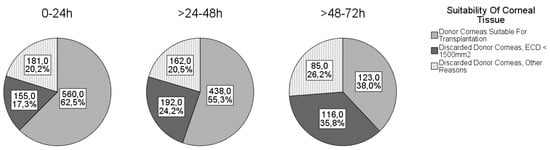
In Germany, more than one-third of donor corneas harvested are not suitable for transplantation. We evaluated the factors associated with the usability of donor corneas. Method: Data from 2032 consecutive donor corneas harvested at the Rhineland-Palatinate Eye Bank in Mainz, Germany, were retrospectively analyzed. Factors of interest were age, sex, lens status, cause of death, cardiopulmonary resuscitation (CPR), death-to-explantation-interval (DEI), and the influence of these factors on the proportion of discarded donor corneas. Factors associated with endothelial cell density (ECD) were analyzed in a linear regression mixed model. Results: Higher donor age, male gender, pseudophakic lens status, and longer DEI were associated with significantly reduced ECD. With respect to DEI, the estimated cell loss was 7 ± 2 cells/mm2/hour (p < 0.001). Age was associated with a lower ECD of 6 ± 2 cells/mm2 per year (p = 0.001). Female ECD was 189 ± 44 cells/mm2 higher than male ECD (p < 0.001). Pseudophakic eyes had 378 ± 42 cells/mm2 less compared with phakic eyes (p < 0.001). Cause of death did not affect the ECD. Of note, 55% and 38% of corneas harvested on the second and third postmortem day, respectively, and 45% of corneas from donors older than 80 years were still suitable for transplantation. In the context of a growing need for donor corneas, we do not recommend limiting donor age and collection time to 24 h or excluding oncology donors, as is the practice in many countries. Therefore, we propose a mathematical model for better donor preselection.
- corneal graft
- donor cornea
- corneal banking
- suitability for transplantation
- death-to-explantation interval
- endothelial cell density
1. Introduction
2. Analysis on Results
2.1. Donors
| Cause of Death/CPR | Male | Female | Total |
|---|---|---|---|
| Cardiovascular/cerebrovascular disease n |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| (%) (n = 837) | 186 (38.2%) | 142 (40.6%) | 328 (39.2%) | |||
| Mean ECD ± SD (cells/mm2) | 1944 ± 622 | 2018 ± 581 | Cancer n (%) (n = 836) | 181 (37.2%) | 113 (32.3%) | 294 (35.2%) |
| Minimum (cells/mm2) | Sepsis n (%) (n = 848) | 71 (14.4%) | 64 (18.1%) | 135 (15.9%) | ||
| CPR n (%) (n = 928) | 24 (4.4%) | 9 (2.3%) | 33 (3.6%) |
| 32 | ||
| 118 | ||
| Maximum (cells/mm2) | 3272 | 3142 |
| Phakic eyes | 799 (68.9%) | 473 (55.6%) |
| Pseudophakic eyes | 352 (30.3%) | 369 (43.4%) |
| Aphakic eyes | 9 (0.8%) | 8 (0.9%) |
2.2. Causes of Disqualification
| Suitable | Discarded | |
|---|---|---|
| No (%) (n = 2032) | 1127 (55.5%) | 905 (44.5%) |
| Gender (n = 2028) | ||
| Corneas from male donors (%) | 622 (53.3%) | 544 (46.7%) |
| Corneas from female donors (%) | 503 (58.4%) | 359 (41.6%) |
| Side (n = 2032) | ||
| Right corneas (%) | 573 (56.3%) | 445 (43.7%) |
| Left corneas (%) | 554 (54.6%) | 460 (45.4%) |
| Lens status (n = 2014) | ||
| Phakic (%) | 812 (63.6%) | 464 (36.4%) |
| Pseudophakic (%) | 302 (41.9%) | 419 (58.1%) |
| Aphakic (%) | 7 (41.2%) | 10 (58.8%) |
| Decade of Life | ECD ± SD (cells/mm2) | n | ||||
|---|---|---|---|---|---|---|
| 95% CI | (cells/mm2) |
p-Value | ||||
| <50 years | 2316 ± 47 | 63 | ||||
| Intercept | 2919 ± 149 | (2626; 3212) | 50–59 years | 2233 ± 49 | 166 | |
| Sex (ref: female) | 60–69 years | 2137 ± 59 | 325 | |||
| 70–79 years | ||||||
| Male | −189 ± 44 | (−275; −102) | <0.001 | 1949 ± 58 | ||
| Age (year) | 541 | |||||
| −6 ± 2 | (−10; −2) | 0.001 | 80–89 years | 1846 ± 63 | 613 | |
| DEI (hour) | −7 ± 2 | (−10; −5) | <0.001 | |||
| Lens status (ref: phakic) | ||||||
| Aphakic | −87 ± 156 | (−393; 218) | 0.574 | |||
| Pseudophakic | −378 ± 42 | (−461; −295) | <0.001 |
| Odds Ratio | 95% CI for Odds Ratio | Regression Coefficient b | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Age | 0.99 | (0.98; 0.99) | −0.01 (−0.02; −0.01) | p = 0.001 | |||
| DEI | 0.98 | (0.97; 0.98) | −0.02 (−0.03; −0.02) | p < 0.001 | |||
| Lens status (pseudophakic) | 0.48 | (0.39; 0.60) | −0.73 (−0.96; −0.52) | p < 0.001 | |||
| Sex (male) | 0.72 | (0.59; 0.89) | −0.32 (−0.52; −0.12) | p | ≥90 years | 1839 ± 59 | 147 |
2.3. Associations
| Parameter | Estimate ECD ± SD (cells/mm2) | |||
|---|---|---|---|---|
| = 0.002 | ||||
| CPR (no) | 0.45 | (0.25; 0.81) | −0.80 (−1.56; −0.25) | p = 0.008 |