A large body of research shows an association between higher body weight and low vitamin D status, as assessed using serum 25-hydroxyvitamin D concentrations. Vitamin D can be metabolised in adipose tissue and has been reported to influence gene expression and modulate inflammation and adipose tissue metabolism in vitro. However, the exact metabolism of vitamin D in adipose tissue is currently unknown. White adipose tissue expresses the vitamin D receptor and hydroxylase enzymes, substantially involved in vitamin D metabolism and efficacy. The distribution and concentrations of the generated vitamin D compounds in adipose tissue, however, are largely unknown. Closing this knowledge gap could help to understand whether the different vitamin D compounds have specific health effects in the setting of adiposity.
- C3 epimer
- inflammation
- metabolic health
- obesity
- overweight
- 25-hydroxyvitamin D
1. Introduction
1.1. Vitamin D Metabolism
The precursors of 25(OH)D include vitamin D3 (cholecalciferol), which is found in animal products, and vitamin D2 (ergocalciferol), which is mainly present in mushrooms [31,32][14][15]. In humans, vitamin D3 can also be generated in the skin by photosynthesis after UVB exposure of the precursor 7-dehydrocholesterol. Vitamin D2 and vitamin D3 follow the same metabolic pathway. The term vitamin D is used when vitamin D2 or D3 could be used interchangeably. The conversion of vitamin D to its different compounds is achieved through the action of cytochrome P450 enzymes, for example, vitamin D 25-hydroxylases (CYP2R1, CYP27A1 and CYP2J2), 1α-hydroxylase (CYP27B1) and the aforementioned CYP24A1. The activity of these enzymes is partially dependent on magnesium as a cofactor [33,34][16][17]. Hydroxylase enzymes are mainly expressed in the liver and kidney, as well as in other tissues and cell types, such as testes, blood cells, immune cells and adipose tissue [30][18]. Vitamin D is converted in the liver (25 hydroxylases) and kidneys (1α hydroxylases) into bioactive 1,25-dihydroxyvitamin D (1,25(OH)2D). Vitamin D is catabolised by 1,25-dihydroxyvitamin D hydroxylase (CYP24A1) to 24,25-dihydroxyvitamin D (24,25(OH)2D) or 1,24,25-trihydroxyvitamin D (1,24,25(OH)3D) [30][18]. In circulation, vitamin D compounds are bound to the vitamin D binding protein (DBP) and albumin. A schematic overview of vitamin D metabolism is provided in Figure 1. Vitamin D binds to the vitamin D receptor (VDR), which is expressed in almost all human tissues, including adipose tissue [35][19]. After binding, the VDR forms a complex with the retinoid X receptor (RXR). This complex is transferred to the nucleus, where it acts as a transcription factor. Many genes have a vitamin D response element (VDRE) in their promotor regions. Target genes are related to inflammatory processes and cell differentiation, in addition to bone and calcium metabolism [36][20]. The transcription regulation by vitamin D is reported to be highly tissue-specific.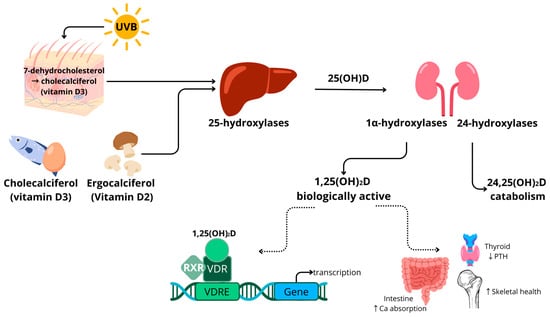
1.2. Vitamin D in Adiposity
Two meta-analyses demonstrated a significantly higher prevalence of low vitamin D levels (serum 25(OH)D < 30 ng/mL) in adults and children with higher body weight [39,40][22][23]. Currently, the major hypotheses for this association are the sequestration of fat-soluble vitamin D in an increased amount of adipose tissue in people with elevated body fat mass [41][24] and the volumetric distribution of vitamin D over a larger amount of body mass [42][25]. Logically, this leads to the hypothesis that weight loss could contribute to achieving vitamin D sufficiency in people with higher body weight. However, the findings are currently inconclusive. Blum et al. showed a correlation between serum vitamin D3 and WAT vitamin D3 levels [43][26]. They measured a mean vitamin D3 content in WAT of 102.8 ± 42 nmol/kg in people with a mean body mass index (BMI) of 50.6 kg/m2. This means that serum vitamin D could significantly improve upon weight loss if all vitamin D is released from adipose tissue. However, Himbert et al. reviewed the effect of surgery and diet-induced weight loss on serum 25(OH)D concentrations, and they concluded that weight loss did increase serum 25(OH)D levels but that this is often not enough to reach sufficient vitamin D concentrations [44][27]. The expression and protein secretion of the hydroxylase enzymes involved in the conversion of vitamin D have been reported in many tissues, including WAT [47][28]. Human adipocytes were shown to express CYP27B1, as well as CYP24A1 [48][29]. The expression of the enzymes CYP2R1 and CYP2J2 was also shown in human adipose tissue [49][30]. Jonas et al. demonstrated an increased CYP27B1 expression in WAT of people with higher body weight (BMI > 40 kg/m2) [50][31]. In another study, however, the expression of CYP2J2 and CYP27B1 was decreased in women with higher body weight (BMI > 35 kg/m2) [49][30]. These contradicting results illustrate that more research is necessary to understand the link between vitamin D metabolism and adipose tissue. However, hypotheses do exist; for example, the expression of CYP24A1 in adipose tissue could lead to an increased degradation of 1,25(OH)2D in people with higher body weight. This effect could be aggravated by the concomitant downregulation of CYP2R1, another 25-hydroxylase, which was seen in a mouse model of obesity [51][32]. Such changes in hydroxylase enzyme expression could be a partial explanation for the decreased vitamin D status in people with higher body weight and underline the link between adipose tissue and vitamin D metabolism. In addition to hydroxylase enzymes, adipocytes express the VDR [48[29][30],49], meaning that vitamin D compounds binding the receptor can have a direct local effect on gene transcription in adipose tissue. Adipose VDR is reported to be increased in obesity [50][31]. A genomic study showed that the rs3782905 single-nucleotide polymorphism (SNP) in the VDR gene is associated with differences in adiposity [52][33], which indicates a relation between vitamin D signalling and the development of adipose tissue. However, the impact of different VDR genotypes on the development of adiposity is not supported by all data [53][34]. Together, these findings on hydroxylase enzymes and VDR expression indicate once again that vitamin D metabolism is linked to adipose tissue mass. The relations between WAT and vitamin D metabolism in people with higher body weight are depicted in Figure 2.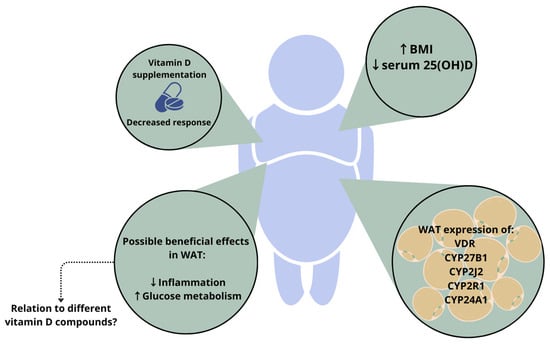
2. Relevance of Different Vitamin D Compounds
2.1. Free Vitamin D Compound
2.2. 1,25-Dihydroxyvitamin D (1,25(OH)
2
D)
The 1,25(OH)2D compound is generally considered the active form due to its high affinity for the VDR [77][52]. With regard to the anti-inflammatory effects of 1,25(OH)2D, NFkB signalling has been implicated as a potential mechanism, since vitamin D has been reported to decrease NFkB expression [12][53] and to block NFkB translocation to the nucleus [13,78[54][55][56],79], thus decreasing the transcription of pro-inflammatory cytokines. Even though these findings directly link 1,25(OH)2D to decreased inflammation in vitro, there are contradicting reports of the effects of vitamin D supplementation on inflammatory markers in vivo. Wamberg et al. [80][57] observed a diminishing effect on inflammation in an adipocyte cell line treated with 1,25(OH)2D3. However, this effect was not reproduced in primary human adipocytes, and it was not reflected in circulating inflammatory markers in vivo [80][57]. Adipokines are messenger molecules produced by adipocytes. They affect energy metabolism, insulin resistance, inflammation and blood pressure and are strongly related to metabolic health [84,85][58][59]. Two well-known examples are leptin and adiponectin. Leptin is known as the satiety hormone, which, in healthy conditions, supresses food intake, regulates energy metabolism and acts as a negative feedback loop upon adipose tissue accumulation [86,87][60][61]. However, in people with higher body weight, leptin resistance frequently occurs [88,89,90][62][63][64]. Adiponectin is an adipose-tissue-derived hormone with health-promoting effects. It has been reported to increase insulin sensitivity and have anti-inflammatory properties [91][65]. Adiponectin levels are often decreased in people with increased body fat [92][66]. The effects of 1,25(OH)2D exposure on adiponectin have also been reported, e.g., decreased adiponectin production in human primary adipocytes [99][67]. Accordingly, a negative association between adiponectin levels and serum 25(OH)D was observed in humans [97][68]. However, this effect was only reported in a subgroup of participants with a BMI > 25 kg/m2. In another study, no association between serum 25(OH)D and adiponectin was reported [100][69]. And yet another study found a positive correlation between 25(OH)D and adiponectin levels [96][70]. Two trials did not show an effect of vitamin D on adipokine levels [101,102][71][72].2.3. 24,25-Dihydroxyvitamin D (24,25(OH)
2
D)
The 24,25(OH)2D compound is a clearance product in the vitamin D metabolic cascade. The ratio of 24,25(OH)2D to 25(OH)D has been suggested to be an alternative marker of vitamin D status [103][73]. This ratio takes vitamin D metabolism and feedback loops into account and is not dependent on the level of DBP [104,105][74][75]. When assessing other vitamin D compounds, Binkley et al. described the predictive value of 24,25(OH)2D for the response to vitamin D supplementation [20][10]. In this study, the ratio of 24,25(OH)2D/25(OH)D did not predict the response to vitamin D supplementation, contradicting earlier suggestions of 24,25(OH)2D/25(OH)D being an improved status marker [103,106][73][76]. However, the sample size was relatively small (n = 62) and consisted of postmenopausal women only. These data indicate that the measurement of 24,25(OH)2D could have an additional clinical relevance to measuring only serum 25(OH)D [106][76].2.4. C-3 Epimers of Vitamin D Compounds
In vitamin D metabolism, a parallel C-3 epimerisation pathway introduces additional vitamin D compounds. The most important of these is the C-3α isomer of 25(OH)D, which results from the reversal of the stereochemical configuration of the –OH group at C-3 (3β→3α). It is important to measure this compound for two reasons. Firstly, the 3α epimer has been reported to lead to the overestimation of vitamin D status with current detection methods, such as immunoassays and MS assays, if it is not properly separated [109][77]. The extent of this additional contribution depends on physiological and pathological conditions and age; e.g., 3α levels are naturally higher in newborns, especially in those born prematurely [110,111][78][79]. With respect to body composition, a negative correlation was reported for serum 25(OH)D concentrations and fat mass in infants at 12 months in a vitamin D supplementation trial [113][80]. The authors reported that serum 25(OH)D was a predictor of lean mass and fat mass in regression models. This correlation was only present at the age of three months for 3α-25(OH)D, even though 3β-25(OH)D was associated with all time points. In a Thai national health survey, the relative amount of 3α-25(OH)D3 was associated with age, sex and living conditions [114][81]. Males and people living in rural areas had higher relative concentrations of serum 3α-25(OH)D3. The survey observed a negative correlation between BMI and 3β-25(OH)D, but not 3α-25(OH)D. Another study that included women with polycystic ovary syndrome (PCOS) and healthy controls did not observe differences between the two groups in 3β and 3α-25(OH)D3 [115][82].References
- Holick, M.F. Vitamin D and bone health. J. Nutr. 1996, 126, 1159S–1164S.
- Holick, M.F. The role of vitamin D for bone health and fracture prevention. Curr. Osteoporos. Rep. 2006, 4, 96–102.
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110.
- Holick, M.F. Deficiency of sunlight and vitamin D. BMJ 2008, 336, 1318–1319.
- Cashman, K.D. Vitamin D deficiency: Defining, prevalence, causes, and strategies of addressing. Calcif. Tissue Int. 2020, 106, 14–29.
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930.
- Dissanayake, H.A.; de Silva, N.L.; Sumanatilleke, M.; de Silva, S.D.N.; Gamage, K.K.K.; Dematapitiya, C.; Kuruppu, D.C.; Ranasinghe, P.; Pathmanathan, S.; Katulanda, P. Prognostic and therapeutic role of vitamin D in COVID-19: Systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2022, 107, 1484–1502.
- Shah, K.; Saxena, D.; Mavalankar, D. Vitamin D supplementation, COVID-19 and disease severity: A meta-analysis. QJM Int. J. Med. 2021, 114, 175–181.
- Bikle, D.; Bouillon, R.; Thadhani, R.; Schoenmakers, I. Vitamin D metabolites in captivity? Should we measure free or total 25 (OH) D to assess vitamin D status? J. Steroid Biochem. Mol. Biol. 2017, 173, 105–116.
- Binkley, N.; Borchardt, G.; Siglinsky, E.; Krueger, D. Does vitamin D metabolite measurement help predict 25 (OH) D change following vitamin D supplementation? Endocr. Pract. 2017, 23, 432–441.
- Makris, K.; Sempos, C.; Cavalier, E. The measurement of vitamin D metabolites part II—The measurement of the various vitamin D metabolites. Hormones 2020, 19, 97–107.
- Wildman, R.P.; Muntner, P.; Reynolds, K.; McGinn, A.P.; Rajpathak, S.; Wylie-Rosett, J.; Sowers, M.R. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: Prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004). Arch. Intern. Med. 2008, 168, 1617–1624.
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.L.; Foka, A.J.; Ndoadoumgue, A.L. Geographic distribution of metabolic syndrome and its components in the general adult population: A meta-analysis of global data from 28 million individuals. Diabetes Res. Clin. Pract. 2022, 188, 109924.
- Rao, D.S.; Raghuramulu, N. Food chain as origin of vitamin D in fish. Comp. Biochem. Physiol. Part A Physiol. 1996, 114, 15–19.
- Atsuko, T.; Toshio, O.; Makoto, T.; Tadashi, K. Possible origin of extremely high contents of vitamin D3 in some kinds of fish liver. Comp. Biochem. Physiol. Part A Physiol. 1991, 100, 483–487.
- Uwitonze, A.M.; Razzaque, M.S. Role of magnesium in vitamin D activation and function. J. Osteopath. Med. 2018, 118, 181–189.
- Risco, F.; Traba, M. Influence of magnesium on the in vitro synthesis of 24, 25-dihydroxyvitamin D3 and 1 alpha, 25-dihydroxyvitamin D3. Magnes. Res. 1992, 5, 5–14.
- Saponaro, F.; Saba, A.; Zucchi, R. An update on vitamin D metabolism. Int. J. Mol. Sci. 2020, 21, 6573.
- Plum, L.A.; DeLuca, H.F. Vitamin D, disease and therapeutic opportunities. Nat. Rev. Drug Discov. 2010, 9, 941–955.
- Carlberg, C. Vitamin D and Its Target Genes. Nutrients 2022, 14, 1354.
- Goltzman, D.; Mannstadt, M.; Marcocci, C. Physiology of the calcium-parathyroid hormone-vitamin D axis. Vitam. D Clin. Med. 2018, 50, 1–13.
- Pereira-Santos, M.; Costa, P.d.F.; Assis, A.d.; Santos, C.d.S.; Santos, D.d. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349.
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A. Vitamin D insufficiency in overweight and obese children and adolescents. Front. Endocrinol. 2019, 10, 103.
- Abbas, M.A. Physiological functions of Vitamin D in adipose tissue. J. Steroid Biochem. Mol. Biol. 2017, 165, 369–381.
- Drincic, A.T.; Armas, L.A.; Van Diest, E.E.; Heaney, R.P. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity 2012, 20, 1444–1448.
- Blum, M.; Dolnikowski, G.; Seyoum, E.; Harris, S.S.; Booth, S.L.; Peterson, J.; Saltzman, E.; Dawson-Hughes, B. Vitamin D3 in fat tissue. Endocrine 2008, 33, 90–94.
- Himbert, C.; Ose, J.; Delphan, M.; Ulrich, C.M. A systematic review of the interrelation between diet-and surgery-induced weight loss and vitamin D status. Nutr. Res. 2017, 38, 13–26.
- Li, J.; Byrne, M.E.; Chang, E.; Jiang, Y.; Donkin, S.S.; Buhman, K.K.; Burgess, J.R.; Teegarden, D. 1α, 25-Dihydroxyvitamin D hydroxylase in adipocytes. J. Steroid Biochem. Mol. Biol. 2008, 112, 122–126.
- Nimitphong, H.; Holick, M.F.; Fried, S.K.; Lee, M.-J. 25-hydroxyvitamin D3 and 1, 25-dihydroxyvitamin D3 promote the differentiation of human subcutaneous preadipocytes. PLoS ONE 2012, 7, e52171.
- Wamberg, L.; Christiansen, T.; Paulsen, S.; Fisker, S.; Rask, P.; Rejnmark, L.; Richelsen, B.; Pedersen, S. Expression of vitamin D-metabolizing enzymes in human adipose tissue—The effect of obesity and diet-induced weight loss. Int. J. Obes. 2013, 37, 651–657.
- Jonas, M.I.; Kuryłowicz, A.; Bartoszewicz, Z.; Lisik, W.; Jonas, M.; Kozniewski, K.; Puzianowska-Kuznicka, M. Vitamin D receptor gene expression in adipose tissue of obese individuals is regulated by miRNA and correlates with the pro-inflammatory cytokine level. Int. J. Mol. Sci. 2019, 20, 5272.
- Elkhwanky, M.S.; Kummu, O.; Piltonen, T.T.; Laru, J.; Morin-Papunen, L.; Mutikainen, M.; Tavi, P.; Hakkola, J. Obesity represses CYP2R1, the vitamin D 25-hydroxylase, in the liver and extrahepatic tissues. JBMR Plus 2020, 4, e10397.
- Ochs-Balcom, H.M.; Chennamaneni, R.; Millen, A.E.; Shields, P.G.; Marian, C.; Trevisan, M.; Freudenheim, J.L. Vitamin D receptor gene polymorphisms are associated with adiposity phenotypes. Am. J. Clin. Nutr. 2011, 93, 5–10.
- Ruiz-Ojeda, F.J.; Anguita-Ruiz, A.; Leis, R.; Aguilera, C.M. Genetic factors and molecular mechanisms of vitamin D and obesity relationship. Ann. Nutr. Metab. 2018, 73, 89–99.
- Tobias, D.K.; Luttmann-Gibson, H.; Mora, S.; Danik, J.; Bubes, V.; Copeland, T.; LeBoff, M.S.; Cook, N.R.; Lee, I.-M.; Buring, J.E. Association of Body Weight With Response to Vitamin D Supplementation and Metabolism. JAMA Netw. Open 2023, 6, e2250681.
- van den Heuvel, E.G.; Lips, P.; Schoonmade, L.J.; Lanham-New, S.A.; van Schoor, N.M. Comparison of the effect of daily vitamin D2 and vitamin D3 supplementation on serum 25-hydroxyvitamin D concentration (total 25 (OH) D, 25 (OH) D2 and 25 (OHD3) and importance of body mass index: A systematic review and meta-analysis. Adv. Nutr. 2023.
- Liu, J.; Fox, C.S.; Hickson, D.A.; May, W.D.; Hairston, K.G.; Carr, J.J.; Taylor, H.A. Impact of abdominal visceral and subcutaneous adipose tissue on cardiometabolic risk factors: The Jackson Heart Study. J. Clin. Endocrinol. Metab. 2010, 95, 5419–5426.
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.-Y.; Vasan, R.S.; Murabito, J.M.; Meigs, J.B.; Cupples, L.A. Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the Framingham Heart Study. Circulation 2007, 116, 39–48.
- Cancello, R.; Clement, K. Is obesity an inflammatory illness? Role of low-grade inflammation and macrophage infiltration in human white adipose tissue. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 1141–1147.
- Eckel, R.H.; Alberti, K.G.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2010, 375, 181–183.
- van Etten, E.; Mathieu, C. Immunoregulation by 1, 25-dihydroxyvitamin D3: Basic concepts. J. Steroid Biochem. Mol. Biol. 2005, 97, 93–101.
- Charoenngam, N.; Holick, M.F. Immunologic effects of vitamin D on human health and disease. Nutrients 2020, 12, 2097.
- Lei, X.; Zhou, Q.; Wang, Y.; Fu, S.; Li, Z.; Chen, Q. Serum and supplemental vitamin D levels and insulin resistance in T2DM populations: A meta-analysis and systematic review. Sci. Rep. 2023, 13, 12343.
- Farahmand, M.A.; Daneshzad, E.; Fung, T.T.; Zahidi, F.; Muhammadi, M.; Bellissimo, N.; Azadbakht, L. What is the impact of vitamin D supplementation on glycemic control in people with type-2 diabetes: A systematic review and meta-analysis of randomized controlled trails. BMC Endocr. Disord. 2023, 23, 15.
- Nykjaer, A.; Dragun, D.; Walther, D.; Vorum, H.; Jacobsen, C.; Herz, J.; Melsen, F.; Christensen, E.I.; Willnow, T.E. An endocytic pathway essential for renal uptake and activation of the steroid 25-(OH) vitamin D3. Cell 1999, 96, 507–515.
- Bikle, D.D. The free hormone hypothesis: When, why, and how to measure the free hormone levels to assess vitamin D, thyroid, sex hormone, and cortisol status. JBMR Plus 2021, 5, e10418.
- Mendel, C.M. The free hormone hypothesis: A physiologically based mathematical model. Endocr. Rev. 1989, 10, 232–274.
- Bikle, D.D.; Malmstroem, S.; Schwartz, J. Current controversies: Are free vitamin metabolite levels a more accurate assessment of vitamin D status than total levels? Endocrinol. Metab. Clin. 2017, 46, 901–918.
- Schwartz, J.; Lai, J.; Lizaola, B.; Kane, L.; Weyland, P.; Terrault, N.; Stotland, N.; Bikle, D. Variability in free 25 (OH) vitamin D levels in clinical populations. J. Steroid Biochem. Mol. Biol. 2014, 144, 156–158.
- Marques-Pamies, M.; López-Molina, M.; Pellitero, S.; Santillan, C.S.; Martínez, E.; Moreno, P.; Tarascó, J.; Granada, M.L.; Puig-Domingo, M. Differential behavior of 25 (OH) D and f25 (OH) D3 in patients with morbid obesity after bariatric surgery. Obes. Surg. 2021, 31, 3990–3995.
- Karlsson, T.; Osmancevic, A.; Jansson, N.; Hulthén, L.; Holmäng, A.; Larsson, I. Increased vitamin D-binding protein and decreased free 25 (OH) D in obese women of reproductive age. Eur. J. Nutr. 2014, 53, 259–267.
- Brommage, R.; Deluca, H.F. Evidence that 1, 25-dihydroxyvitamin D3 is the physiologically active metabolite of vitamin D3. Endocr. Rev. 1985, 6, 491–511.
- Nimitphong, H.; Guo, W.; Holick, M.F.; Fried, S.K.; Lee, M.J. Vitamin D inhibits adipokine production and inflammatory signaling through the vitamin D receptor in human adipocytes. Obesity 2021, 29, 562–568.
- Karkeni, E.; Bonnet, L.; Marcotorchino, J.; Tourniaire, F.; Astier, J.; Ye, J.; Landrier, J.-F. Vitamin D limits inflammation-linked microRNA expression in adipocytes in vitro and in vivo: A new mechanism for the regulation of inflammation by vitamin D. Epigenetics 2018, 13, 156–162.
- Marcotorchino, J.; Tourniaire, F.; Landrier, J.-F. Vitamin D, adipose tissue, and obesity. Horm. Mol. Biol. Clin. Investig. 2013, 15, 123–128.
- Mutt, S.J.; Karhu, T.; Lehtonen, S.; Lehenkari, P.; Carlberg, C.; Saarnio, J.; Sebert, S.; Hyppönen, E.; Järvelin, M.R.; Herzig, K.H. Inhibition of cytokine secretion from adipocytes by 1, 25-dihydroxyvitamin D3 via the NF-κB pathway. FASEB J. 2012, 26, 4400–4407.
- Wamberg, L.; Cullberg, K.; Rejnmark, L.; Richelsen, B.; Pedersen, S. Investigations of the anti-inflammatory effects of vitamin D in adipose tissue: Results from an in vitro study and a randomized controlled trial. Horm. Metab. Res. 2013, 45, 456–462.
- Trayhurn, P.; Bing, C.; Wood, I.S. Adipose tissue and adipokines—Energy regulation from the human perspective. J. Nutr. 2006, 136, 1935S–1939S.
- Sahu, B.; Bal, N.C. Adipokines from white adipose tissue in regulation of whole body energy homeostasis. Biochimie 2023, 204, 92–107.
- Gruzdeva, O.; Borodkina, D.; Uchasova, E.; Dyleva, Y.; Barbarash, O. Leptin resistance: Underlying mechanisms and diagnosis. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 191–198.
- Izquierdo, A.G.; Crujeiras, A.B.; Casanueva, F.F.; Carreira, M.C. Leptin, obesity, and leptin resistance: Where are we 25 years later? Nutrients 2019, 11, 2704.
- Prolo, P.; Wong, M.-L.; Licinio, J. Leptin. Int. J. Biochem. Cell Biol. 1998, 30, 1285–1290.
- Paul, R.F.; Hassan, M.; Nazar, H.S.; Gillani, S.; Afzal, N.; Qayyum, I. Effect of body mass index on serum leptin levels. J. Ayub Med. Coll. Abbottabad 2011, 23, 40–43.
- Kumar, R.; Mal, K.; Razaq, M.K.; Magsi, M.; Memon, M.K.; Memon, S.; Afroz, M.N.; Siddiqui, H.F.; Rizwan, A. Association of leptin with obesity and insulin resistance. Cureus 2020, 12, e12178.
- Wang, Z.V.; Scherer, P.E. Adiponectin, the past two decades. J. Mol. Cell Biol. 2016, 8, 93–100.
- Fang, H.; Judd, R.L. Adiponectin regulation and function. Compr. Physiol. 2011, 8, 1031–1063.
- Lorente-Cebrián, S.; Eriksson, A.; Dunlop, T.; Mejhert, N.; Dahlman, I.; Åström, G.; Sjölin, E.; Wåhlén, K.; Carlberg, C.; Laurencikiene, J. Differential effects of 1α, 25-dihydroxycholecalciferol on MCP-1 and adiponectin production in human white adipocytes. Eur. J. Nutr. 2012, 51, 335–342.
- de Souza, W.N.; Norde, M.M.; Oki, É.; Rogero, M.M.; Marchioni, D.M.; Fisberg, R.M.; Martini, L.A. Association between 25-hydroxyvitamin D and inflammatory biomarker levels in a cross-sectional population-based study, São Paulo, Brazil. Nutr. Res. 2016, 36, 1–8.
- Zhang, M.; Gao, Y.; Tian, L.; Zheng, L.; Wang, X.; Liu, W.; Zhang, Y.; Huang, G. Association of serum 25-hydroxyvitamin D3 with adipokines and inflammatory marker in persons with prediabetes mellitus. Clin. Chim. Acta 2017, 468, 152–158.
- Lwow, F.; Bohdanowicz-Pawlak, A. Vitamin D and selected cytokine concentrations in postmenopausal women in relation to metabolic disorders and physical activity. Exp. Gerontol. 2020, 141, 111107.
- O’Sullivan, A.; Gibney, M.J.; Connor, A.O.; Mion, B.; Kaluskar, S.; Cashman, K.D.; Flynn, A.; Shanahan, F.; Brennan, L. Biochemical and metabolomic phenotyping in the identification of a vitamin D responsive metabotype for markers of the metabolic syndrome. Mol. Nutr. Food Res. 2011, 55, 679–690.
- Al-Sofiani, M.E.; Jammah, A.; Racz, M.; Khawaja, R.A.; Hasanato, R.; El-Fawal, H.A.; Mousa, S.A.; Mason, D.L. Effect of vitamin D supplementation on glucose control and inflammatory response in type II diabetes: A double blind, randomized clinical trial. Int. J. Endocrinol. Metab. 2015, 13, e22604.
- Wagner, D.; Hanwell, H.E.; Schnabl, K.; Yazdanpanah, M.; Kimball, S.; Fu, L.; Sidhom, G.; Rousseau, D.; Cole, D.E.; Vieth, R. The ratio of serum 24, 25-dihydroxyvitamin D3 to 25-hydroxyvitamin D3 is predictive of 25-hydroxyvitamin D3 response to vitamin D3 supplementation. J. Steroid Biochem. Mol. Biol. 2011, 126, 72–77.
- Dugar, A.; Hoofnagle, A.N.; Sanchez, A.P.; Ward, D.M.; Corey-Bloom, J.; Cheng, J.H.; Ix, J.H.; Ginsberg, C. The Vitamin D Metabolite Ratio (VMR) is a Biomarker of Vitamin D Status That is Not Affected by Acute Changes in Vitamin D Binding Protein. Clin. Chem. 2023, 69, 718–723.
- Ginsberg, C.; Hoofnagle, A.N.; Katz, R.; Becker, J.O.; Kritchevsky, S.B.; Shlipak, M.G.; Sarnak, M.J.; Ix, J.H. The vitamin D metabolite ratio is independent of vitamin D binding protein concentration. Clin. Chem. 2021, 67, 385–393.
- Herrmann, M.; Farrell, C.-J.L.; Pusceddu, I.; Fabregat-Cabello, N.; Cavalier, E. Assessment of vitamin D status–a changing landscape. Clin. Chem. Lab. Med. (CCLM) 2017, 55, 3–26.
- Schorr, P.; Kovacevic, B.; Volmer, D.A. Overestimation of 3α-over 3β-25-Hydroxyvitamin D3 Levels in Serum: A Mechanistic Rationale for the Different Mass Spectral Properties of the Vitamin D Epimers. J. Am. Soc. Mass Spectrom. 2021, 32, 1116–1125.
- Chen, Y.-C.; He, Y.-Y.; Li, Y.-M.; Wu, B.-T.; Yang, Y.-W.; Feng, J.-F. The importance of analyzing the serum C3-epimer level for evaluating vitamin D storage in some special populations. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5334–5343.
- Bailey, D.; Veljkovic, K.; Yazdanpanah, M.; Adeli, K. Analytical measurement and clinical relevance of vitamin D3 C3-epimer. Clin. Biochem. 2013, 46, 190–196.
- Hazell, T.J.; Gallo, S.; Berzina, l.; Vanstone, C.A.; Rodd, C.; Weiler, H.A. Plasma 25-hydroxyvitamin D, more so than its epimer, has a linear relationship to leaner body composition across infancy in healthy term infants. Appl. Physiol. Nutr. Metab. 2014, 39, 1137–1143.
- Chailurkit, L.; Aekplakorn, W.; Ongphiphadhanakul, B. Serum C3 epimer of 25-hydroxyvitamin D and its determinants in adults: A national health examination survey in Thais. Osteoporos. Int. 2015, 26, 2339–2344.
- Moin, A.S.M.; Sathyapalan, T.; Atkin, S.L.; Butler, A.E. Inflammatory markers in non-obese women with polycystic ovary syndrome are not elevated and show no correlation with vitamin D metabolites. Nutrients 2022, 14, 3540.