Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Omar Cauli and Version 2 by Lindsay Dong.
Peripheral inflammation and gait speed alterations are common in several neurological disorders and in the aging process, but the association between the two is not well established. Biomarkers play an important role in the decision-making process, and IL-6 can be an effective biomarker in establishing the diagnosis of slow gait speed. Further longitudinal research is needed to establish the use of molecular biomarkers in monitoring gait impairment.
- cytokines
- molecular marker
- falls
- IL-6
1. Introduction
Gait velocity is a simple screen of functional status in older adults, and predicts major adverse outcomes in older individuals such as falls, dementia, and death [1][2][3][4][5][6][1,2,3,4,5,6]. A gait speed lower than 0.8 m/s is a reliable cut-off for identifying subjects at increased risk of disability, and evidence on the relationship between circulating IL-6 levels and gait speed suggests that higher IL-6 levels may be associated with poorer performance, hospitalization, institutionalization, and death in older adults [7][8][9][10][11][7,8,9,10,11]. Falls are common in older adults, but little is known about accidental falls and their relationship to movement disorders and chronic inflammation. It has been estimated that adults older than 60 years of age suffer the most fatal falls, therefore as the prevalence of older fallers is predicted to increase with changes in demography, prevention strategies should prioritize fall-related research and establish effective strategies to reduce risk [12]. According to the World Health Organization, approximately 684,000 fatal falls occur each year, making it the second leading cause of unintentional injury death after road traffic injuries [13]. The increasing number of people who suffer falls is also an economic problem for health services worldwide, with an estimated cost for the EU of 25 billion Euros for treating fall-related injuries [14]. In addition, people who have experienced a fall develop fear of falling, which is a serious issue that negatively impacts their physical and mental health [15]. Movement disorders and chronic inflammation are frequently comorbid and underdiagnosed [7]. Systemic inflammation is closely associated with central neuroinflammation [8]. The accessibility and practicality of using blood samples have led to numerous studies measuring the profile of serum or plasma immune markers in several neurological disorders, and many of these studies have found a significant association between those markers and disease severity. Other spatiotemporal parameters, such as a stride length of 0.64 m, accurately predict major adverse events such as physical disability, falls, institutionalization, and mortality [16]. In addition, C-reactive protein (CRP) has been significantly and negatively associated with the total number of daily strides [17].
Previous studies of older adults have linked gait and mobility problems to high CRP levels, and chronic inflammation may be a factor affecting denervation of muscles and changes in the neuromuscular junction [18][19][18,19]. Inflammation also plays a role in the initiation and progression of knee osteoarthritis, and studies have shown that osteoarthritis is associated with high serum levels of inflammatory markers that alter gait mechanism [20][21][22][23][24][25][20,21,22,23,24,25].
Recent developments in drug therapies with biological agents such as anti-tumor necrosis factor alpha (TNF-α), have provided great benefits in terms of reductions in joint inflammation, pain, and improved gait function [26]. Levels of pro-inflammatory cytokines, and in particular, elevated IL-6 and CRP have been identified as independent predictors of impaired mobility, disability, and slow walking speed in older adults [7][19][27][28][29][30][31][32][33][34][35][7,19,27,28,29,30,31,32,33,34,35].
There is growing evidence of associations between elevated levels of inflammatory cytokines such as IL-6, TNF-α, or the acute phase CRP and several chronic health conditions or adverse aging outcomes including muscle loss and cognitive impairment (Figure 1) [34][35][34,35].
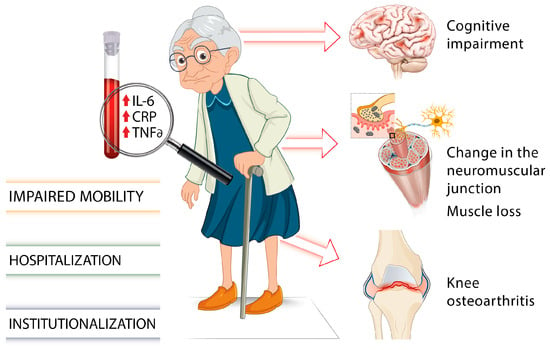
Figure 1. Involvement of proinflammatory markers on gait impairments and frailty in older individuals [7][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][7,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35].
2. Inflammatory Biomarkers and Gait Impairment in Older Adults
2.1. CRP
CRP as an inflammatory marker predictive of decreased gait was the most frequently used study parameter, and was included in 13 of the 21 articles analyzed. High sensitivity CRP (hs-CRP) was used for the relationship with gait parameters in five of them [36][37][38][39][40][43,44,45,48,50].
In one study [41], several groups were categorized according to their initial CRP, taking 1.33 mg/dL as a low value, and 2.7 mg/dL as a high value. Values higher than 2.7 mg/dL were associated with a greater probability of subsequent disability. They were also associated with the following: activities of daily living (ADL), instrumental activities of daily living (IADL), impaired balance, impaired walking speed, and arthritis.
Elevated CRP levels were related to low vitamin D levels [42], with a higher probability of slow walking speed, which was attenuated when vitamin D deficiency was absent, although the relevant factor inducing slow gait was CRP. Another study [43][36] investigated major mobility impairment (MMD) and reported consistent relationships with elevated CRP (>3.0 mg/dL) and a higher risk of MMD, which increased the risk by 38% with a sensitivity of 63% and specificity of 54% as a predictive value over 5 years.
The relationship between CRP and fibrinogen [44][49] with gait speed was studied with 373 people over 20 years, associating the two parameters with gait speed as a single task after adjusting for cardiovascular and risk parameters. However, when executive functions were taken into account, the association with CRP disappeared and the association with fibrinogen was attenuated. Dupont et al. [39][48] used the combination of two parameters, white blood cell count and high-sensitivity CRP, as factors related to the onset of sarcopenia, and observed a negative association with baseline physical activity, quality of life scores, and the SF-36 physical component score in middle-aged and older men. Baseline leukocyte levels were negatively associated with gait velocity, isometric 90° quadriceps and isokinetic peak torque. In another study with 421 participants [45][46], where CRP was related to motor cognitive risk syndrome (MCR), characterized by cognitive complaints and slow gait, patients with higher CRP levels (2.8 mg/dL) had a higher probability of MCR if memory impairment was present.