Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Marcel F. Kunrath and Version 2 by Ron Wang.
Dental components manufactured with zirconia (ZrO2) represent a significant percentage of the implant-prosthetic market in dentistry. However, during the last few years, we have observed robust clinical and pre-clinical scientific investigations on zirconia both as a prosthetic and an implantable material. Dental devices manufactured from ZrO2 are structurally and chemically stable with biocompatibility levels allowing for safe and long-term function in the oral environment.
- mucointegration
- osseointegration
- zirconia
- biocompatibility
- cell response
1. Introduction
The requirements for biomaterials are for them to be biocompatible coupled with high durability while exposed to the harshness of the oral environment. Additionally, they should not affect or interfere with the recipient’s physiology and general health. Prosthetic components and implants made from zirconia (ZrO2) reveal excellent biological and mechanical properties and superior aesthetic advantages when compared to other biomaterials available on the market [1][2][3][1,2,3]. With the ever increasing body of research conducted around zirconia, clinical use of zirconia implants is on the rise due to their biological, aesthetic and physical properties. [4]. Moreover, it presents itself as an excellent material in the manufacture of customized implants, prosthetic components and various other dental prostheses by means of 3D printing technology [5][6][7][5,6,7].
The challenge with products manufactured with ZrO2 is their hardness and the complexity in the treatment of their surfaces [1][8][1,8]. However, current advanced manufacturing protocols have been able to develop nanoscale textures on this material by applying techniques such as anodizing, high-intensity lasers, acid etching and surface coatings [8][9][10][11][12][8,9,10,11,12]. Gnilitskyi and collaborators reported the use of high-speed femtosecond laser on ZrO2 surfaces for surface nanotexturization, which has been proven to be of significant importance in terms of cell adhesion and osseointegration in an animal model [9]. Thus, the nano-interaction between ZrO2-based surfaces and cells reveals a new and promising path in research which needs more scientific investigation.
Studies on the biological interaction of ZrO2 have become increasingly relevant and are following a path similar to other well proven materials such as titanium and its alloys [13][14][13,14]. Rottmar et al. demonstrated that zirconia surfaces had the best performance with regards to fibrinogen adsorption and thrombogenicity [15]. Furthermore, reports prove zirconia to have an advantage in terms of biological properties with soft peri-implant tissues thereby modulating fibers and cell attachment and behavior with greater effectiveness and biocompatibility [16][17][16,17]. Along with the properties mentioned above, zirconia has a low surface energy [18][19][18,19], therefore it retains very low amounts of plaque and consequently has less bacterial colonization on its surface. In a study, Kunrath et al. showed by comparing surfaces with different morphologies which were exposed to the bacterium Staphylococcus epidermidis that there was less bacterial adhesion on ZrO2 surfaces [18]. Moreover, Roehling et al., revealed a significant reduction in the formation of oral biofilm on zirconia surfaces after 72 hours [19].
2. Zirconia Applications and Variations
With the aim of offering an alternative to metal-based dental prostheses, structural ceramics have been improved and are now widely used in dentistry. Among all dental ceramics, zirconia has emerged as a versatile and promising material due to its biological, mechanical and optical properties which have contributed to its rapid and widespread adoption in dentistry. Zirconia has been a material of choice which, when used with CAD/CAM technology, has allowed the fabrication of various prosthetic components and customized implants for a broad range of treatment options. Zirconia-based ceramics are routinely used for structural applications in engineering such as in the manufacturing of cutting tools, gas sensors, refractories and structural opacifiers [20][24]. The ceramic composites that are currently in use in medical and dental devices originated from structural materials used in the aerospace and military industry. In order to meet structural demands, zirconia is doped with stabilizers to achieve high strength and fracture toughness [21][25]. These materials have been modified to suit the additional requirements of biocompatibility [22][26].3. Surface Modifications Aiming at Improved Biological Responses
3.1. Sand Blasting
Sandblasting, which is also known as airborne particle abrasion, produces a surface topography that has micro-roughness. Various parameters affect the roughness that is created on the implant surface, this includes the size, shape and kinetic energy of the particles used in the sandblasting process [23][31]. During the process of sandblasting, compressed air pressure creates an impulse which ejects the particles toward the surface of the implant. Thus, the kinetic energy which is obtained by the particles depends on their density, volume and velocity. The main advantage of the process of sandblasting is that a homogenous and gentle anisotropic abrasion can be obtained on hard materials like ceramic, glass and silicon. Alumina particles are the generally preferred sandblasting materials because of their low cost, hardness and needle-like shape. The major disadvantage of using the sandblasting technique is that it may slightly change the surface chemistry because of inevitable alumina contamination and in the case of ceramics induce micro-cracks within the implant or the prosthetic part prior to any functional stresses [24][32]. Many studies have proven that although the sandblasted zirconia surfaces show slight enhancement in cell attachment, their metabolic activity is still inferior to that of etched zirconia surfaces [23][25][31,33].
3.2. Acid Etching
The process of acid etching is performed with either hydrofluoric acid, nitric acid or sulfuric acid. Acid etching treatment can also be used to overcome alumina contamination as it has been proven to remove the alumina residues (Table 1). Heat treatment follows thereafter, which helps smoothen the sharp edges made as a result of the etching process [26][34]. Advantages of acid etching include the homogenous roughening of the material, regardless of its size and shape [27][35]. This method presents no risk of delamination and does not exert stress on the material [28][36]. However, it might cause undesirable chemical changes which can be a disadvantage of the process [29][37]. The topography formed after acid etching depends on prior treatment, composition of acid mixture, temperature and the length of exposure to the etchant. Acid etching is generally used to generate a micro scale surface texture which has the ability to achieve interlocking between the implant and the bone [27][35]. Recent studies show that combining the sandblasting and acid etching techniques enhances the degree of micro-roughness of zirconia as well. Such a combination has been proposed and is currently used in some commercially available zirconia implants; the purpose is to optimize micro-roughness, which would also provide a more receptive surface for osteoblast cell attachment and proliferation [26][30][34,38].
Table 1. Summary of the current chemical and physical treatments for zirconia implant surface.
| Zirconia Implants Surface Treatments | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | Procedure | Disadvantages | Characteristics | References | |||||||
| Sandblasting | High pressure alumina (Al | 2 | O | 3) | release | Surface micro-cracks, Structural stress, contaminations | Low cost, hardness and needle-like shape | [23][25] | [31,33] | ||
| Acid etching | Combinations of: (1) ≃48% hydrofluoric acid (HF) (2) ≃70% nitric acid (HNO | 3 | ) (3) ≃98% Sulfuric acid (H | 2 | SO | 4 | ) | Undesired chemical changes | Remove the alumina contamination. Micro scale surface texture for bone to implant contact interface | [27][28][29] | [35,36,37] |
| Selective infiltration technique | Coating and glass heating procedure | Extended only to the surface grains | Nano-porous surface | [31 | |||||||
Figure 4. SEM micrographs demonstrating the different behavior and alignment of human gingival fibroblasts on different ZrO2-modified surfaces developed for implant abutments submitted to three different polishing protocols under a 24-h culture (A–D) and 48-h culture (E–H). The more polished surfaces showed greater cell counts (B–D, F–H) revealing an influence of polishing in the proliferation of this cell at 24 h and 48 h. Letters (a,b,c) represent statistical significance between the groups. Reprinted with permission under Creative Commons Attribution 4.0 International License, reference [80][88].
Table 2. Summary of the current cellular and tissular interactions of the ZrO2 derivates.
| ZrO | 2 | -Derivates Interactions | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cellular and Tissular Response | Tissue | Cells | Effects | References | ||||||||||
| Connective tissue cells | Fibroblasts Macrophages |
-Increased cells migration and proliferation. -Fibronectin and vitronectin release. -Collagen and extracellular matrix proteins release. -Better cellular activity with hydrophilic surfaces. |
[77][78] | 86 | [79][80][81][82] | ,87 | [ | ,88 | 83 | ,89 | ][ | ,90 | 84] | [85,,91,92] |
| Blood cells | Erythrocytes Platelets |
-Fibrinogen cascade activation. -Plasma proteins activation. |
[63][64][65][66] | [71,72,73,74] | ][32] | [39,40] | ||||||||
| Polishing | ||||||||||||||
| Defense cells | Neutrophils, Leukocytes | -Histamine release. -Mast cell degranulation. |
[63][64][65][66][ | |||||||||||
112]. Authors suggested [105][113] that zirconia coating on the surface of titanium implants favors bone apposition more than titanium uncoated implants. The coating provides a favorable interaction between the bone-implant region promoting the development of more mature bone apposition [105][113].
Regarding post-loading osseointegration evaluation, Akagawa et al. [106][114], found that there is no significant difference in clinical features between the loaded and unloaded zirconia implants. However, the bone-implant contact for the unloaded group was 81.9% whereas it was 69.8% for the loaded group (Table 3). Another study that examined the role of osseointegration under various loading conditions around one-stage threaded zirconia implants, showed no difference in bone-implant contact ratio among the single freestanding, connected freestanding and mixed implant-tooth prosthetics using partially stabilized zirconia implants [107][115]. These findings were in agreement with a report that compared the bone-implant contact (BIC) (after 4 weeks of healing) of submerged zirconia implants, non-submerged zirconia implants and submerged titanium as the control [108][116] (Table 3). The results demonstrated the best performance with regards to bone-volume density in submerged zirconia implants (80%), followed by submerged titanium (74%) and non-submerged zirconia (63%) [108][116]. Moreover, no statistical difference was found between the BIC of all three types of implants when zirconia implants were compared to titanium and alumina [109][117]. Based on some studies, it was also suggested that the zirconia implants might withstand occlusal loads over a longer period of time [110][118].
Table 3. Summary of the hard tissues’ response of the ZrO2-based materials.
| Bone Tissue Response to ZrO | 2 | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect | Author | Effectiveness | Reference | |||||||||||||||||
| Implant Loading | Akagawa et al. Stadlinger et al. |
No bone-implant contact (BIC) with significant difference between the loaded and unloaded zirconia implants (BIC loaded: 81.9%; BIC unloaded: 69.8%). No BIC significant difference submerged zirconia and the non-submerged zirconia implants. |
[106][108] | [114,116] | ||||||||||||||||
| Chemical Property | Gahlert et al. Noumbissi et al. Sollazzo et al. |
No difference of bone formation pattern in direct contact with zirconia and surface-modified titanium implant surfaces. Zirconia oxide high resistance to corrosion and ions release. Higher BIC percentage of zirconia implant compared to titanium implant. |
[105][111] | [113 | [112] | ,119,121] | ||||||||||||||
| Silicon carbide polishing paper with diamond or silica suspension | Smoother surface compared to acid etching and sandblasting | Average surface roughness between 8 and 200 nm. No surface chemistry modifications. | 67][68] | ,75 | [69][70][71][72][[ | ,76,77 | 90 | ,78 | 73][74][75][76][77][78] | ,12385 | [79] | ,86 | [80] | ,87 | [81] | ,88 | [82] | ,89 | [83][84][][ | , |
| Surface Treatments | 79 | 91 | ][ | ,80 | 92 | ,90,91 | 85] | ,92,93,94 | ][93] | [71,72,73, | [32][33][34] | [40,41,42] | ||||||||
| 74 | [ | 86 | ,81 | ] | , | Sennerby et al.82 | [ | ,83 | 87][88][89 | ,84 | Sandblasted zirconia implants can achieve a higher stability in bone than machined zirconia implants. | ] | , | [113] | 95,96,97,98,99,100,101] | Laser treatment | ||||
| [ | ] | (1) CO | 2 | laser (2) ER:YAG (3) Cr:YSGG |
Disrupts chemical structure | No surface contamination. Improve material wettability |
Epithelium tissue | Epithelial cells | -Increased differentiation and proliferation. -Faster healing process and protective scarring. |
[ | ||||||||||
| Biocompatibility | Liagre et al. Hisbergues et al. Helmer et al. |
No pseudo-teratogen effect. No evidence of high cytotoxicity or inflammation. No evidence of local bone reaction associated to the alumina treatment. | 85] | [114][86]] | [93 | [87 | ,94 | [115]][116][ | [127,129,132 | 88][89 | ,95,96,97] | [35][36][37] | [43,44,45] | |||||||
| Ultraviolet light treatment (UVC) | ||||||||||||||||||||
| ] | UVC photons | No effects on surface roughness and surface chemistry | Effect of superhydrophilicity | Osteoprogenitors | Osteoblasts | -Increased migration and proliferation. -Increased activity of osteopontin, osteocalcin, BMP-2 genes.-Osteoprogenitors sells adherence and proliferation. |
[69][70][71][72][73][74][75][[38][39][40][41][42][43][44] | [46,47,48,49,50,51,52] | ||||||||||||
| Coating | Obtained by electrophoretic deposition (EPD) and plasma-spraying: (1) Reinforced hydroxyapatite (HA) (2) Calcium Phosphate (Ca(PO) | 4 | ) (3) Bioglaze (RKKP) |
Coating-implant bond strength and modification of chemical structure | Low cost and a high deposition rate. Good biocompatibility, corrosion resistance, and bioactivity | [45][46]50][51][52] | [53 | [47][48][ | ,54 | 49 | ,55 | ] | ,56,57 | [ | ,58,59,60] | |||||
| Biofunctionalization | (1) Immobilized arginine—glycine—aspartate (RGD) | Structural chemical changes | Improved biochemical properties and biological responses | [39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][54][55] | [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63] | |||||||||||||||
| Self-assembly | Self-assembled monolayers of active organic compound and terminal functionalization | Van der Waals layer interactions | Surface vapor deposition of active organic compound and molecule adhesion | [56][57][58][59][60] | [64,65,66,67,68] | |||||||||||||||
3.3. Selective Infiltration Technique
This technique involves coating the surface of the material with a specific infiltration glass and then heating it at a temperature higher than its glass transition temperature. This is followed by the infiltration of molten glass that occurs between the material grains (Table 1). This technique can be used for selective roughening because only the surface grains joined with the infiltration glass are involved in the process, thereby allowing control over the area requiring treatment. Traces of infiltration agent left behind, can further be removed by immersion in a solution of 5% hydrofluoric acid and rinsing with water [31][39]. This selective infiltration etching technique is often used to create a nano-porous surface on zirconia implants [32][40]. The major advantage of this technique is that the actual surface chemistry of material remains unchanged, and the nanoscale roughness of the surface can be enhanced without losing any material or changing the microscopic surface roughness.
3.4. Polishing
Polishing gives a comparatively smoother surface than acid etching and sandblasting (Table 1). It is known that the epithelial cells are more likely to adhere to rough surfaces (acid etching and sandblasting) as compared to smoother polished surfaces, whereas fibroblasts adhere well onto both roughened and smooth surfaces [33][41]. Polishing of a zirconia surface is performed by using a silicon carbide polishing paper and a diamond or silica suspension using a polishing machine [34][42]. Mechanical surface treatment that includes polishing, allows a change in the surface topography without modifying the actual surface chemistry or structural integrity. The average surface roughness of a polished zirconia biomaterial is between 8 and 200 nm [32][34][40,42]. Polishing also serves to clean the implant surface to a certain extent, along with giving it a smooth texture.
3.5. Laser Treatment
In contrast with sandblasting and acid etching techniques, laser treatment exerts zero risk of surface contamination as there is no direct contact between the laser and the biomaterial [35][43]. The laser surface treatments also tend to improve the material wettability by altering the surface properties, which further plays a major role in cell adhesion. The test for wettability is conducted by putting one drop of the liquid on a flat solid surface of the material and the contact angle is further used to represent the final shape of that drop (Table 1). The higher the contact angle, the lower the wettability of the material. The wettability of material also affects the protein adsorption and cellular adhesion [36][44]. Protein adsorption depends completely on the nature of the protein-bearing aqueous solution, and the cells are believed to behave differently in response to different organization of the adsorbed protein layers. It is therefore important that the implant surface wettability be elevated, thereby allowing optimal protein adsorption. However, the use of lasers on zirconia ceramic has been reported to disrupt its chemical structure with the potential of inducing pre-function cracks and partial transformation to the monoclinic phase as a result [36][37][44,45].
3.6. Ultraviolet Light Treatment
Various studies have shown that bone implant contact of the implants treated with ultraviolet (UV) light was deeply enhanced because of the effect of superhydrophilicity (Table 1). A material is described to be superhydrophilic when the contact angle of the water droplet is less than 5° [38][39][46,47]. Hydrophilicity is one of the key factors involved in the initial interaction with proteins and cells that is beneficial for the early phases of wound healing and osseointegration [40][48]. When the hydrophilic oxide surface binds to water, hydroxyl (OH−) and oxygen (O2−) groups are formed on the outermost layer. The formation of hydroxylated oxide surface improves the surface reactivity with the surrounding ions, amino acids and proteins in the tissue fluid. When compared to hydrophobic surfaces, osteoblasts cultured on hydrophilic surfaces have shown to exhibit higher levels of differentiation markers, including alkaline phosphatase and osteocalcin [41][42][49,50]. The effect of hydrophilic surfaces on osseointegration can be observed with improvements in the bone implant contact and bone anchorage that occurs in the early stages of bone healing. Other studies have shown that the atomic percentage of hydrocarbon will change after UV treatment [43][44][51,52].
3.7. Coating
Coating of yttrium stabilized zirconia (YSZ) with reinforced hydroxyapatite (HA) has shown positive results in the enhancement of adhesive strength and coating stability [42][50]. Because of their versatility, calcium phosphate (Ca(PO)4)(CP)-based coatings are generally fabricated using plasma-spraying techniques. Despite its numerous drawbacks, this technique is said to provide low cost and a high deposition rate [45][46][53,54] (Table 1). For depositing CP-based coatings, new techniques are constantly being developed to address the issues associated with plasma spraying. In an in vitro study, Pardun et al. synthesized a YSZ/HA coating by wet powder spraying (WPS) using a double action airbrush spray. Although WPS shows versatility in coating curved surfaces with different thickness, the long-term stability of these coatings has not been confirmed [47][48][55,56].
Because of its simplicity and highly versatile nature, electrophoretic deposition (EPD) has been proposed as an alternative to traditional techniques. An approach that combines both plasma electrolytic oxidation and electrophoretic deposition has been made to fabricate and coat zirconia or hydroxyapatite film on zirconium [49][50][51][57,58,59]. Good biocompatibility, corrosion resistance and bioactivity obtained through this process broadens the potential applications of EPD. Apart from HA, silica is also commonly used as a coating material for zirconia. The use of RKKP has also shown a positive cell response and osseointegration. Coating with RKKP was fabricated using either an enameling and firing technique or thermal treatment. AP40, another silica bioactive glass, was also determined to be comparable in terms of reactivity with RKKP [48][56]. Frandsen et al. sputter coated a commercial zirconia implant with a film of titanium and conducted anodization to produce a coating of TiO2 nanotubes on the surface. Along with the enhanced osteoblast behavior, superhydrophilicity was also observed on the treated implant [52][60].
3.8. Biofunctionalization
Biomimetic surface modification, also called biofunctionalization, involves immobilization of biomolecules on the surface to change their biochemical properties and biological responses [39][47]. Biofunctionalization also allows anchorage of organic components such as proteins, enzymes and peptides on the implant surface thereby determining the type of tissue that develops at the implant-bone interface (Table 1). Arginine-glycine-aspartate (RGD) is commonly used as an adhesive peptide [53][61]. Many other adhesive proteins are found to possess RGD as their cell recognition site, including fibronectin, fibrinogen and collagen. These RGD sequences are identified using at least one of the integrins [54][62]. Adhesion proteins and integrins form a pair to provide cell anchorage, differentiation and growth signal. The RGD peptide has shown to be successfully immobilized with physical-chemical modifications (surface polarization) or applying functionalized coatings on Y-TZP and thereby enhancing the biocompatibility of the material as well as cell attachment to its surface [53][55][61,63]. The existence of biomolecules at the surface of biomaterials simulates the native cellular micro-environment in control of cell behavior. For instance, Arg-Gly-Asp (RGD), a cell-binding order, which originated from the extracellular matrix (ECM) protein like the fibronectin, has been extensively used because it encourages cell adhesion by enabling integrin receptors. RGD-containing peptides improve the connection of numerous cell types on different types of biomaterials [53][55][61,63].
3.9. Self-Assembly
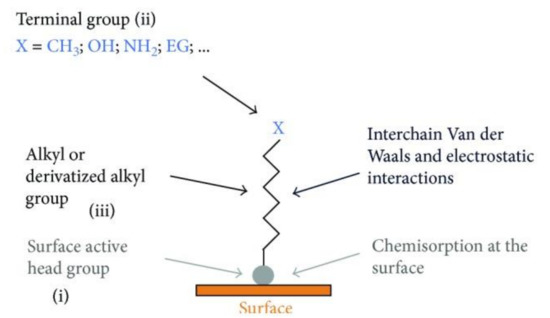
An autonomous process by which the components are organized into patterns or structures without any external intervention is called self-assembly [56][64] (Table 1). Self-assembled monolayers (SAMs) (Figure 2) are formed by the process of solution deposition, i.e., the immersion of a particular substrate into the solution of an active surfactant in a particular solvent which may either be organic or aqueous, or the solid surface vapor deposition of an active organic compound or by aerosol spraying. The driving force for self-assembly is generally the specific interaction between the head group of the surfactant and substrate surface. Most of the surfactants consist of three distinctive parts, namely, the surface active head group which binds strongly to the surface, the terminal group which is located at the monolayer surface shows the interfacial properties of the assembly and the alkane chain which serves as a linker between the head and the terminal groups and facilitates the packing of the molecules in the monolayer with the Van der Waals interactions between adjacent methylene groups that orient and stabilize the monolayer [57][65]. Therefore, by carefully composing the mixture of substrate, SAM solution, and subsequent terminal functionalization, a multitude of subsequent molecule adhesions is feasible [58][59][60][61][66,67,68,69]. In this typical procedure, clean or freshly prepared substrate is absorbed in a diluted 1/10 ml solution of surfactant compound(s) in highly pure solvent for 12–48 h at room temperature. After this, the slides are vacated, cleaned with solvent and dried under a flow of nitrogen [57][59][65,67]. Nanoscale modifications of dental implants have been an active scientific research area, where new techniques such as SAMs are offering approaches to standardize tissue response and microbiota micro environment in accordance with the conditions of bio-activity, anti-adhesion, anti-bacterial or combined effects (Table 1).
4. Biological Responses
The biological responses performed after the placement of a biomaterial in the oral environment are very important for tissues where there is a need for healing [3][12][13][3,12,13]. Surface modifications, functionalization of ZrO2, as well as innovations in the base-material can induce individualized cellular responses promoting a better performance of the device once it is implanted [9][12][17][62][9,12,17,70]. As a result, intraosseous implants, components for implants and oral prostheses made from ZrO2 have attracted the attention of researchers and clinicians due to their biocompatibility properties (Table 2). Materials made from ZrO2 have consistently shown better biological reactions in periodontal and epithelial tissues where most of the cells are fibroblasts, red-blood cells, platelets, defense and epithelial cells [63][64][65][66][67][68][69][70][71][72][73][74][75][76][77][78][79][80][81][82][83][84][85][86][87][88][89][90][91][92][71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100]. In addition, these cells are crucial for the short and long-term success of biomaterials placed in the oral environment although their original task is to protect against contamination from the external environment. Active in vitro/in vivo research is being developed to discover the main ways to modify ZrO2 for better modulation of cells found in soft tissues (Figure 3 and Figure 4).
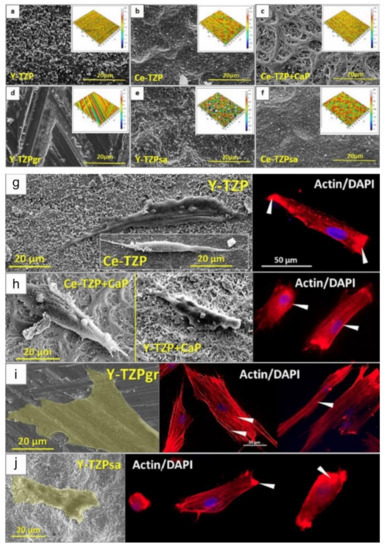
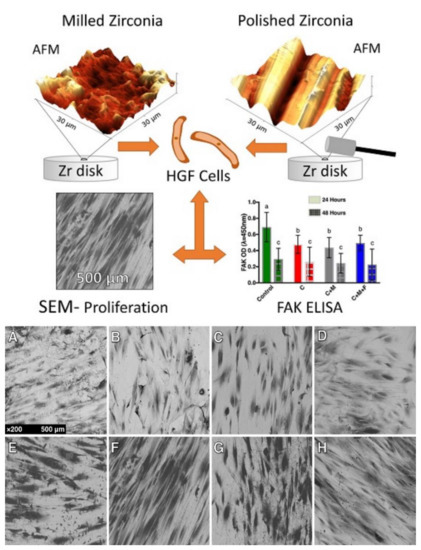
Figure 3. Different ZrO2-surfaces morphologies modified by varied surface treatments (a–f). Microscopies using electron microscopy (SEM) and confocal microscopy showing the different responses of osteoprogenitor cells regarding morphology and nuclei position on four different ZrO2-modified surfaces. The cells presented an elongated morphology in some surfaces (g,h) and a flattened morphology in other topographies (i,j). Showing, as reported in the study, that surface morphology characteristics in zirconia are more important for cell evolution and consequent proliferation than properties such as roughness and wettability. Reprinted and adapted with permission under Creative Commons Attribution 4.0 International License, reference [76][84].
| 76 | ||||||||||||
| ] | ||||||||||||
| [ | ||||||||||||
| 77 | ||||||||||||
| , | ||||||||||||
| 78 | ||||||||||||
| , | 79 | , | 80,81,82,83,84] | |||||||||
| Oral biofilms cells | Bacteria cells | -Lower bacterial adhesion and proliferation. -Reduced bacteria activity. |
[94][95][96][97][98]102] | [102,103,104,105 | [99][100][ | ,106 | 101 | ,107 | ] | ,108,109 | [ | ,110] |
5. Clinical Benefits
5.1. Osseointegration of Zirconia Implants
Osseointegration is one of the most important criteria for the success of an implant treatment. Bone apposition that takes place on different types of implant surfaces depends on the surface properties of the implant [103][104][111,
5.2. Clinical Stability of Zirconia Implants
There are generally two types of modalities to assess osseointegration of dental implants. There are destructive methods such as the pull-push technique and reverse torque and on the other hand there are non-destructive modalities such as resonance frequency analysis (RFA) and the Periotest. It should be noted that none of those techniques and modalities measure osseointegration per se, they rather assess implant stability. The Periotest assesses stability by measuring the amount of micromovement of the implant and the RFA measures the frequency returning from an implant. In both cases, values are given to the measurements and correspond to a certain level of implant stability. Torque removal forces are used as a biomechanical measure for anchorage or osseointegration in which the greater forces required to remove implants may be portrayed as an increase in the strength of osseointegration [117][122] (Table 3).