Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Argen Mamazhakypov and Version 2 by Lindsay Dong.
In response to various stressors, cardiac chambers undergo structural remodeling. Long-term exposure of the right ventricle (RV) to pressure or volume overload leads to its maladaptive remodeling, associated with RV failure and increased mortality. While left ventricular adverse remodeling is well understood and therapeutic options are available or emerging, RV remodeling remains underexplored, and no specific therapies are currently available.
- mast cells
- right ventricle
- cardiac remodeling
1. Introduction
Cardiac remodeling refers to changes in size, mass, geometry, and function of heart, that develop in the course of various cardiovascular pathologies. It initially represents an adaptive process of the heart in response to mechanical, neurohumoral, or other stressors, with the primary aim of preserving cardiac function [1]. However, sustained exposure to pathological factors triggers the development of maladaptive cardiac remodeling. Cardiac remodeling can affect either the left or right ventricle (RV) or both ventricles and is associated with unfavorable outcomes and treatment responses [1][2][1,2]. It is now recognized as an important aspect of cardiovascular disease progression and is emerging as a therapeutic target in heart failure therapy [1].
Currently approved therapies have been efficient in reducing mortality and morbidity of left-heart failure patients [3][4][5][3,4,5]. Both pharmacological and non-pharmacological therapies beneficially impacted prognosis in heart failure patients by modulating the cardiac remodeling process [5][6][7][5,6,7]. Modulation of the renin-angiotensin-aldosterone (RAAS) and sympathetic nervous system is the cornerstone of pharmacotherapy of left heart failure [8]. Increased activity of the sympathetic nervous and RAAS has also been implicated in the pathophysiology for pressure overload-related RV failure [9][10][11][9,10,11]. Consequently, angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, and β-blockers have demonstrated efficacy in reversing RV, remodeling in animal models [9][10][9,10]. However, currently, they are not recommended for therapy of RV failure associated with pulmonary hypertension due to inconsistent results in clinical trials [12]. It is important to note that most of the previous trials were small, underpowered, enrolled patients with systemic RV or predominantly focused on the pulmonary vasculature and did not assess RV remodeling [13][14][13,14]. In addition, the differences between the RV and left ventricle might account for the dissimilar responses of the failing ventricles to inhibitors of neurohormonal activity [15][16][15,16]. However, despite advances in treatment, the burden of heart failure remains high, emphasizing the ongoing need for further research and the development of novel management strategies [3].
Cardiac remodeling develops in response to stressors such as volume or pressure overload. Such unfavorable hemodynamic conditions occur in a variety of diseases, including hypertension, valvular pathologies, chronic pulmonary diseases, obesity, and metabolic disorders. To counteract the sustained rise in wall stress caused by excessive pressure and/or volume load, the myocardium undergoes phenotypic and functional transformations, which encompass a sequence of molecular, cellular, and interstitial alterations. Cardiomyocytes become enlarged due to new contractile protein synthesis, contributing to the increased size and mass of the affected cardiac chamber [17][18][17,18]. In addition to cardiomyocyte changes, cardiac remodeling involves alterations in other cell types and extracellular matrix organization. Fibroblast activation and proliferation result in the amplified synthesis of extracellular matrix proteins [19]. Changes in coronary microvascular endothelial cells lead to alterations in the coronary microvasculature and blood supply to the heart [20]. One of the important features of cardiac remodeling is the recruitment and accumulation of diverse inflammatory and immune cells within the myocardium [21][22][21,22], which can mediate both protective and deleterious effects [21].
2. Right Ventricular Remodeling
Recent studies have provided strong evidence to recognize the pivotal role of the RV in cardiovascular pathologies [23]. Functional and structural changes of the RV define the prognosis in patients with various cardiovascular diseases, including congenital heart disease [24], pulmonary arterial hypertension [25], myocardial infarction [26], advanced left heart failure [27] and stable coronary artery disease [28]. The recognition of the RV as a critical player in the progression of cardiovascular and respiratory conditions has sparked increased research attention towards the RV in recent years [29][30][31][29,30,31]. Pressure overload is a key pathogenetic factor for RV remodeling and dysfunction, which is associated with the release and subsequent accumulation of a myriad of bioactive molecules in the circulation and within the cardiac tissue [32][33][32,33]. These bioactive molecules have the potential to directly impose deleterious effects on the RV and modulate its response to pressure or volume overload [22]. Similar to the remodeling of the left ventricle, RV remodeling in response to pressure or volume overload is intricately associated with alterations in the function of cardiomyocytes, fibroblasts, endothelial cells, and various immune and inflammatory cells [34][35][36][34,35,36]. These cells are critically involved in cardiac remodeling, and their dysfunction can be caused by a multitude of factors and mediators synthesized and released by various cells within the RV myocardium [36]. Interactions between different cell types play a vital role in determining the overall outcome. Another hallmark of RV remodeling is the increased production and deposition of extracellular matrix proteins. Ultimately, this alters the microenvironment of the myocardial cells and leads to a rise in tissue stiffness and expansion of the intercellular space within the heart [37]. The pathogenesis of the deleterious events during the course of RV remodeling involves a complex interplay of various processes and signaling pathways, including inflammation [22], extracellular matrix synthesis [38], calcium homeostasis [39], endothelial cell dysfunction [40], nitric oxide (NO) synthesis [41], endothelial-mesenchymal transition [42], matricellular protein synthesis [43] and growth factor signaling pathways such as transforming growth factor-β (TGF-β) [44] and apelin [45]. These interactions collectively dictate the fate of the RV under pressure or volume overload, and a better understanding of these intricate processes is essential to developing effective therapeutic strategies for the prevention or management of RV dysfunction and failure.3. Mast Cell Biology
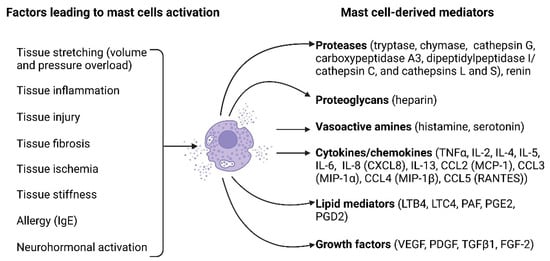
The pivotal role of mast cells in allergic responses has long been recognized [46]. However, recent studies have suggested their involvement in various pathological processes associated with different non-allergic diseases, such as tissue remodeling, repair, fibrosis, and angiogenesis [46][47][46,47]. Mast cells represent immune cells residing within the peripheral tissues and originate from bone marrow-derived precursor cells, regulated by key growth factors such as c-KIT ligand stem cell factor [48]. Mast cells express numerous cell surface antigens, including the cytokine receptor KIT (CD117) and the high-affinity receptor for the Fc region of immunoglobulin E (FcεRI). They are often identified as c-kit+FcεRI+ [49][50][51][49,50,51]. Mast cells also express the pan leukocyte antigen (CD45); however, they do not express surface antigens specific for other hematopoietic cells like CD2, CD3, CD4, CD11a, CD11b, CD11c, CD14, CD15, CD19, etc. [52][53][52,53]. Evaluation of the expression of these antigens allows distinguishing between mast cells and other CD45+ cells [54]. The most commonly used method for histochemical identification of mast cells in tissue sections is toluidine blue staining [55]. Morphologically, mast cells are identified by the presence of multiple large metachromatic granules in their cytoplasm, which store a variety of mediators, cytokines, and proteases [56]. Mast cell activation can be mediated by the binding of antigens and antibodies to their membrane [57]. Additionally, activation may occur in response to diverse stimuli, including neuropeptides (substance P, vasoactive intestinal peptide), calcitonin gene-related peptide, and neurotensin), basic compounds (compound 48/80), inflammatory mediators, and certain drugs [57]. Figure 1 illustrates the key factors causing mast cell activation and the biologically active substances released by mast cells upon their activation.Figure 1. Mast cell activation factors and mast cell-derived mediators. A multitude of factors can induce mast cell activation and encompass tissue stretching due to pressure or volume overload, tissue inflammation, tissue injury, tissue fibrosis, tissue ischemia, tissue stiffness, allergies, and neurohormonal activation. Upon activation, mast cells release a diverse array of biologically active substances, including proteases (such as tryptase, chymase, cathepsin G, carboxypeptidase A3, dipeptidyl peptidase I (DPPI, cathepsin C), cathepsins L and S, and renin), proteoglycans (heparin), vasoactive amines (histamine and serotonin), cytokines/chemokines (such as TNFα, IL-2, IL-4, IL-5, IL-6, IL-8 [CXCL8], IL-13, CCL2 [MCP-1], CCL3 [MIP-1α], CCL4 [MIP-1β], and CCL5 [RANTES]), lipid mediators (LTB4, LTC4, PAF, PGE2, PGD2), and growth factors (VEGF, PDGF, TGFβ1, FGF-2). The figure was created using BioRender.com, accessed on 25 November 2023.
Upon mast cell activation, their degranulation follows [58]. Degranulated mast cells in tissues can be identified using toluidine blue staining by a reduced granule content in their cytoplasm and by extracellular metachromatic granules in their immediate vicinity [59][60][59,60]. For the quantification of mast cell activation, the number of degranulated cells is expressed as a percent of the total number of mast cells [61]. Expression of some surface antigens, including CD63, CD200R1 and CD203c, was reported to significantly increase because of mast cell degranulation and was proposed as a surrogate molecular marker for mast cell activation [62].
Mast cells exert their effects through the release of various mediators, which are pre-stored in the granules or synthesized upon mast cell activation. The biologically active substances released by mast cells are then involved in various processes. Many factors released by mast cells, including histamine, heparin, proteoglycans, serotonin, and proteases, are preformed and stored in the granules [63].
4. Mast Cell-Deficient Lines to Study Cardiac Physiology and Remodeling
Mast cell-deficient lines have significantly deepened our knowledge of mast cell biology and their role in diseases. The most frequently used in biomedical research mast cell-deficient mouse lines carry naturally occurring mutations in the white spotting (W) locus on mouse chromosome 5, which encodes the c-KIT proto-oncogene [64][66]. All these mutations lead to reduced receptor tyrosine kinase KIT-dependent signaling and severe mast cell deficiency, as the development of mast cells is critically dependent on the binding of the growth factor stem cell factor to its receptor KIT [65][67].
KitW/W-v mice are double heterozygotes, which carry two mutant alleles, W and W-v [66][70]. The W mutant allele is characterized by a point mutation at a splicing site in the transcript, resulting in a truncated KIT protein lacking kinase activity, whereas the Wv mutant allele represents a point mutation in the kinase domain of the c-KIT coding sequence, resulting in decreased tyrosine kinase activity [66][70]. KitW/W homozygotes mice display severe anemia and neutropenia; however, they die around the first week of life [67][68]. KitW-v homozygotes also exhibit severe anemia, and many of them survive to maturity (hence “v” for “viable”) [67][68]. KitW/W-v mice, which combine the severe KitW with the milder KitW-v mutation, have widely been used in biomedical research for their favorable survival and vigor [68][71].
KitW-sh/W-sh mice bear a spontaneous inversion mutation W-sash (W-sh) in the transcriptional regulatory elements upstream of the c-KIT transcription start site [69][72]. The defects caused by the W-sh mutations are confined to melanogenesis and mast cells. Heterozygotes are black with a broad white belt at the midline (hence the name and symbol sash) [70][73]. KitW-sh/W-sh mice are fertile and not anemic, which makes them more preferable than KitW/W-v mice in certain disease models [71][74]. However, the inversion in KitW-sh/W-sh mice also disrupts the gene encoding the pro-atrial natriuretic peptide (ANP) convertase corin, which is responsible for proteolytic cleavage of pro-ANP to produce ANP [72][75].
5. Mast Cells in Healthy Hearts
Besides cardiomyocytes, endothelial cells and fibroblasts, heart tissue contains a number of other cell types, including various immune and inflammatory cells [73][74][97,98]. The immune cells in the healthy myocardium comprise mast cells, macrophages, T lymphocytes (CD4+ and CD8+), natural killer cells, eosinophils, B cells, dendritic cells, neutrophils, monocytes, and plasma cells. These immune cells are involved in the maintenance of tissue homeostasis, regulation of inflammation, tissue repair, and heart protection against potential pathogens [74][98]. Cardiac mast cells are generally located in the interstitial space between cardiomyocytes and are closely associated with coronary vessels [75][99] and nerves [76][100]. They constitute only a small part of the immune cells present within the healthy myocardium. According to a recent single-cell RNA sequencing analysis, mast cells constituted less than 1% of all CD45+ immune cells in the healthy mouse myocardium [54]. In this study, the authors identified mast cells in cluster 19 of the single cell sequencing results, which expressed the mast cell marker Mcpt8 and the mast cell-associated cytokines IL4 and IL13 [54]. Mast cell distribution exhibits significant variation within the wall of mouse hearts; they are most prevalent in the epicardium (50%) and myocardium (45%), with fewer numbers in the endocardium (5%) [77][103]. In contrast, in healthy rats, mast cell numbers appear to be similar in both the subepicardial and subendocardial layers of the left ventricle [78][104]. Mast cells are known for their heterogeneity, so the phenotypes of cardiac mast cells differ from those found in other tissues. In contrast to mast cells found in human skin and lungs, mast cells in human hearts demonstrate slightly different patterns of mediator release and synthesis [79][113]. Upon cross-linking of IgE receptors on human heart mast cells, histamine, tryptase, leukotriene C4, and prostaglandin D2 are released, although they differ quantitatively and qualitatively compared to skin and lung mast cells [79][113]. Mast cell heterogeneity is also evident from the patterns of mediator release. Human heart mast cells respond to C5a and protamine by releasing histamine in a similar way as skin mast cells; however, they differ from lung mast cells in this aspect [79][113].6. Mast Cells in Right Ventricular Physiology and Remodeling
Various immune and inflammatory cells are crucially involved in cardiac remodeling [22]. Notably, the content of immune cells in the RV differs from that in the left ventricle in physiological as well as pathological conditions [80][116]. Specifically, the number of CD45+/CD11b/c+ cells was on average four times higher in the RV than in the left ventricle in rats exposed to either normoxia or hypoxia, suggesting a higher content of immune cells in the RV. A substantial body of evidence has accumulated supporting the involvement of mast cells in left heart hypertrophy and failure. However, the role of mast cells in RV hypertrophy and failure remains insufficiently explored. In pathological conditions associated with left ventricular remodeling, mast cell numbers in the left ventricle were increased and exhibited more dynamic changes compared to the RV in animals as well as in humans. Activation of mast cells in response to pressure overload occurs early after exposure to the stressor, as evidenced by increased mast cell degranulation in the RV of mice 3 days following pulmonary artery banding (PAB) surgery [81][117]. The source of increased mast cell numbers in RV remodeling remains to be elucidated. In left ventricular remodeling induced by angiotensin II infusion, the increase in mast cell density was shown to result from the maturation of pre-existing immature mast cells [82][89]. SHR commonly serves as a model of systemic arterial hypertension and left ventricular hypertrophy. Enhanced myocardial fibrosis, increased collagen volume fraction, and elevated hydroxyproline levels in the left ventricle in SHR were closely linked to an increased accumulation of mast cells in the left ventricle [83][106]. The evidence for the pathological role of mast cells in adverse RV remodeling was further provided in experiments exploiting mast cell-deficient mice and pharmacological inhibition of mast cell activation [84][87]. Treatment of wild-type mice subjected to pressure overload by PAB with the mast cell stabilizer cromolyn significantly improved RV remodeling and function [84][87]. Accumulating evidence suggests that mast cells may also play a protective role in myocardial remodeling [51][85][51,124]. Moreover, mast cells and their granules exert protective effects in the acute phase after myocardial infarction in rats via improving cardiomyocyte survival and vascularization [86][110]. Mast cell population heterogeneity could account for the diversity of mast cell effects [87][125].7. Mechanisms of Mast Cell-Mediated Effects on the Heart
7.1. Effects of Mast Cells on Cardiomyocytes
Mediators released by activated mast cells may exert direct effects on cardiomyocytes and impact their survival, apoptosis, contraction, and arrhythmogenesis. Experiments with adoptive transfer of bone marrow-derived mast cells from wild-type mice or corresponding knockout mice to mast cell-deficient KitW-sh/W-sh mice with diabetic cardiomyopathy demonstrated a role of mast cell-derived IL6 and TNF-α in promoting cardiomyocyte death [88][130]. The mast cell-derived mediator histamine, which is present in the human heart at high concentrations, was shown to reduce cell viability and induce cardiomyocyte apoptosis [89][131]. In line with these observations, pharmacological inhibition, or genetic disruption of the histamine H2 receptor slowed heart failure progression in mice subjected to pressure overload through a reduction of myocardial apoptosis [89][131]. In cardiac volume overload, chymase uptake by cardiomyocytes resulted in myosin degradation and cardiomyocyte dysfunction [90][133]. In contrast, mast cell deficiency led to reduced contractility and myofilament Ca2+ sensitization after myocardial infarction in mice, suggesting an important role of cardiac mast cells in preserving postischemic cardiac function [51].7.2. Mast Cells and Extracellular Matrix Modulation
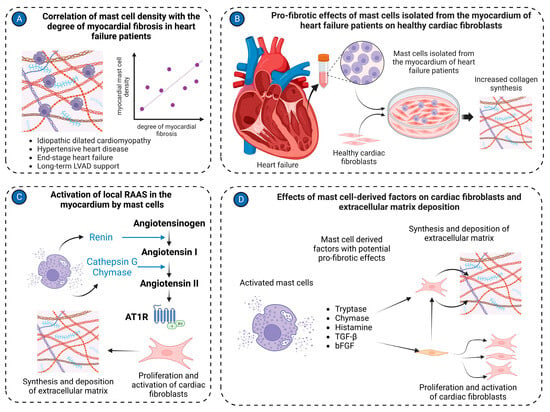
Myocardial fibrosis plays a pivotal role in the pathogenesis and progression of various cardiac diseases [38]. Elucidating the precise mechanisms underlying myocardial fibrosis development is crucial for understanding disease pathogenesis and identifying novel therapeutic targets [91][138]. Myocardial fibrosis involves an interplay of versatile processes, including the synthesis and turnover of extracellular matrix proteins, the activation and proliferation of cardiac fibroblasts, as well as the synthesis of diverse inflammatory mediators and growth factors with potent pro-fibrotic properties [92][139]. These intricate events are meticulously orchestrated by various cell types residing within the myocardium, including various immune cells [92][93][94][139,140,141]. Recent studies have implicated mast cells as significant contributors to myocardial fibrosis [95][142]. In patients with idiopathic dilated cardiomyopathy, a notable association was demonstrated between mast cell density and the severity of myocardial fibrosis [96][143]. Experimental studies provided further evidence to support the link between mast cell activation and myocardial fibrosis development. In Dahl salt-sensitive rats, degranulated mast cells were found to localize near fibrotic regions in the myocardium [97][146]. Chymase inhibition with chymostatin reduced myocardial active TGF-β1 levels in rats subjected to pressure overload by transverse aortic constriction (TAC), suggesting that activation of latent TGF-β1 is one of the pathways by which cardiac mast cell-derived chymase contributes to myocardial fibrosis [98][148]. Besides TGF-β1 activation, chymase induced TGF-β1 expression in a dose-dependent fashion in rat cardiac fibroblasts [99][149]. Another pathway by which mast cells can contribute to myocardial fibrosis is the activation of the RAAS in the heart. Mast cells are recognized as a significant source of renin in the myocardium, which consequently converts angiotensinogen to angiotensin I [76][100][100,152]. Next, cathepsin G [101][153] and chymase [102][103][154,155] derived from activated mast cells convert angiotensin I into angiotensin II. Angiotensin II subsequently exerts pro-fibrotic effects on the myocardium [104][156] through angiotensin II receptors, which are present on cardiac fibroblasts and mediate multiple pro-fibrotic effects [104][105][156,157]. Activated mast cells release a number of other factors, including histamine [89][131] and tryptase [106][107][101,158] that might account for their pro-fibrotic activities on cardiac fibroblasts. Treatment of isolated cardiac fibroblasts with tryptase induced increased collagen synthesis and fibroblast proliferation [106][107][101,158]. Collagen production was enhanced via activation of the protease-activated receptor-2 and ERK1/2 signaling [107][158]. The relevance of in vitro findings was further corroborated by the reduction of myocardial fibrosis in spontaneously hypertensive rats treated with a tryptase inhibitor [107][158]. MMP/tissue inhibitors of the metalloproteinases system play a key role in the modulation of the extracellular matrix in pathological conditions. Several lines of evidence implicate mast cells in the regulation of this system in volume overload-induced cardiac remodeling (Figure 23).Figure 23. Mast cell in cardiac fibrosis. (A) Mast cell density positively correlates with the degree of myocardial fibrosis in the left ventricular tissues isolated from patients with various cardiac pathologies, including idiopathic dilated cardiomyopathy, hypertensive heart disease, end-stage heart failure, and long-term LVAD support; (B) Mast cells isolated from cardiac tissues of heart failure patients stimulate activation of healthy cardiac fibroblasts, causing them to synthesize and release extracellular matrix molecules in co-culture experiments; (C) Mast cells activate the local RAAS in the myocardium. Renin produced by mast cells can convert angiotensinogen to angiotensin I. Cathepsin G and chymase derived from mast cells transform angiotensin I to angiotensin II. Angiotensin II stimulates cardiac fibroblasts to synthesize extracellular matrix molecules; (D) Several factors derived from mast cells, such as tryptase, chymase, histamine, TGF-β, and bFGF, activate cardiac fibroblasts to myofibroblasts and stimulate production of extracellular matrix molecules. The figure was created using BioRender.com, accessed on 25 November 2023.
7.3. Mast Cells and Myocardial Vascularization
Most cardiac pathologies are associated with changes in myocardial vascularization [40][108][40,165]. Mast cells are present in the walls of both microvessels and larger coronary arteries, suggesting their potential involvement in both micro- and macrovascular pathologies of the coronary arteries (Figure 34).
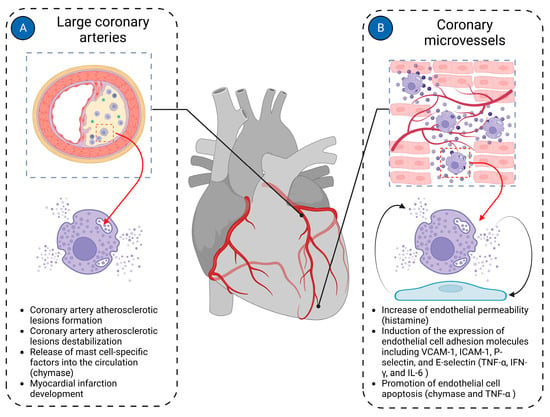
Figure 34. Mast cells in cardiac vasculature. Mast cells in the cardiac vasculature have been implicated in the pathologies of both large coronary arteries and coronary microvasculature. (A) In large coronary arteries, mast cells are mainly involved in the pathogenesis of coronary atherosclerotic plaque formation and contribute to its instability, ultimately leading to the development of myocardial infarction; (B) In coronary microvessels, mast cells primarily interact with endothelial cells, modulating their functions. Histamine derived from mast cells increases the permeability of endothelial cells. Mast cell-derived TNF-α, IFN-γ, and IL-6 induce expression of endothelial cell adhesion molecules such as VCAM-1, ICAM-1, P-selectin, and E-selectin. Chymase and TNF-α derived from mast cells promote endothelial cell apoptosis. The figure was created using BioRender.com, accessed on 25 November 2023.
Mast cells have been shown to induce left ventricular diastolic dysfunction in various animal models of heart failure [109][110][166,167]. Abnormal mast cell activation was identified as a cause of cardiac microvessel disease in Leprdb/db female mice, another experimental model of diastolic dysfunction associated with heart failure with preserved ejection fraction [61]. The cardiac microvessel disease was characterized by enhanced vessel permeability due to disruption of endothelial adherens junctions by mast cell-derived histamine [61]. Histamine released by mast cells may interact with both H1 and H2 receptors to exert its effects on the cardiac endothelial cells and contribute to heart failure development [111][168].
Increased serum tryptase levels were reported in patients with stable coronary artery disease, suggesting that chronic low-grade inflammation in atherosclerotic plaques triggers mast cell activation [112][170]. In vitro experiments demonstrated that activated mast cells might contribute to plaque erosion by inducing endothelial cell apoptosis [113][114][171,172].
7.4. Mast Cells and Myocardial Inflammation
Myocardial inflammation in various cardiac pathologies is recognized as a significant contributor to adverse myocardial remodeling in both ventricles [22]. The importance of mast cells in this process is emphasized by the fact that they possess a variety of inflammatory mediators in their granules and are able to rapidly generate more inflammatory agents upon activation [115][177]. Activated mast cells release a number of inflammatory factors, including interleukins (IL-1, IL-3, IL-4, IL-5, IL-6, IL-8, IL-10, IL-13, and IL-17), TNF-α, and chemokines (CXCL8/IL-8, CCL2/MCP-1, CCL3/MIP-1α, CCL4/MIP-1β, and CCL5/RANTES) [56].
Inflammatory mediators released by mast cells can enhance myocardial inflammation by activating further inflammatory processes. In canine experimental cardiac ischemia-reperfusion, mast cells primarily released TNF-α, which then exacerbated myocardial inflammation and cardiac injury by upregulating IL-6 in infiltrating leukocytes and initiating the cytokine cascade [116][178]. In line with this report, attenuated myocardial injury in mast cell-deficient KitW/KitW-v mice following myocardial ischemia-reperfusion was associated with lower serum IL-6 compared to their wild-type counterparts [117][83].
Markedly elevated myocardial TNF-α levels in response to cardiac volume overload were observed in wild-type rats at 5 days post-fistula; conversely, TNF-α was almost undetectable in the hearts of mast cell-deficient rats [118][164].