Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Jerzy Gebicki and Version 2 by Sirius Huang.
Arterial blood pressure monitoring plays an important role in preventive medicine, allowing, in selected cases, the identification of vascular dysfunction. Extensive research, encompassing both healthy subjects and patients with a range of vascular issues, has consistently demonstrated the efficacy of the Flow Mediated Skin Fluorescence (FMSF) technique in identifying cases of impaired vascular function, including many cases of silent vascular dysfunction that are not manifested by changes in blood pressure.
- FMSF technique
- NADH fluorescence
- vascular circulation
- vascular screening
1. Introduction
The diagnosis and treatment of vascular diseases incurs tremendous costs to the healthcare system. Early diagnosis of vascular dysfunction is not always possible, as it is often not manifested by characteristic symptoms. Hypertension is a common example of such silent vascular dysfunction. Therefore, occasional monitoring of arterial blood pressure is recommended as a preventative measure. However, blood pressure monitoring is only able to identify selected cases of vascular dysfunction. Many other cases of silent vascular dysfunction are not manifested by changes in blood pressure.
Vascular system dysfunction often results in insufficient delivery of oxygen and nutrients to tissues, due to hypoxia. There are techniques available for the assessment of the body’s reaction to hypoxia. The classical technique, called flow-mediated dilation (FMD) and regarded as the gold standard [1][2][3][1,2,3], is based on stimulation of the vascular circulation in response to the post-occlusive reactive hyperemia (PORH) [4]. However, FMD only measures the reaction of the macrocirculation to transient hypoxia. Despite great research interest in the use of the FMD technique, its widespread adoption as a routine diagnostic technique has been hindered by the technical complexities involved in its execution.
Changes in the functioning of the endothelium of large blood vessels are often preceded by dysfunction of vascular microcirculation [5]. Because cutaneous microcirculation is representative for the assessment of systemic microcirculation, its dysfunctions and pathologies [6][7][8][6,7,8] and is readily accessible for monitoring, changes in epidermal cell functioning in response to ischemia are a sensitive marker of early vascular circulation disorders.
In light of this, there is growing demand for a diagnostic tool that is both simple and non-invasive, for assessment of the body’s reaction to transient hypoxia. Addressing this need is the Flow Mediated Skin Fluorescence (FMSF) technique [9][10][11][12][13][14][15][16][17][9,10,11,12,13,14,15,16,17]. The FMSF technique stands out for its ability to provide information on distinguishable macro- and microcirculatory responses to transient hypoxia.
The FMSF technique is based on the measurement of the strongest fluorescence emitted from human skin, nicotinamide adenine dinucleotide (NADH) fluorescence. A significant part of the exciting light is absorbed by the epidermis and papillary dermis [11][18][19][20][11,18,19,20]; hence, the emission of NADH and its changes are related to changes in the mitochondrial redox balance of the NADH/NAD+ pair in epidermal cells, which are the final recipients of oxygen from the circulatory system.
NADH fluorescence has previously been used to determine mitochondrial function in vivo [21][22][23][24][21,22,23,24]. Because only the reduced form of the NADH/NAD+ pair fluoresces, limited information can be obtained regarding the redox balance of this coenzyme as an indicator of mitochondrial function. However, the reduced form of the coenzyme (NADH) accumulates under ischemia and hypoxia, while it is oxidized during hyperemia. Hence, changes observed during the PORH test can be used to assess the NADH/NAD+ balance in epidermal cells and vascular response to ischemic conditions.
2. Brief Description of the FMSF Methodology
The Flow Mediated Skin Fluorescence (FMSF) technique measures changes in the in-tensity of nicotinamide adenine dinucleotide (NADH) fluorescence from the skin on the forearm (Figure 1). The changes are stimulated by blocking and releasing blood flow in the brachial artery. The skin is characterized by a specific metabolism. The epidermal layer of skin is not directly vascularized, and oxygen and nutrients are transported from the dermis by diffusion. Therefore, epidermal cell metabolism can be considered a unique and sensitive marker of early dysfunction in vascular circulation and metabolic regulation.
Figure 1.
Operating principle of AngioExpert.
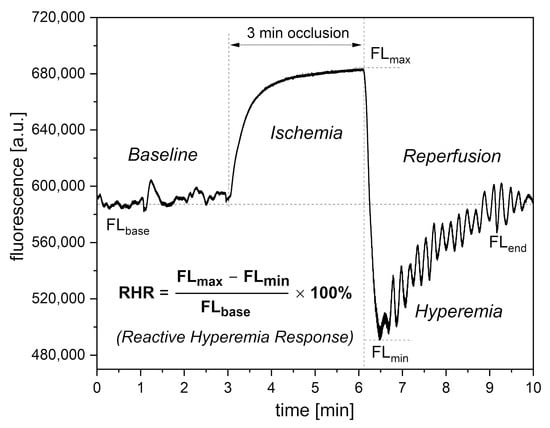
Figure 2.
Definition of the RHR parameter.
3. Interpretation of Key FMSF Parameters for Vascular Screening
Of the three parameters selected for vascular screening, the RHR and HS parameters are particularly useful. The RHR parameter is defined in Figure 2. RHR is a unique parameter based on the combined responses from both the ischemic and hyperemic parts of the measured FMSF trace (RHR = IRmax + HRmax). It represents the overall function of the vascular system, including both macro- and microcirculation [14][17][14,17]. The HS parameter represents a direct measure of the intensity of microcirculatory oscillations related to myogenic oscillations with frequencies in the range of 0.052–0.15 Hz, recorded during reperfusion [13][14][17][13,14,17]. Myogenic microcirculatory oscillations are a very sensitive measure of the microcirculatory response to hypoxia and can be monitored with high precision using the FMSF technique. As the values of the HS parameter can vary within a quite broad range, it is more practical to use a normally distributed log (HS). The baseline microcirculatory oscillations hold interesting diagnostic potential. The intensity and relative distribution of these oscillations in the low frequency range (<0.15 Hz) have been found to be sensitive to various stress factors. These include emotional stress, physical exhaustion, post-infection states, and hormonal deficiencies. The NOI parameter can be used for universal characterization of stress of various origins. The NOI parameter represents the contribution of endothelial and neurogenic oscillations relative to all oscillations detected at low-frequency intervals (<0.15 Hz). For emotional stress, physical exhaustion, or post-infection stress, the NOI parameters have values below 60%. In the case of hormonal deficiency frequently associated with erectile dysfunction, the NOI parameter values are in the range of 90–100% [15][17][15,17]. Based on extensive experience, the function of the RHR, HS, and NOI parameters can be presented in the form of a colored strip, as shown in Figure 3. The most optimal values are shown in green and values indicating potential vascular dysfunction are shown in yellow.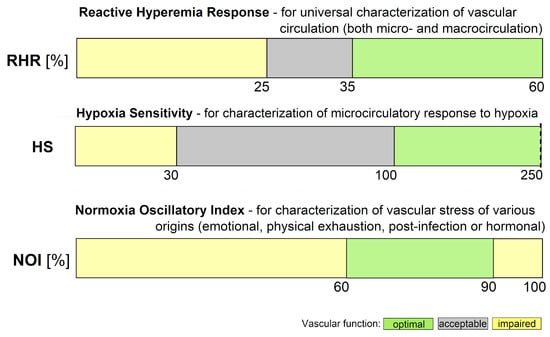
Figure 3. Ranges of key FMSF parameters (RHR—Reactive Hyperemia Response, HS—Hypoxia Sensitivity, NOI—Normoxia Oscillatory Index).