory failure was calculated. In conclusion, evidence is arising that inflammation, increased permeability, and microbiome dysbiosis in the gut occur in COVID-19 patients and thus provide new targets for adjuvant treatments of acute and chronic COVID-19. More research in this area is needed.