The issue becomes even more debated when it is extended to individuals with liver disease in whom another pathogenic cause (viral, metabolic, or other) is already present. Since the diagnosis of alcohol-related liver disease is based on evidence of clinical and biochemical abnormalities in association with alcohol consumption exceeding certain limits (set at thirty grams per day for males and twenty grams per day for females), it should be evaluated if the assumption of drinks in a quantity below these thresholds could have detrimental consequences in this category of patients.
2. Drinking Quantification
It is very problematic to make an accurate assessment of the amount of drinks consumed by an individual. This is mainly due to a major self-report bias, partly caused by the difficulty of obtaining true information on the grams of alcohol contained in different types of drinks, with a coexisting lack of reliability in reporting the amount of each of the various types of drinks taken by patients. To overcome this limitation, it is reasonable to avoid estimating exact grams while it is more useful to quantify the number of standard drinks taken. In the many national and international guidelines, the definition of alcoholic unit (or standard drink) is not in agreement, with values ranging from eight to sixteen grams. The most accepted measure is that proposed by the World Health Organization (WHO), which has established this amount as ten grams of pure alcohol, corresponding approximately to a half glass of wine (125 milliliters with an alcohol content of 12°), a can of beer (330 milliliters at 4.5°) or a glass of hard liquor (40 milliliters at 36°)
[14].
Drinking habits can be assessed through interviews, quantity frequency diaries, or questionnaires. A viable alternative to these methods is the use of screening instruments routinely employed to identify alcohol use disorder. The most widely adopted instrument is the Alcohol Use Disorders Inventory Test (AUDIT), which consists of ten questions, the first of which is the Alcohol Use Assessment Test
[15].
3. NAFLD
Non-alcoholic fatty liver disease (NAFLD) is a widespread condition, with a worldwide estimated prevalence ranging from 6 to 35 percent. NAFLD is nowadays the most common cause of liver disease in Western industrialized countries, due to the broad diffusion of metabolic risk factors like diabetes mellitus, arterial hypertension, dyslipidemia, and obesity
[16][17][18][19][20][16,17,18,19,20]. The spectrum of NAFLD varies from simple hepatic steatosis to non-alcoholic steatohepatitis (NASH), in which there is a coexistence of fat accumulation, lobular inflammation, ballooning of the hepatocytes, and fibrosis, to liver cirrhosis
[21][22][23][21,22,23].
Even if there are no guidelines or evidence in favor of or against the consumption of a modest amount of alcohol in these patients, in clinical practice, a total abstention from drinking is often recommended.
It should be noted that several studies indicated cardiovascular disease as one of the main causes of mortality in patients with NAFLD
[24] and that the use of a moderate quantity of alcoholic beverages has a beneficial effect in decreasing unfavorable cardiovascular outcomes in the general population
[25]. Following these considerations, the discussion about this controversial issue is as current as ever, and many observational studies have been carried out. The main characteristics of the analyzed studies are summarized in
Table 1.
Sookoian et al. performed a meta-analysis including 43,175 individuals, which showed a protective effect of minimal alcohol consumption against NAFLD, more evident in women than in men, and against the development of advanced disease
[26].
Table 1.
Studies on NAFLD patients.
A large cohort study conducted in Korea, involving more than 58,000 individuals with fatty liver disease in abdominal ultrasounds and an estimated low probability of fibrosis according to non-invasive markers (FIB-4, NFS, and APRI)
[27], demonstrated a correlation between light (1–10 g/day) or moderate alcohol consumption (10–30 g/day in males, 10–20 g/day in females) and the progression to intermediate or high fibrosis. When the latter of these two outcomes was used as the unique endpoint, the aforementioned association was even stronger. To exclude the possible effect of binge drinking, a subgroup analysis on patients who did not consume 60 or more g of alcohol on a single occasion was performed, confirming an increased risk of fibrosis progression in moderate drinkers. An important limitation of this work was the composition of the sample, predominantly consisting of young middle-aged individuals, which makes it difficult to generalize the results to the overall population.
Another large cohort, including nearly ten thousand patients with an echographic diagnosis of steatosis, was analyzed in Japan. The aim was to evaluate the effect of drinking on the incidence of hepatocellular carcinoma (HCC)
[28]. The population was stratified according to the daily amount of alcohol intake, and a higher incidence of HCC at increasing levels of ethanol consumption was observed. In the multivariate analysis, drinking 40 or more g/day of alcohol was reported as an independent risk factor for carcinogenesis. These results have to be cautiously interpreted because of the imbalance between sex categories in the cohort, with a large prevalence of men; another limit is the lack of a comparison with the incidence of HCC in the general population.
A similar study included 5297 subjects who underwent an ultrasound examination of the liver during a systemic health check-up conducted in Japan
[29]. Participants were categorized according to the weekly quantity of ethanol assumed and divided into four groups (0–1–69.9, 70–139.9, 140–279.9, and more than 280 g/week). The results showed an inverse relationship between each category and fatty liver in males, whereas in women, only an intake below the threshold of 70 g per week appeared to be protective against steatosis. Drinking frequency was also evaluated: in men, an inverse association with NAFLD irrespective of the number of days of alcohol consumption was seen; drinking on 4 to 6 days per week and on a daily basis inversely correlated with fatty liver in women. The main limitation of this work is the composition of the sample, which consisted of healthy individuals, thereby making these results impossible to apply to the general population.
Aberg et al. analyzed a cohort of more than eight thousand individuals with NAFLD, using the fatty liver index (FLI) as a diagnostic criterion. The endpoints were fatal and non-fatal liver-related events (requiring hospital admission or causing liver cancer or death), cardiovascular events, cancer, and all-cause death
[30]. An alcohol intake above 9 g per day had a statistically significant association with adverse liver outcomes. An increased risk for the onset of cancer was observed in people consuming more than 30 g of ethanol per day. An alcohol intake of up to 49 g/day was associated with a reduced risk for incident cardiovascular adverse events, and a J-shaped correlation with all-cause death was found, with a maximal risk reduction of 21% in the low-consumption category (from 0 to 9 g per day); reaching an intake above 30 g/day, the risk of death tended to increase proportionally to the rising quantity of alcohol consumed. In the subgroup of patients who consumed less than 24 g per day of ethanol, the largest risk reduction for cardiovascular death and mortality of all causes was seen in preferential wine drinkers. In addition, whereas consumption of non-wine alcoholic beverages up to 24 g/day raised the risk for liver events, low preferential wine drinking exhibited nonsignificant risk estimates for liver disease.
A study on a cohort obtained from the National Health and Nutrition Examination Survey (NHANES, a nationwide survey of the American population) was performed. The sample consisted of 4568 individuals affected by NAFLD (diagnosed with HSI score)
[31]. Modest alcohol consumption, defined as an intake of a minimum of half a drink to less than one and a half drinks per day, was associated with a significantly lower risk of death; conversely, drinking a higher amount of alcohol showed a trend toward increased mortality. A separate evaluation according to the sex category was carried out, with evidence of a more relevant beneficial effect of modest alcohol consumption in women rather than in men. Among older patients (people above 64 years), drinking more than a modest quantity of ethanol did not show a harmful effect on mortality. The population was also stratified according to FIB-4 score values: in subjects at high risk of fibrosis, no beneficial effect of modest drinking was observed. Even excluding deaths from cardiovascular causes, the aforementioned protective effect remained; similarly, the deleterious effect of drinking more than one and a half drinks per day was confirmed.
Another study was based on the NHANES database, comprising more than 4000 individuals with evidence of steatosis in abdominal ultrasounds
[32]. Only excessive alcohol consumption (higher than 3 drinks/day for men) was independently associated with an increased overall mortality. Analyzing the specific causes of death, only mortality by cancer was found to be correlated with excessive alcohol intake; in patients affected by metabolic syndrome, there was also an association with fatal cardiovascular outcomes. Regarding the consumption pattern, it was seen that binge drinking (defined as having 5 or more alcoholic drinks on a single occasion) for at least 13 days a year implied a significant rise in the risk of death, which becomes even higher in the case of binge drinking for more than 20 days per year.
Akahane et al. analyzed a cohort of 2429 males with an ultrasound diagnosis of fatty liver during an annual health check-up
[33]. The prevalence of NAFLD was shown to be the lowest in the moderate-drinking group (alcohol intake of 30–60 g/day) and the highest in the abstainers. Chronic alcohol consumption was independently and inversely associated with liver steatosis, with a greater beneficial effect seen in light drinkers (defined as people who consumed less than 30 g/day of alcohol). The absence of women also makes it difficult to generalize these results in this case.
A small study including 151 diabetic patients with NAFLD (diagnosed according to the presence of steatosis detected with ultrasound), with a non-invasive evaluation of liver stiffness made by transient elastography, reported no significant protective effect of light or moderate alcohol consumption
[34].
4. Chronic Viral Hepatitis
Chronic hepatitis C virus (HCV) and hepatitis B virus (HBV) infections are a global health problem, affecting millions of people worldwide, with important morbidity and mortality
[35][36][37][38][39][49,50,51,52,53].
HCV infection has a higher prevalence in patients with alcohol use disorder (AUD); in particular, a 30-fold higher prevalence has been estimated compared with the general population
[40][41][54,55]. No similar evidence was found regarding the prevalence of HBV infection in alcohol users.
It has been widely demonstrated that alcohol abuse contributes to accelerate the progression of chronic HCV and HBV hepatitis
[42][43][56,57], promoting worsening fibrosis, cirrhosis, and hepatocellular carcinoma
[44][58].
The interactions between alcohol and hepatitis viruses in causing liver damage are complex, and the biological mechanisms involved have not yet been clearly defined
[45][59].
Hepatitis B virus (HBV) infection leads to massive liver damage with progression, if untreated, to cirrhosis in 15–40% of patients, and consequently to liver failure and cancer
[46][60].
Alcohol consumption accelerates liver injury in patients with chronic HBV infection, leading to an increase in fatty changes and fibrosis progression
[47][61]. A study, performed in vivo
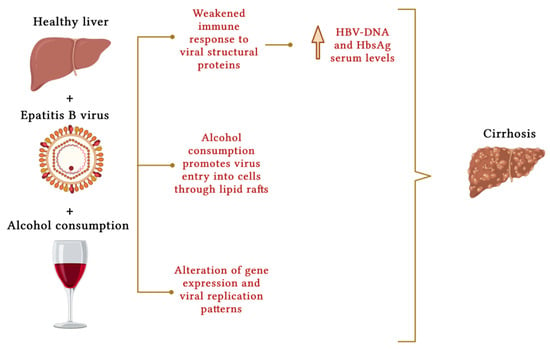
[48][62], that analyzed the trend of fibrosis markers in immunologically compromised mice (SCID), thus in the absence of an immune response against viral proteins, fed an isocaloric diet with ethanol component for 5 weeks. An approximately 7-fold increase in HBV DNA load was found in this population compared with the control group. An increase in hepatitis B surface antigen (HBsAg) levels was also found. Mice with HBV fed with an alcohol-enriched diet showed significantly worsening of liver steatosis. Thus, the study found that chronic alcohol consumption alters, in vivo, gene expression and viral replication patterns, even in the absence of an immune response against the virus.
The mechanisms by which alcohol catalyzes liver damage in patients with chronic hepatitis B are still being investigated; however, several studies attempted to explain the molecular mechanisms underlying liver damage in these individuals.
Among the mechanisms investigated, interference with the immune system seems to impact the pathogenesis. Indeed, alcohol has been shown to impair a proper immune response to HBV, promoting its replication and liver inflammation. Specifically, studies have shown that excessive alcohol consumption can elevate HBV DNA serum levels by weakening the immune response to viral structural proteins
[49][63] (
Figure 1). In addition to the direct effect of alcohol on viral replication, it also appears to have an indirect role in the life cycle of the virus and its entry into cells via lipid rafts
[50][64], which play an important role in molecular signaling mechanisms. Cell membranes have receptors that act as entry points for viruses, allowing them to enter hepatocytes. They are greatly affected by the surrounding microenvironment, which in turn is influenced by alcohol consumption, particularly by the production of acetaldehyde
[51][65].
Figure 1. Molecular mechanisms that represent the contribution of alcohol consumption to the development of liver cirrhosis in chronic HBV infection. Alcohol consumption impairs the immune response to viral proteins and alters viral gene expression, promoting virus replication (with increased serum levels of HBV DNA and HBsAg). Alcohol consumption seems to promote viral entry into hepatocytes through lipid rafts. Created with
BioRender.com.
The pathophysiological mechanism by which alcohol consumption and hepatitis C infection synergistically accelerate the progression of liver fibrosis and liver damage also remains unclear
[52][66]. Several hypotheses have been investigated (
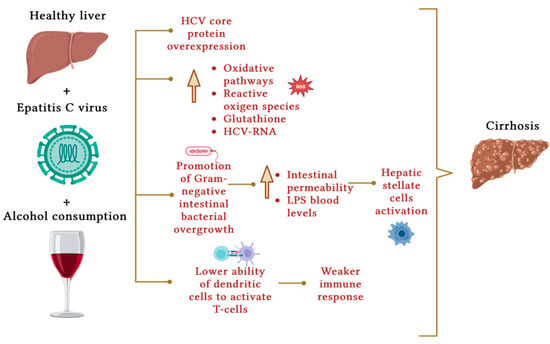
Figure 2). Otani et al.
[53][67] believe that the combined detrimental effect resulting from the action of alcohol and chronic hepatitis C acts via HCV core protein overexpression, with the enhancement of oxidative pathways and reactive oxygen species. Chronic HCV infection has been shown to cause glutathione depletion and consequently oxidative stress
[54][68].
Figure 2. Molecular mechanisms that represent the contribution of alcohol consumption to the development of liver cirrhosis in chronic HCV infection. The overexpression of HCV core protein, the activation of oxidative pathways, and the depletion of molecules with antioxidant activity such as glutathione favoring the production of reactive oxygen species have been recognized as cofactors involved. Ethanol also alters intestinal permeability, leading to an increase in blood levels of lipopolysaccharide secondary to the growth of Gram-negative intestinal bacteria and liver fibrosis due to the activation of hepatic stellate cells. Finally, alcohol weakens the immune response as T cells are activated with greater difficulty by dendritic cells. Created with
BioRender.com.
Alcohol consumption promotes the growth of certain Gram-negative intestinal bacteria, increasing intestinal permeability and thus blood levels of lipopolysaccharide
[55][69], activating hepatic stellate cells, which promote fibrosis
[56][70]. Among the mechanisms involved, in patients with chronic HCV infection, dendritic cells have been shown to have a lower ability to activate T cells, consequently prompting a weaker immune response
[57][71].
Some studies suggest that, in addition to the inhibitory effects on the immune system, alcohol consumption is also involved in the activation of inflammatory pathways and cytokines that mediate inflammation; this accelerates the progression of liver disease
[58][72], demonstrating that even in individuals with chronic hepatitis C who consume moderate amounts of alcohol (<50 g/day), inflammatory markers are increased compared to controls, suggesting an important role of oxidative stress.
The impact of modest alcohol consumption on increasing serum HCV RNA levels has also been demonstrated
[59][73].
5. Hemochromatosis
A toxic additive effect has been hypothesized in subjects with hemochromatosis in the case of concurrent alcohol consumption, partly because iron accumulation in the liver has often been observed in alcoholics, with a mechanism not yet fully understood
[60][61][97,98].
Fletcher et al. estimated an approximately 6-fold increased risk of developing liver cirrhosis in individuals with hemochromatosis consuming more than 60 g/day of alcohol
[62][99].
An in vivo study, which produced conflicting results, was conducted on 59 mice
[63][100] and reported a lower bioavailability of vitamins (especially vitamin E) in all animals exposed to an iron-containing diet and alcohol consumption (at doses of 2%, 5%, and 8%). A significant increase in lipid peroxidation activity was found in all animals consuming alcohol, an iron-rich diet, or both. Blood levels of transaminases showed a greater increase in the case of an iron diet alone when compared to mice fed with ethanol and an iron diet.
The study found that ethanol exposure in iron-overloaded animals positively modulated oxidative stress and organ damage, and this finding was also confirmed by liver biopsy. Notably, in animals fed an iron-rich diet with ethanol in addition, the reduction in vitamin C levels appeared to be much less pronounced when compared to the group only fed an iron-rich diet, which would suggest an antioxidant effect of ethanol in the case of iron overload, despite the reduction in antioxidant vitamins.
Studies on moderate alcohol consumption in hemochromatosis are therefore still lacking.